Abstract
AimIn this retrospective report, the foreign body findings in adult patients with chronic cough were aimed to explore.MethodsBetween October 2011 and May 2017, patients with bronchial foreign body aspirations mistakenly diagnosed as COPD or asthma in outside centers were collected. The bronchoscopic and clinical findings of four patients with chronic cough were found from the archieve of the hospital.ResultsThe age of the patients who applied to our clinic ranged from 27 to 64 years. Endobronchial foreign bodies were successfully removed with FOB in all patients. The extracted foreign bodies were stone, headscarf needle, a needle-like object and a foil paper.ConclusionIn adults with chronic cough foreign body aspiration should be immediately taken into account.
Keywords
Introduction
Cough is the symptom of all chronic respiratory system diseases and some non-respiratory system pathologies, as well as the normal protective mechanism of airways. It is one of the most common reasons for referral to a doctor. Chronic cough term is used to describe coughs that last longer than eight weeks. Despite the approaches of published guidelines, treatment of chronic cough is still not as successful as desired.1 Foreign body aspiration is very rarely seen in healthy adults Foreign body aspirations can be seen in elderly, in alcohol and sedative drug users, in neurological diseases, during epileptic seizures, due head trauma and general anesthesia, and rarely in healthy adults. Tablet forms of medicines, small metal or plastic parts, foods, turban needles, tracheostomy cannula are foreign bodies reported as aspiration reasons in the literature. Apart from this, cases in which teeth or instruments of dental treatments were aspirated have also been reported in the literature.1-2 Foreign body aspirations may lead to acute symptoms such as asphyxia, sudden breathlessness and cough, as well as late complications due to diagnostic delays, such as chronic breathlessness like asthma and COPD, hemoptysis, pneumonia, atelectasis, and bronchiectasis. Foreign body aspirations can be detected during the examination of such cases. Our study was retrospective. We examined 4 adults with foreign body aspiration who had different diagnoses and treatments due to chronic cough in the external centers and was referred to our clinic.
Materials and Methods
Our study was planned retrospectively by examining the patients who underwent fiberoptic bronchoscopy. The study was conducted with reference to our retrospective patient information. Between October 2011 and May 2017, 311 cases who underwent fiberoptic bronchoscopy were examined retrospectively. Foreign body aspirations were detected with FOB in cases of unresolved chronic cough, who applied to our clinic. The characteristics of the patients have been studied. Among them, bronchial foreign body aspirations were detected. Bronchial aspiration should be investigated and considered in patients with unresolved chronic cough. In addition, we emphasized the importance of fiberoptic bronchoscopy in cases of chronic cough that did not improve or were not relieved clinically.
Results
Between October 2011 and May 2017, bronchial foreign body aspirations were mistakenly diagnosed as COPD or asthma in other health centers. The age of the patients who applied to our clinic ranged from 27 to 64 years. Endobronchial foreign bodies were successfully removed with FOB in all patients. Images of endobronchial foreign bodies detected by fiberoptic bronchoscopy are shown in the pictures. Separate case the informations is as follows:Our cases with chronic coughing and endobronchial foreign bodies were composed of 4 individuals.Case ReportA 64-year-old man with chronic cough, sputum, shortness of breathlasting for four consecutive years and fever in the last week, stated that he was previously completely healthy. The patient stated that he had gone into a crisis of wheezing and coughing due to aspiring something while eating rice four years ago, but he was relieved after swallowing and did not refer to the doctor initially. On following days, chest x-ray taken due to cough and shortness of breath was said to be normal. The patient was given bronchodilator medication for COPD. Despite using long-acting beta-2 agonist and anticholinergics for four years, he had a history of uncomfortable breathing, wheezing, feeling of something stuck in the throat and coughing. The patient went to the general surgery clinic of our hospital first because of the feeling of something stuck in the throat and there was no pathology. The patient was referred to our clinic by the general surgeon because of his respiratory complaints. The body mass index of the patient was 37.2. On physical examination, blood pressure was 115/85 mmHg, pulse rate was 86/min, respiratory rate was 22/min, oxygen saturation was 94% in room air and fever was 36.6 Co degrees. During auscultation localized wheezing was noted in the lower right lung. A homogeneous intensity increase was observed in the right lower area of chest x-ray. Hemogram and biochemical findings were normal. Mild obstruction was observed in pulmonary function tests: FEV1: 1.86 liters (67%), FVC: 2.15 liters (68%), FEV1/FVC: 68.6%, PEF:3.75 (66%) and FEF25-75: 1.7 liters (62%). Flexible bronchoscopy was applied to the patient for diagnostic and therapeutic purposes with preliminary diagnosis of foreign body aspiration. The removed foreign body turned to be a stone. It was observed that the complaints of the patient disappeared in the periodic follow-ups after the procedure. PA chest X-ray showed a homogeneous intensity increase with paracardiac placement, which did not erase the right atrium border (Fig. 1) Foreign body (stone) image with flexible bronchoscope (Figure 2)Case Report 2A 34-year-old woman with chronic cough, sputum, shortness of breath lasting for two consecutive years and fever in the last week, stated that she was previously completely healthy. Two years ago, when the patient threw a piece of paper she was playing into her mouth as a joke, she had gone into a crisis of wheezing and coughing due to aspiring something, but she was relieved after swallowing and did not refer to the doctor initially. On following days, chest x-ray taken due to cough and shortness of breath was said to be normal. The patient was given bronchodilator medication for asthma. Despite using long-acting beta-2 agonist and inhaled corticosteroids for two years, she had a history persistent dyspnea, wheezing, feeling of something stuck in the throat and coughing. The patient who was referred to our pulmonology polyclinic was evaluated by us. On physical examination, blood pressure was 110/70 mmHg, pulse rate was 94/min, respiratory rate was 23/min, oxygen saturation was 93% in room air and fever was 37.3 Co degrees. During auscultation localized wheezing was noted in the lower right lung. A homogeneous intensity increase was observed in the right lower area of chest x-ray. Hemogram and biochemical findings were normal. Mild obstruction was observed in pulmonary function tests: FEV1: 1.76 liters (65%), FVC: 1.95 liters (68%), FEV1/FVC: 68.8%, PEF: 3.45 (66%) and FEF25-75: 1.46 liters (64%). Flexible bronchoscopy was applied to the patient for diagnostic and therapeutic purposes with preliminary diagnosis of foreign body aspiration. The removed foreign body bi FOB turned to be a foil paper (Figure 3). The patient was clinically relieved after the procedure.Case Report 3A 27-year-old woman with chronic cough, sputum, shortness of breath lasting for two consecutive years and fever in the last week, stated that she was previously completely healthy. Two years ago, when the patients was wearing a headscarf needle in her mouth, she had gone into a crisis of hoarseness, wheezing and coughing due to aspiration, but she was relieved in a short while and did not refer to the doctor initially. Approximately 3 months later, she was diagnosed with asthma. Bronchodilator medication was given to the patient for asthma. Despite using long-acting beta-2 agonist and inhaled corticosteroids, she had a history persistent dyspnea, wheezing and coughing. The patient who was referred to our pulmonology polyclinic was evaluated by us. On physical examination, blood pressure was 120/80 mmHg, pulse rate was 74/min, respiratory rate was 27/min, oxygen saturation was 92-3% in room air and fever was 37.0 Co degrees. During auscultation localized wheezing was noted in the lower right lung. A homogeneous intensity increase was observed in the right lower area of chest x-ray. Hemogram and biochemical findings were normal. Mild obstruction was observed in pulmonary function tests: FEV1: 1.66 liters (63%), FVC: 1.90 liters (67%), FEV1/FVC: 67.6%, PEF: 3.35 (63%) and FEF25-75: 1.36 liters (60%). Flexible bronchoscopy was applied to the patient for diagnostic and therapeutic purposes with preliminary diagnosis of foreign body aspiration. The removed foreign body bi FOB turned to be a headscarf needle. The patient was clinically relieved after the procedure.Figure 4 shows the endobronchial settlement of the headscarf needle as a foreign body.Case Report 4A 29-year-old woman with chronic cough, sputum, shortness of breath lasting for two and a half consecutive years, stated that she was previously completely healthy. Two and a half years ago, when the patients accidently took a wire into her mouth at work and aspired due to carelessness, she had gone into a crisis of hoarseness coughing, but she was relieved in a short while and did not refer to the doctor initially. Approximately 3 months later the patient developed dyspnea and she was diagnosed with asthma by a specialist. Bronchodilator medication was given to the patient for asthma. Despite using asthma medications she had a history persistent dyspnea, wheezing and coughing. The patient who was referred to our pulmonology polyclinic was evaluated by us. On physical examination, blood pressure was 130/70 mmHg, pulse rate was 76 /min, respiratory rate was 28/min, oxygen saturation was 94% in room air and fever was 37.0 Co degrees. During auscultation localized wheezing was noted in the lower right lung. A homogeneous intensity increase was observed in the right lower area of chest x-ray. Hemogram and biochemical findings were normal. Mild obstruction was observed in pulmonary function tests: FEV1: 1.55 liters (59%), FVC: 1.77 liters (63%), FEV1/FVC: 85%, PEF: 3.15 (60%) and FEF25-75: 1.28 liters (58%). Flexible bronchoscopy was applied to the patient for diagnostic and therapeutic purposes with preliminary diagnosis of foreign body aspiration. The removed foreign body bi FOB turned to be a needle like object. The patient was clinically relieved after the procedure. Figure 5 shows the endobronchial foreign body image.
Discussion
Foreign body aspiration can lead to early and late findings. Because foreign body aspirations cause early complaints such as stridor, cough, hoarseness, shortness of breath, diagnosis and treatment is usually done early. It has been reported that in 21.8% of the cases diagnosis was delayed longer than 30 days.3 Diagnosis requires advanced methods in cases of aspiration disregard or unawareness.4-5 Especially in the elderly and with delayed diagnosis of aspiration, severe complications such as shortness of breath, chronic cough, pneumonia, atelectasis can follow. Therefore, it is very important to reliably remove the tracheobronchial foreign object diagnosed by flexible or rigid bronchoscopy. In patients suspected of foreign body presence, it is important to confirm the diagnosis by further examination and bronchoscopy as well as detailed physical examination and chest x-ray. All of our cases who referred to our clinic were adult patients with foreign body aspirations who had different diagnoses and treatments due to chronic cough in other health institutions. In adults, the right main bronchus shows wider angulation with the trachea. Foreign body aspirations are more frequent in the right endobronchial system,6 because foreign bodies follow a flatter path from larynx to the right main bronchus than
the left. In all of our cases bodies were in the right bronchial system. Rigid bronchoscopy and flexible bronchoscopy are successfully used in the diagnosis and treatment of foreign body aspiration cases. Baharloo et al,7 performed 103 rigid and 9 flexible bronchoscopies in a foreign body case series of 121 patients without any complications. In recent years, rigid bronchoscopy has been replaced by flexible bronchoscopy due to its advantages such as reaching more distal parts of the tracheobronchial system and not requiring general anesthesia. Danado et al.,8 used flexible bronchoscopy in %95 of 56 patients and did not encounter any complications. Rigid bronchoscopy was used only in two patients and only one of them required surgical treatment. Swanson et al.,9 have successfully removed foreign bodies with flexible bronchoscopy in the majority of pediatric patients. In the presented case, flexible bronchoscopy was performed without the need for rigid bronchoscopy and thoracotomy with the help of stapled forceps. Foreign bodies in all of our 5 cases were successfully removed by flexible bronchoscopy. Complications associated with foreign bodies of mechanical stenosis in the airways are: bronchiectasis, atelectasis, lung abscess, pneumothorax, pneumomediastinum, hemoptysis, recurrent respiratory infections and reactive granulation tissue formation. Foreign bodies structural features, location in the tracheobronchial system, delay in diagnosis and treatment play a role in the development of such complications.10 In adult patients with non-specific symptoms such as chest pain and dyspnea when foreign body aspiration can not be understood with anamnesis, radiopaque objects such as prosthetic dentition can be easily detected in chest x rays taken during routine examination.11 Flexible bronchoscopy was used for both diagnosis and treatment in our entire 5 cases. Normal radiographic findings can be seen in 6-80%. Patient with nonspecific history, clinical and radiological findings should undergo thoracic computed tomography examination. In most of the cases; foreign body itself, lobar/segmental hyperlucency due to air trapping, bilateral air trapping, total lung opacity, atelectasis and parenchymal consolidation, heterogeneous or homogeneous increase of density in lung graft may be seen radiographically.4-5 All of our 5 endobronchial foreign body aspiration cases’ chest x-rays showed a homogenous increase of density in the lower right lung area. As a result; in adult patients with persistent cough, foreign body aspirations should be considered. Flexible bronchoscopy is a highly effective and safe method for diagnosing and removing foreign bodies.12 History, physical examination, radiology and other laboratory examinations are often sufficient to consider foreign body aspirations. Chest X-ray is widely used to support aspiration of foreign body. Sensitivity of radiological findings range from 63% to 96%.13 Chest X-ray and radiological examination are important for foreign body aspirations. In some of our cases, the findings on the chest x-ray when combined with a history of aspiration led to the pre diagnosis of foreign body. In a study conducted in our country Gürsu et al.,14 in a population of 33 foreign body aspirations, has emphasized that 77.4% aspirates were inorganic objects and 64.5% of them were beaded pins. Chronic cough describes coughs that last longer than eight weeks. In adults the prevalence of chronic cough, which is a common and quite inconvenient complaint, has been reported to be 3-40%.14 In all of our cases, there were cough complaints that lasted longer than 8 weeks. In a study in China, in patients with FBA chronic cough was the most common symptom with 67%. Other symptoms included: hemoptysis 23%, fever 19% and dyspnea 16%.15 Patients who had aspirated foreign bodies and have not noticed at the time, referred to hospitals later on, and for that reason received corticosteroids and antibiotics. These treatments hide the symptoms of foreign bodies and may eventually lead to lung parenchyma loss. A careful anamnesis, good physical examination, suspicion of foreign body aspiration facilitates diagnosis and treatment. The treatment of tracheobronchial foreign body aspiration is to remove the foreign body. Prior to 1970’s, rigid bronchoscopy was used for it, but FOB became popular in later years.16 As in our cases, if foreign body aspiration is suspected, bronchoscopy should be planned. Another important point is that, while rigid bronchoscopy is usually performed by many physicians in bronchial foreign body aspiration, our study shows that flexible bronchoscopy is a safe and effective diagnostic and treatment method. Foreign body bronchial aspiration may be encountered, but the detection and presentation of foreign bodies in those with chronic cough is of special importance.
Declarations
Informed Consent
Informed consent was obtained from all patients included in the study.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
None.
References
- Morice AH, Fontana GA, Sovijarvi AR, et al. The diagnosis and management of chronic cough. Eur Respir J. 2004;24(3):481-492. doi:10.1183/09031936.04.00027804
- Cherniack RM. Current therapy of respiratory disease. Hamilton, ON: BC Decker; 1986.
- Saquib Mallick M, Rauf Khan A, Al-Bassam A. Late presentation of tracheobronchial foreign body aspiration in children. J Trop Pediatr. 2005;51(3):145-148. doi:10.1093/tropej/fmh103
- Ozdemir A, Cosentino CM, Siwik SA, Wilfond BS. Radiological case of the month: orange seed aspiration. Arch Pediatr Adolesc Med. 1998;152(9):921-922. doi:10.1001/archpedi.152.9.921
- Tokar B, Ozkan R, Ilhan H. Tracheobronchial foreign bodies in children: importance of accurate history and plain chest radiography in delayed presentation. Clin Radiol. 2004;59(7):609-615. doi:10.1016/j.crad.2004.01.006
- Dikensoy O, Usalan C, Filiz A. Foreign body aspiration: clinical utility of flexible bronchoscopy. Postgrad Med J. 2002;78(921):399-403. doi:10.1136/pmj.78.921.399
- Baharloo F, Veyckemans F, Francis C, et al. Tracheobronchial foreign bodies: presentation and management in children and adults. Chest. 1999;115(5):1357-1362. doi:10.1378/chest.115.5.1357
- Donado Una JR, de Miguel Poch E, Casado Lopez ME, Alfaro Abreu JJ. Fiberoptic bronchoscopy in extraction of tracheobronchial foreign bodies in adults. Arch Bronconeumol. 1998;34(2):76-81.
- Swanson KL, Prakash UB, Midthun DE, et al. Flexible bronchoscopic management of airway foreign bodies in children. Chest. 2002;121(5):1695-1700. doi:10.1378/chest.121.5.1695
- Pogorzelski A, Zebrak J, Pawlik J, Cherian Z, Buchwald J. Bronchopulmonary complications due to aspiration of foreign bodies in children. Pediatr Pol. 1995;70(4):325-331.
- Karadas S, Gönüllü H, Sayır F, Aydın İ. A rare cause of dyspnea in elderly patients: foreign body aspiration. J Clin Anal Med. 2012;3(4):466-468.
- Cunanan OS. The flexible fiberoptic bronchoscope in foreign body removal: experience in 300 cases. Chest. 1978;73(5):725-726. doi:10.1378/chest.73.5.725
- Hoeve LJ, Rombout J, Pot DJ. Foreign body aspiration in children: the diagnostic value of signs, symptoms and preoperative examination. Clin Otolaryngol. 1993;18(1):55-57. doi:10.1111/j.1365-2273.1993.tb00810.x
- Ege E, Demirdogen E. Chronic cough: definition, prevalence, algorithmic management. Turkiye Klinikleri J Immunol Allergy Spec Top. 2009;2(1):1-3.
- Chen CH, Lai CL, Tsai TT, Lee YC, Perng RP. Foreign body aspiration into the lower airway in Chinese adults. Chest. 1997;112(1):129-133. doi:10.1378/chest.112.1.129
- Lan RS, Lee CH, Chiang YC, Wang WJ. Use of fiberoptic bronchoscopy to retrieve bronchial foreign bodies in adults. Am Rev Respir Dis. 1989;140(6):1734-1737. doi:10.1164/ajrccm/140.6.1734
Figures

Figure 1. Chest X-ray film of Case 1
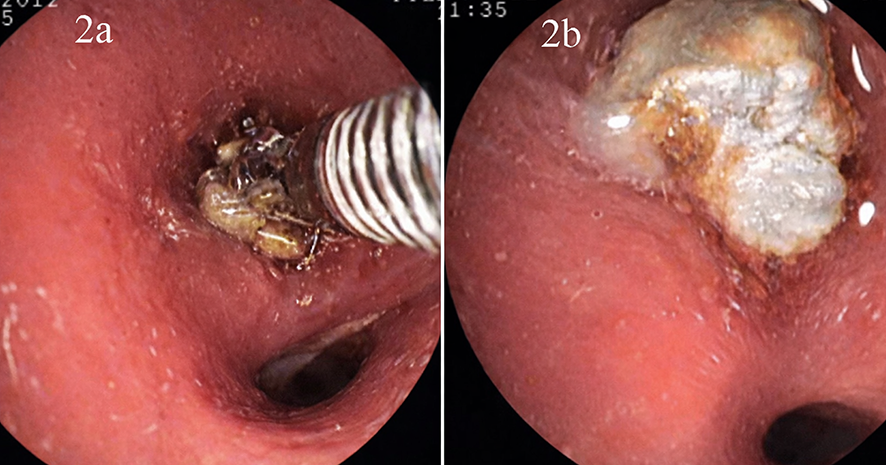
Figure 2. Foreign body (stone) images with flexible bronchoscope (2a, 2b) in Case 1.
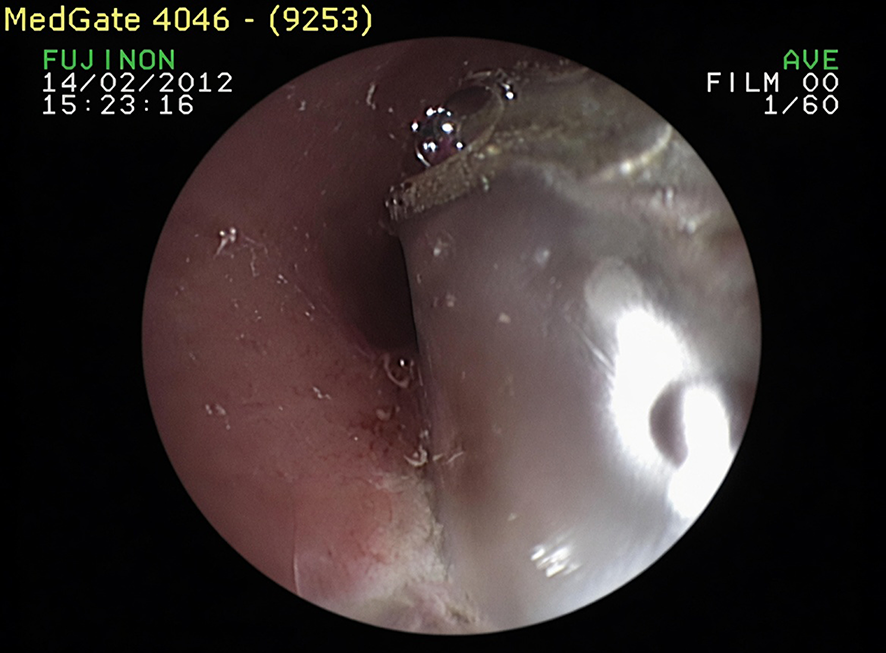
Figure 3. The foreign body (foil paper) in Case 2.
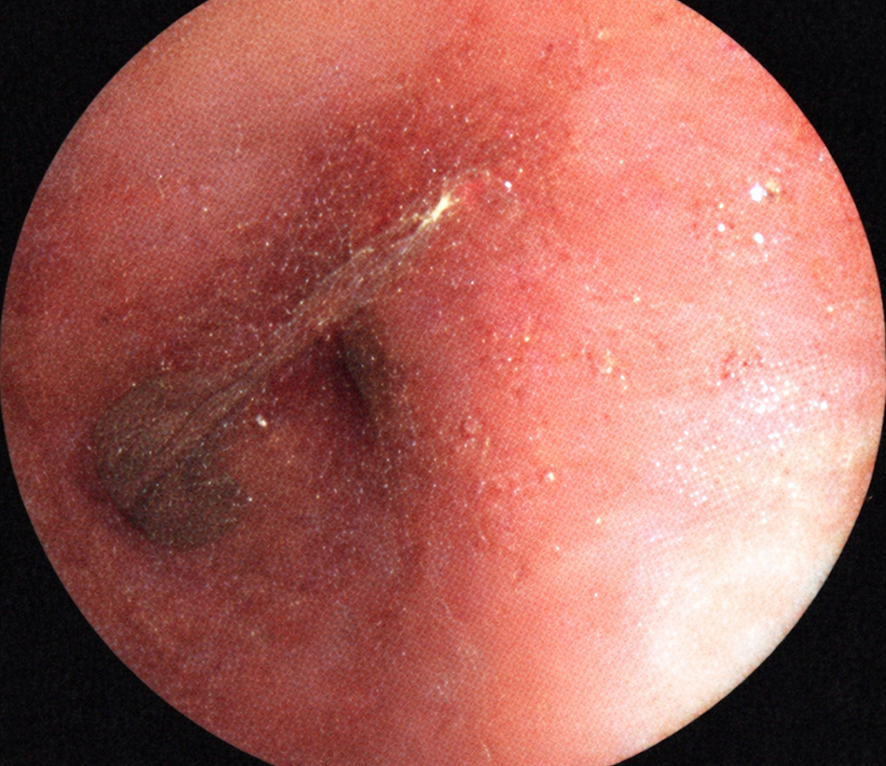
Figure 4. Endobronchial settlement of the headscarf needle as a foreign body in Case 3.

Figure 5. Endobronchial foreign body image in Case 4.
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Suat Konuk, Hikmet Çoban. Endobronchial foreign body aspirations causing chronic cough and dyspnea. Eu Clin Anal Med 2026;6(2):9-13. doi:10.4328/ECAM.125
- Received:
- 24.02.2018
- Accepted:
- 14.03.2018
- Published Online:
- 15.03.2018
- Printed:
- 01.05.2018