Abstract
AimEpidemiological studies are important for the prevention and resolution of health problems. We carried out this study to evaluate the incisional and excisional biopsies applied to the nasal skin in the Kırşehir region.MethodsBetween December 2014 and October 2017, 354 patients and 354 lesions were evaluated with a mass on the nasal skin retrospectively. The mean age of the patients, gender distribution, localization of lesions and histopathological type were investigated. These masses were classified as non-neoplastic, benign, premalignant, and malignant.ResultsThe number of females were 226, and the number of males were 128. Age distribution ranged from 9 to 90. There were 20 cases under 18 years old. Premalignant and malignant lesions were not observed in adolescent/pediatric age group. Eighty-two cases over 60 years of age were identified, and 60% of them had a malignant tumor. Nasal skin lesions were more common in the 31-40 age range (24.9%). The most common lesion group was benign tumors (65.2%, n=231), followed by malignant tumors (20.1%, n=71), non-neoplastic lesions (9.6%, n=34) and premalignant lesions (5.1%, n=18). Nevus (175), basal cell carcinoma (67) and chronic nonspecific inflammations (21) were the most common diagnoses. Among the malignant tumors, basal cell carcinoma was diagnosed (67) (M/F:1.09, mean age:65.8) more than squamous cell carcinoma (4). In the patient group with benign tumors, there were vascular tumors (13: capillary hemangioma; 10, hemangioma; 3), verruca vulgaris (12), skin appendage tumors (11: richoepithelioma; 4, trichofolliculoma; 2, steatocystoma; 1 hydradenoma papilliferum; 1, chondroid syringoma; 3), seborrheic keratosis (8), fibroepithelial polyp (7), fibroma (4) and dermatofibroma (1) respectively after nevus. In 18 premalignant lesions, 11 cases were diagnosed as actinic keratosis, and 7 cases were diagnosed as keratoacanthoma.ConclusionThe literature on demographic and histopathological evaluation of nasal lesions is limited. The increase in epidemiological studies can offer a comparative advantage over other studies and can be a guide for health management. Patients with a mass on the nose are required to undergo differential diagnosis with a biopsy.
Keywords
Introduction
The nose is a midfacial organ with great functional and outstanding aesthetic importance. A number of diseases can involve the nose, and some of these can pose special problems at this site.1 They rarely cause mortality, but the quality of life is affected. The external skin of the nose is anatomically separated into vertical thirds; from the glabella (the space between the eyebrows) to the bridge, to the tip. The skin of the upper nose is thick and relatively tensible (flexible and mobile), but then tapers, adhering strongly to the osseocartilaginous framework, and becomes the thinner skin of the dorsal section, the bridge of the nose. The skin overlying the bridge of the mid nose is the thinnest, least tensible, nasal skin since it most adheres to the support framework. The skin of the lower nose is as thick as the skin of the upper nose, because it has more sebaceous glandular structures, particularly at the nasal tip.2
Because the nose is highly exposed to trauma, including ultraviolet (UV) light, skin lesions have a high occurrence rate in this part of the face. UV exposure can also result in cancerous involvement of the skin in a particular area. Due to the protection mechanisms of the body, comprising local inflammatory cells and tumor suppressive genes at the genetic level, the cumulation of UV trauma does not always result in cancer. Also, there are distinct types of UV light with divergent wavelengths, of which UV-A causes reactive oxygen radical formation and UV-B induces mutations, particularly in the p53 gene.3
We present skin lesions classified as non-neoplastic lesions, benign tumors, premalignant lesions, or malignant tumors. A premalignant lesion is the one that is not yet malignant but is expected to turn into a malignant lesion. The most frequent skin lesions of the nose and rare diagnoses, seen in our study are presented, along with our results.
Materials and Methods
Our study was approved by the local ethics committee. We analyzed 354 patients that were histopathologically diagnosed, with the complaint of mass on the nose, retrospectively. The data such as mean age of the patients, gender distribution, localization of lesions, lesions characteristics and histopathological type, were recorded by reviewing the patient files. Data analysis was performed using the SPSS 20.0 program. Descriptive statistics for the evaluation of results are shown as mean, minimum and maximum values, and numbers and percentages of the investigations.
Results
Lesions of the nose are widely distributed in all groups, aged 9 years to 90 years (Table 1). Out of 354 patients studied, nevus was the most common lesion found (49.4%) followed closely by basal cell carcinoma (18.9%).
While inflammatory lesions can affect any age, benign & malignant lesions were more common in older age groups. There were 82 cases (23.2%) in the older age group, and 60% of these had malignant tumors. Females were affected more than males for overall lesions. Females 226: Males 128 (a ratio of approximately 1.77). Lesions of the nose are most common in the age group 31 to 40 years (24.9%).
Melanocytic nevus was the most common diagnosis of the benign tumors (75.8%, n=175). Among 231 benign tumors, 13 were vascular tumors. Age varied from 18 to 74 years, female to male ratio was 3.3:1 (males 3, females 10). 3 out of 13 hemangioma cases were capillary hemangioma. 3 cases were hemangioma. 12 cases were verruca vulgaris, 8 cases were seborrheic keratosis, 7 cases were fibroepithelial polyp, 8 cases were skin appendage tumors (trichoepithelioma; 4, trichofolliculoma; 2, steatocystoma; 1, hidradenoma papilliferum; 1, chondroid syringoma; 3), 4 cases were fibromas, 1 case was dermatofibroma (Table 2).
In premalignant lesions, 11 cases were actinic keratosis (males 3, females 8) and 7 cases were keratoacanthoma (males 6, females 1) (Table 3).
We found 3 patients with chondroid syringoma which is uncommon on the nose. Two of them were male (ages: 64 and 85), 1 of them was female (age: 18).
A total of 67 patients with BCC of the nose were identified. The male-tofemale ratio was 1.09. The mean age of patients was 65.8. The youngest patient was 34 years old; the oldest was 89 years old (Table 4).
Discussion
Nevi of various types can occur on the nose with any size and shape or degree of pigmentation in head and neck region. They are a synonym for the mole to designate a localized abnormality of the melanocytic system. They present with brownish swelling on the nose. Histopathological confirmation is a must since the malignant transformation of melanocytes results in the development of melanoma and benignancy of nevi should be established for treatment of the patient. Junctional nevi are defined as nevi restricted to the basal layer of the epidermis. Histopathologically they occur nests of benign looking nevi cells in the junctional region. These nevi cells are small, round to oval with a darkly stained nucleus and scanty amphophilic cytoplasm.4 In the present study, among all masses of the nose, intradermal nevus was the most common diagnosis (Figure 1).
Lobular capillary hemangioma (LCH) also named pyogenic granuloma is a common, benign, vascular growth of the mucous membrane and skin. LCH occurs in all ages, but more often in the 3rd decade and females. On histological examination, the lobular arrangement of proliferated capillaries surrounded by an edematous fibromixoid stroma with overlying hyperplasic squamous epithelium is seen.5
The squamous papilloma is described identical to verruca vulgaris. Verruca vulgaris, commonly called as a common wart, is one of the most recognizable skin growths and is a benign squamous proliferative lesion caused by human papilloma virus types 1, 2, and 4. It can arise on any epidermal surface of the body but is seen most frequently on the hands and knees.6
Adnexal skin tumors have different histological patterns which distinguish them from other cutaneous tumors. They are mostly distributed in the head, neck, and trunk. Thus, tumors are categorized on adnexa origin: sweat glands, sebaceous glands, and hair follicles of the skin. Tumors of hair follicle included trichoepithelioma (4 cases), characterized microscopically by multiple horn cysts and epithelial tracts connecting abortive pilar structures and a trichofolliculoma (2 cases). The sebaceous tumors include primarily a solitary steatocystoma and one case of hidradenoma papilliferum (HP).7
Hidradenoma papilliferum and chondroid syringoma (CS) are rare, benign tumors of skin appendages. HP is almost exclusively in the vulva or perianal region. Extragenital hidradenoma papilliferum are referred to as “ectopic hidradenoma papilliferum”. Ectopic hidradenoma papilliferum has been reported in 19 people in the English dermatological literature. Though ectopic apocrine glands are normally found in the nose, there has been only one case of ectopic hidradenoma papilliferum arising in nasal skin. The tumor may show a variety of histopathological features including cystic, tubular, papillary or solid pattern. CS is also named as a mixed tumor in respect to epithelial and mesenchymal ingredients. Histopathologically, it resembles benign mixed tumors (pleomorphic adenomas) originating from salivary glands. The incidence is less than 0,01% of primary skin neoplasms.8-9 We found 3 CS patients in our series (Figure 2).
About 80% of all BCC occur on the face, of these tumors 25% to 30% are found on the nose. BCC is the most common non-melanoma skin cancer of this region. Most commonly, a carcinoma of the nose is a basal cell carcinoma, and a squamous cell carcinoma commonly arises from the dorsum of the nose10-11 (Figure 3,4,5).
Squamous cell carcinomas are malignant tumors that account for one-fourth of total squamous cell carcinomas on head and neck region. Squamous cell carcinomas of the nose are primarily a disease of older males who are exposed to sunlight for a prolonged period. Squamous cell carcinoma is the second most common cancer of the external nose with an incidence of 11% (basal cell carcinoma being most common with an incidence of 87%). SCC is thought to arise from keratinizing or Malpighian epithelial cells. The hallmark of squamous cell carcinoma is the presence of keratin or keratin pearls on the histologic study. These were well-formed desmosome attachments and intracytoplasmic bundles of keratin tonofilaments. Histopathological features of squamous cell carcinoma remain important for the clinician, as they carry prognostic value and help to define the most appropriate treat ment for patients 11 (Figure 6). In Kırsehir region, people have outdoor jobs such as farming. Farmers are exposed to more solar UV radiation and chemical agents than individuals in other occupations. There may be an association with BCC and SCC.
Actinic keratosis (AK) is a common skin disease that is triggered by long-term sun exposure, and it typically forms on the face, neck, balding scalp, chest, shoulders, the back of arms and hands of adults; 75% of all reported lesions present on the head, neck, and forearms. AK is characterized by the formation of keratotic macules, papules, or plaques with superficial scales on a red base, which are classified based on histological findings. Some AK lesions can undergo malignant transformation and progress to invasive squamous cell carcinoma (SCC).12
The differentiation of keratoacanthoma from SCC is very important because both lesions have similar pathologic appearances. A unique clinical property of keratoacanthoma is its rapid growth (within weeks). These lesions generally originate from hair follicles or the superficial epithelium and measure 1-3 cm in diameter. However, the lesions undergo spontaneous resolution within several months.3 Epidermal cysts are usually composed of epidermal elements that are implanted into the dermal layers. They should be differentiated first from trichilemmal cysts by histopathological features. Trichilemmal cysts show specific keratinization without a granular layer (Figure 7). Fibrous papules are dense benign papules, 1-5 mm, that are usually located at the alar parts and the tip of the nose. It is significant to differentiate these lesions from basal cell carcinoma, which also has a pearl-like appearance.3 Papules are also reported as complications of piercing (Figure 8).
Leishmaniasis is spread by the bite of female phlebotomine sand flies and associated with migration of populations from developing countries because of wars and poverty. The disease begins as an erythematous papule at the site of the sandfly bite on exposed parts of the body. The papule increases in size and becomes a nodule. It eventually ulcerates and crusts over. Histologically, amastigotes are seen in monocytes or extracellularly. It is important to see the nucleus and the rod-shaped kinetoplast, a mitochondrial structure containing extranuclear DNA, to diagnose leishmaniasis.13 (Figure 9).
Regardless of whether or not they are malignant, nasal skin lesions can yield important cosmetic defects that should be evaluated carefully before processing any curative or corrective intervention. Any disease that affects the face and nose mostly depends on ultraviolet exposure. As a result of heterogeneity of skin lesions of the nose, proper education of general practitioners, as well as otorhinolaryngologists, is compulsory. Excision biopsy with histopathological study becomes mandatory for confirmation of diagnosis.
In conclusion, nose mass can occur in any age or sex. Inflammatory lesions are more common in children and adolescent. Benign tumors affect middle age people while malignant tumors affect older age group. Females are affected more than males for overall lesions.
Non-neoplastic, benign, premalignant, and malignant lesions affect the external nose. Non-neoplastic and benign lesions are more common than malignant lesions. In non-neoplastic lesions; cysts (epidermal, dermoid, trichilemmal) are the most common lesions, closely followed by inflammatory lesions (folliculitis).
In premalignant lesions, actinic keratosis and keratoacanthoma were found in 18 patients.
Benign lesions comprise 65.2% of cases. Malignant lesions comprise 21% of cases. Basal cell carcinomas are the most common malignant lesions (94.4%).
Many times, clinicians may have the false impression for diagnosis of masses, that can only be corrected by histopathology.
Declarations
Informed Consent
Informed consent was obtained from all participants.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
None.
References
- Lakshmi DV, Shilpa K, Nataraja HV, Divva KG. Nose: applied aspects in dermatology. Indian J Dermatol. 2016;61(2):234. doi:10.4103/0019-5154.177782
- McCullouch TM, Van Daele DJ. Normal anatomy and physiology of the nose, the pharynx, and the larynx. In: Langmore SE, ed. Endoscopic evaluation and treatment of swallowing disorders. New York, NY: Thieme; 2001:7-36.
- Yigider AP, Kayhan FT, Yigit O, Kavak A, Cingi C. Skin diseases of the nose. Am J Rhinol Allergy. 2016;30(3):83-90. doi:10.2500/ajra.2016.30.4318
- Silverberg SG, DeLellis RA, Frable WJ, LiVolsi VA, Wick MR. Silverberg’s principles and practice of surgical pathology and cytopathology. Vol 2. 4th ed. New York, NY: Churchill Livingstone; 2006:2267-2284.
- Ozcan C, Apa DD, Gorur K. Pediatric lobular capillary hemangioma of the nasal cavity. Eur Arch Otorhinolaryngol. 2004;261(8):449-451.
- Kim SJ, Byun SW, Lee SS. Various tumors in the nasal vestibule. Int J Clin Exp Pathol. 2013;6(12):2713-2718.
- Samaila MOA. Adnexal skin tumors in Zaria, Nigeria. Ann Afr Med. 2008;7(1):6-10. doi:10.4103/1596-3519.55691
- Smith FB, Shemen LJ, Guerrieri C, Ismail SS. Hidradenoma papilliferum of nasal skin. Arch Pathol Lab Med. 2003;127:86-88. doi:10.5858/2003-127-e86-hpon
- Yılmaz F, Koybaşı S, Gürel K, Boran C. Chondroid syringoma. KBB Forum. 2005;4(3):147-149.
- Wollina U, Bennewitz A, Langner D. Basal cell carcinoma of the outer nose: overview on surgical techniques and analysis of 312 patients. J Cutan Aesthet Surg. 2014;7(3):143-150. doi:10.4103/0974-2077.146660
- Mishra A, Nagle SK, Oberoi V, Jagade MV, Kasbekar V. Squamous cell carcinoma of nose: an unusual presentation. Clin Rhinol. 2011;4(3):166-167. doi:10.5005/jp-journals-10013-1103
- Chetty P, Choi F, Mitchell T. Primary care review of actinic keratosis and its therapeutic options: a global perspective. Dermatol Ther. 2015;5(1):19-35. doi:10.1007/s13555-015-0070-9
- Markle WH, Makhoul K. Cutaneous leishmaniasis: recognition and treatment. Am Fam Physician. 2004;69(6):1455-1460.
Tables
Table 1. Age wise distribution of the cases
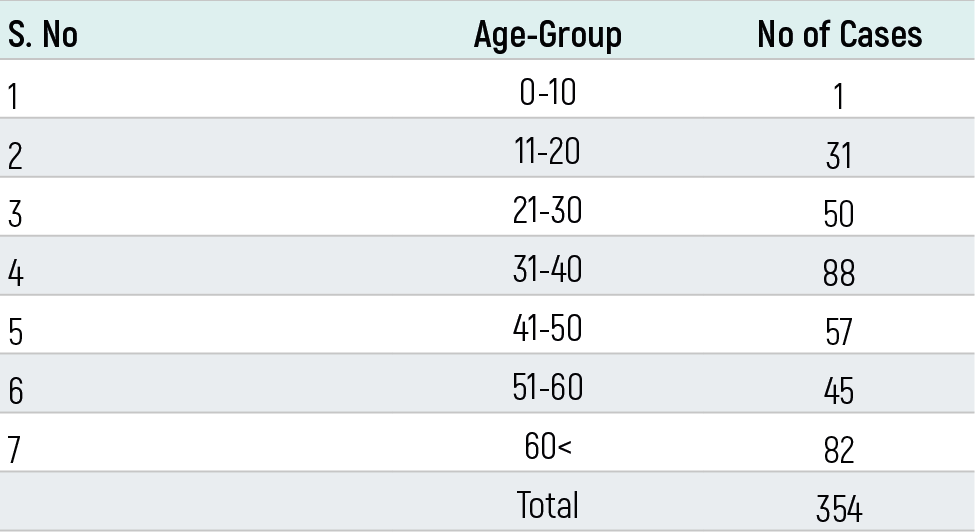
Table 2. Incidence of benign tumors

Table 3. Incidence of premalignant lesions

Table 4. Incidence of malignant tumors

Figures
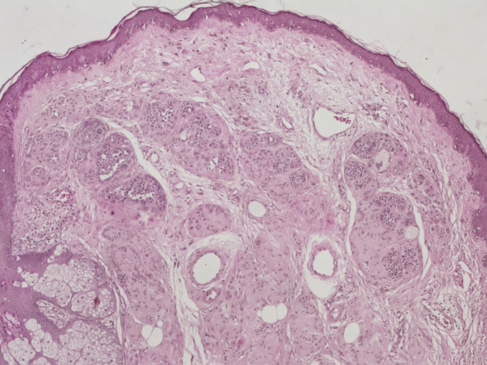
Figure 1. Intradermal nevus (H&E, X50)
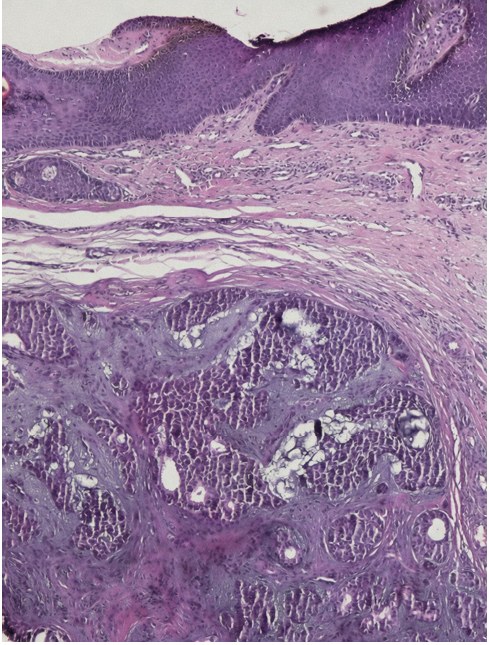
Figure 2. Chondroid syringoma (H&E, X50)

Figure 3. Nodular basal cell carcinoma lesions

Figure 4. Nodular basal cell carcinoma lesions
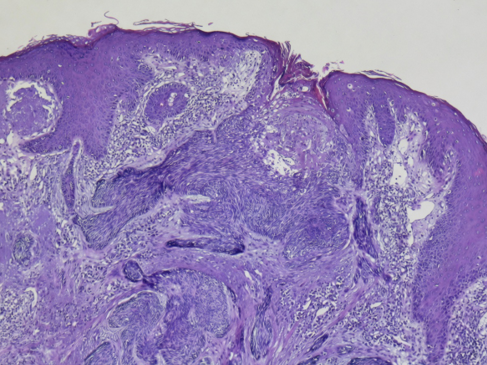
Figure 5. Basal cell carcinoma (H&E, X50)
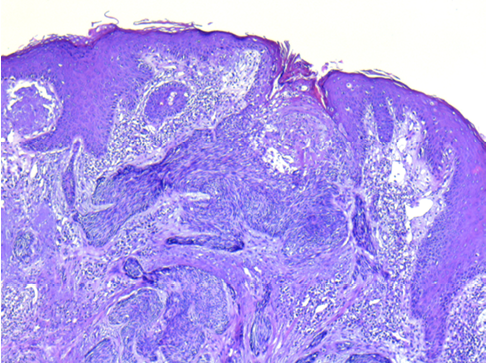
Figure 6. Squamous cell carcinoma (H&E, X100)
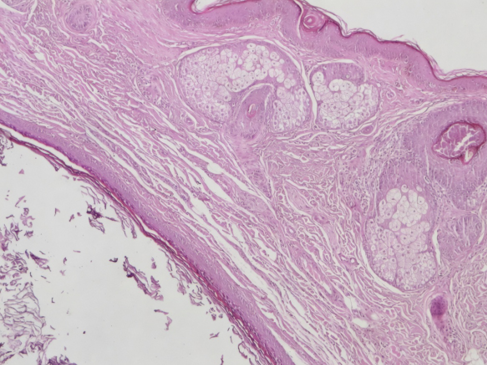
Figure 7. Epidermal cyst (H&E, X50)

Figure 8. Papule on the nose in a patient after piercing usage

Figure 9. Cutaneous leishmaniasis on the nasal dorsum of an immigrant patient
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Asuman Kilitci, Yücel Çiçek, Ersoy Acer, Emine Müge Acar. Analysis of nasal skin biopsies: 354-case series. Eu Clin Anal Med 2018;6(1):4-8. doi:10.4328/ECAM.123
- Received:
- 21.12.2017
- Accepted:
- 02.01.2018
- Published Online:
- 07.01.2018
- Printed:
- 07.01.2018