Abstract
AimWe aimed to investigate glomerular filtration rate (GFR) observed during the painful crisis and 15 days after the painful crisis of sickle cell anemia (SCA) patients.MethodsA total of 38 patients with SCA were included in the study. 25 of these patients were male, and 13 were female. The amount of creatinine and albumin in urine in 24 hours and serum creatinine level were determined during and after 15 days from SCA painful crisis. In the patients, the creatinine clearance was measured during and after 15 days from SCA painful crisis.ResultsIn SCA patients, the average creatinine clearance during the painful crisis was determined as 136.0 ± 80.0 mL / min, after 15 days from the painful crisis, the average creatinine clearance was determined as 124,8 ± 53,4 ml/min (44,9-238,3). In SCA patients, there was no significant difference between the creatinine clearance calculated during the painful crisis and 15 days after the painful crisis (p>0,05). In SCA patients, during the crisis, the amount of albuminuria was 199.5 ± 408.3 mg/day (2.6-1943) while it was determined 167.0 ± 399.7 mg/day (5.7-1944.9) after 15 days of the crisis. There was no statistically significant difference between albuminuria during and 15 days after the crisis.ConclusionIn SCA patients, there was no significant difference between the creatinine clearances calculated during and 15 days after the SCA painful crisis. SCA patients were found to have decreased albuminuria 15 days after the crisis.
Keywords
Introduction
Sickle cell anemia (SCA) is a disease that affects many systems with hereditary transmission and is a clinical condition that has arisen because of red blood cells contain altered hemoglobin S (HbS). HbS occurs as a result of the single point mutation and substitution of the glutamic acid in position 6 of the β-globin chain with valine namely because adenine is replaced by thymine in DNA. SCA is due to ischemic injury and chronic hemolysis caused by the clogging of small blood vessels of clinical findings. Painful crises are most common in SCA patients and cause patients to contact emergency services. Painful crises are called acute vasoocclusive crises because microvascular vessels become clogged with erythrocytes shaped like a sickle and resultin ischemic tissue damage.1-2The vasoocclusive events involving the kidneys are frequent but usually, do not show symptoms. There are structural and functional abnormalities in the kidneys in SCA patients. All these changes are visible from the glomeruli to the tip of the papillary along the nephron. The medullar region of the kidney is composed of renal tubules and medullary blood vessels. The kidney’s oxygen consumption is high. Renal medulla is acidic, hypertonic and hypoxic sensitive. As a result of getting the shape of sickle of erythrocyte, vasoocclusions develops and causes hypoxia. In HbS polymerization and in getting the shape of sickle of erythrocyte, in medulla dysfunction can be found out. Although young patients with SCA have normal kidney function tests, hypertrophy develops. As age progresses, it may progress to end-stage renal failure (ESRD).3-4
Materials and Methods
This study was performed in 38 patients (13 women and 25 men) who applied to Mustafa Kemal University Medical Faculty Research Hospital and Antakya State Hospital with SCA painful crisis between May 2008 and October 2009. In patients, during a painful crisis and 15 days after a painful crisis, serum creatinine, hemogram, ferritin, complete urine analysis and creatinine and albumin were counted in the 24-hour urine. During a painful crisis and 15 days after a painful crisis, it was calculated by the of GFR creatinine clearance of the patients. Patients received hydration, opioid, nonopioid analgesic bleaching during the crisis and some patients received antibiotic treatment. Patients with previously known renal disease, hypertension, and diabetes mellitus were excluded from the study.Serum creatinine and urine creatinine was found with Beckman Coulter Synchron LX20 device, albumin excretion in urine was found with Beckman Coulter device By nephelometer method, serum ferritin was found with Beckman Coulter UniCelDxI 800device by Immunoassay method, urine test was carried out with Automatic Urine AnalyzerLabUMat&Urised - Complete Urine Analyzer and hemoglobin and haematocrit Coulter ® Gen·S™. Albumin excretion in the urine was <30 mg/day normal, 30-300 mg/day microalbuminuria and > 300 mg/day macroalbuminuria. The patient was asked how many times the SCA had suffered the crisis each year. Patients were divided into SCA less than three and more than three per year according to crisis frequency. Statistics Analysis In the analysis of the statistical data, version number 15 of “SPSS for Windows” package program was used. In the patients, Kolmogorov-Smirnov test was used to determine whether the continuous variables were normally distributed. In comparing the number of crises below three or three per year, Mann-Whitney test was used. Statistical significance limit was taken as p<0,05.Results
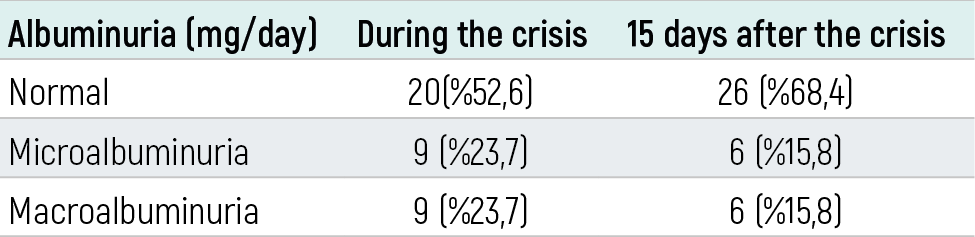
The average age of the patients was found as 25.0 ± 9.3 (11-48). A total of 38 patients, 65.8% were male, and 34.2% were female. The median age of 23 patients who had more than three SCA crises was 22, the median age of 15 patients who underwentless than three crises was 28 years. There was no significant difference between age distribution (p> 0,05). In SCA patients, average serum creatinine values during the painful crisis was 0,54±0,25mg /dl (0,20–1,6), average serum creatinine levels after 15 days from the painful crisis was 0,60±0,21mg/dl (0,30–1,30). There was no difference between the serum creatinine 15 days after and during SCA painful crisis (p>0,05). In SCA patient, average creatinine clearance during the crisis was found as 136,0±80,0 ml/min (23,9–362,9). After 15 days from the crisis, the mean creatinine clearance was found as 124,8±53,4 ml/min (44,9–238,3). Between the crisis and 15 days after the crisis, there was no statistically significant difference between creatinine clearances. During the crisis, serum creatinine level was higher in only one patient from 14 patients who had creatinine clearance <90 ml/min. After 15 days of the crisis, serum creatinine level was higher in only one patient among 12 patients who had creatinine clearance <90 ml/min, others were normal. Accordingly, in SCA patients, GFR should be measured if serum creatinine levels are low or normal. In the study, after the crisis, serum creatinine levels increased in 21 patients, decreased in 11 patients, and not changed in 6 patients. During the crisis, tubular secretion may be slightly elevated, though not significant. More extensive work should be done for this. The laboratory data of the patients are as given in table 1.During the SCA crisis, the average creatinine clearance rate of patients who had less than three crises was 146,9 ml/min, the average creatinine clearance rate of patients who had more than three crises was 128,9 ml/min. There was no significant difference between the two groups (p> 0.05). The creatinine clearance average rate of patients who have had less than three crises 15 days after the crisis was 104,7 ml/min, the creatinine clearance average rate of patients who have had more than three crises was 137,9 ml/min. There was no significant difference between the two groups (p> 0.05). There was no relationship between crisis frequency and GFR. It was found that those who had less than three crises had a decline in GFR after the crisis. It was seen that those who had more than three crises increased GFR after the crisis. When hyperfiltration is considered as (> 140 ml / min), 39.5% during the crisis and 34.2% after 15 days from the crisis. Also, in our patients, GFR was calculated by Modification of diet in renal disease (MDRD). According to this, a significant difference was found between MDRD and creatinine clearance calculated 15 days after the crisis (p<0,05). However, it was higher than that the GFR creatinineclearance calculated by MDRD. (MDRD clearance 179.5 ml / min, creatinine clearance 124.8 ml / min). In our study, during the crisis, there were albuminuria in 47.3% (18 patients) of the patients, the average age of the patients was 27.2. Microalbuminuria was detected in 23.7%, and macroalbuminuria was detected in 23.7% of these patients. Albumin excretion of urinary SCA patients 15 days after crisis and during the crisis is given in table 2. After 15 days from the crisis, 31.5% of them had albuminuria. Microalbuminuria in 15.8% of those patients and macroalbuminuria in 15.8% of those patients was found. Fifteen days after the crisis, eight of the patients were switched from microalbuminuric phase to normoalbuminuric phase, four from macroalbuminuric phase to microalbuminuric phase, one from microalbuminuric phase to macroalbuminuric phase and two patients from normoalbuminuric phase to microalbuminuric phase. During the crisis, albuminuric was detected in 60% of the patients who had less than three crises and albuminuria was detected in 39,1% of the patients who had more than three crises. 15 days after the crisis, 46.6% of the patients who had less than three crises identified as albuminuric, 21.7% of the patients who had less than three crises identified as albuminuric. Also in our patients, we found an increase in albumin excretion with age. While The average creatinine clearance of 18 albuminuric patients during the crisis was 157,1±89,0 ml/min and the average age was 27.2, average creatinine clearance of 20 non-albuminuric patients was 117,0±67,8 ml/min, and the average age was 23. There was no significant difference in creatinine clearance between these two groups (p>0.05). 15 days after the crisis, while the average creatinine clearance of 12 albuminuric patients was 136,1±53,2 ml/min and the average age was 27.4, average creatinine clearance of 26 non-albuminuric patients was 119,6±53,0 ml/min, and the average age was 23.8. There was no significant difference in creatinine clearance between these two groups (p>0.05). There was no statistical significance between creatinine clearance and albuminuria, but creatinine clearance was higher in patients who had albuminuria. In our study, no haematuria was detected in any of the patients.Discussion
SCA is associated with structural and functional renal abnormalities (such as hematuria, proteinuria, papillary necrosis, urinary concentration defects, renal tubular acidosis, acute renal damage, end-stage renal failure and medullary carcinoma).5-6 In patients with SCA, chronic renal disease (CKD) is at high risk for development. Loss of kidney function depends on chronic complications of SCA (such as anemia, hemolysis, and inflammation). During the SCA vasoocclusive crisis, acute renal injury (AKI) development is common. It is unclear whether recurrent AKI in patients with SCA during vasoocclusive crises is a potential factor for the development of CKD. However, recent studies have shown a relationship between recurrent AKI and CKD progression.7-8-9
In a study by Guasch et al., albuminuria was observed in 300 adult patients (184 HbSS and 116 other hemoglobinopathies). Albumin excretion in urinary patients with HbSS was found to be 68%, and macroalbuminuria was found to be 26%. After the age of 40, macroalbuminuria was found to be 40%. It has been shown that the likelihood of developing albuminuria has increased over the years. There is no relationship between anemia and albuminuria.10 In a study by AamerAlem et al. with 73 patients of SCA, proteinuria in 41% of patients (30 patients) and proteinuria in nephrotic levels were found to be 4%.11 In a study by Falk et al., In 381 patients with SCA, proteinuria frequency was found as 26% (101 patients). Proteinuria was detected in nephrotic levels in 12% of these proteinuria patients.12 In a study of 142 SCA patients between 21 months and 20 years of age by Patricia et al., the frequency of microalbuminuria was found to be 19%. Increased age and lower hemoglobin levels were found to correlate.13 In a study of 150 patients, microalbuminuria was found to be 18.5% in patients with SCA with an average survival rate of 8.8 ± 6.4.14 In another study, microalbuminuria was found to be 60.9%, and macroalbuminuria was found to be 2.5%.15 In our study, average albumin excretion was similar to other studies. Crisis frequency did not correlate with albumin excretion. After the crisis in 27 patients, a decrease in albuminuria and increase in albuminuria after the crisis in 11 patients were detected. The increase in the amount of albuminuria during the crisis may be due to increased perfusion. More work is needed in this regard.
In a study of 73 patients, serum creatinine levels were higher in only two patients. Serum creatinine levels were low in 28 of the patients. Serum creatinine levels were normal in 7 of 12 patients with low creatinine clearance.11 In a study by Falk et al., serum creatinine levels were found to be above normal in 7% (26) of 381 SCA patients.12 Similar results were obtained in our patients. Serum creatinine level was high in 5% of our patients (2 patients).
Renal papillary necrosis is a common complication of SCA. It is associated with hematuria, but it is not always accompanied by haematuria. The haematuria of the SCA may be of any age and is more common in SCA carriers.16 In the study of 73 SCA, hematuria was detected in 7 patients.11 In our study, hematuria was not detected in patients. CKD is common in adults with SCA. SCA affects glomerular and tubular functions. Microalbuminuria and glomerular hyperfiltration are the primary signs of renal dysfunction. Glomerular hyperfiltration is common in pediatric patients. It is also frequently observed in adults. Glomerular hyperfiltration is defined as 130ml / min for women and 140ml / min for men. CKD EPI GFR was 135,1 ml / min (112-154,4) and glomerular hyperfiltration rate was 49,5%.15 In a study conducted, the prevalence of CKD was found to be 39.2 (31.6% of CKD prevalence in children and 68.4% in adults).Glomerular hyperfiltration was found to be 68.8% in children and 31.2% in adults. The GFR was 136 ml/min in the 136 HbSS cases and 119 ml/min in the HbSC cases.17 In one study, GFR was 124.2 ml / min.18 In the study conducted in adults, HbSS GFR 138ml / min (109-153) HbSC 119ml / min (95-137).19 In another study of adults, CKD stage 3-5 6%, glomerular hyperfiltration 24.5%.20 In our study, glomerular hyperfiltration was detected at 39.5% during the SCA painful crisis andv34.2% after 15 days of the crisis.
As a result, renal diseases develop in SCA patients. Glomerular hyperfiltration is increased during the crisis in SCA patients, but there is no statistically significant difference when compared to after the crisis. There was no significant difference between GFR after SCA crisis and crisis. There was no significant correlation between SCA painful crisis and GFR and albuminuria. The frequency of SCA crisis has been found to decrease with age. Albuminuria was found to increase with age. Recent studies have emphasized that patients with acute renal failure are at increased risk for the development of chronic kidney disease in the future if they have complete remission. This has also been shown in SCA patients. It is, therefore, necessary to carry out wider work.
Declarations
Informed Consent
Written informed consent was obtained from all participants included in the study.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
None.
References
- Quinn CT. Sickle cell disease in childhood: from newborn screening through transition to adult medical care. Pediatr Clin North Am. 2013;60(6):1363-1381. doi:10.1016/j.pcl.2013.09.006
- Steinberg MH. Predicting clinical severity in sickle cell anemia. Br J Haematol. 2005;129(4):465-481. doi:10.1111/j.1365-2141.2005.05411.x
- Stuart MJ, Nagel RL. Sickle cell disease. Lancet. 2004;364(9442):1343-1360. doi:10.1016/s0140-6736(04)17192-4
- Scheinman JI. Sickle cell disease and the kidney. Nat Clin Pract Nephrol. 2009;5(2):78-88. doi:10.1038/ncpneph1008
- Alkhunaizi AM, Al-Khatti AA. Proteinuria in patients with sickle cell disease. Saudi J Kidney Dis Transpl. 2014;25(5):1038-1041. doi:10.4103/1319-2442.139931
- Nath KA, Hebbel RP. Sickle cell disease: renal manifestations and mechanisms. Nat Rev Nephrol. 2015;11(3):161-171. doi:10.1038/nrneph.2015.8
- Basile DP. The endothelial cell in ischemic acute kidney injury: implications for acute and chronic function. Kidney Int. 2007;72(2):151-156. doi:10.1038/sj.ki.5002312
- Chawla LS, Eggers PW, Star RA, Kimmel PL. Acute kidney injury and chronic kidney disease as interconnected syndromes. N Engl J Med. 2014;371(1):58-66. doi:10.1056/nejmra1214243
- Baddam S, Aban I, Hilliard L, et al. Acute kidney injury during a pediatric sickle cell vaso-occlusive pain crisis. Pediatr Nephrol. 2017;32(8):1451-1456. doi:10.1007/s00467-017-3623-6
- Guasch A, Navarrete J, Nass K, Zayas CF. Glomerular involvement in adults with sickle cell hemoglobinopathies: prevalence and clinical correlates of progressive renal failure. J Am Soc Nephrol. 2006;17(8):2228-2235. doi:10.1681/asn.2002010084
- Aamer A. Renal abnormalities in patients with sickle cell disease: a single center report from Saudi Arabia. Saudi J Kidney Dis Transpl. 2008;19(2):194-199.
- Falk RJ, Scheinman J, Phillips G, et al. Prevalence and pathologic features of sickle cell nephropathy and response to inhibition of angiotensin-converting enzyme. N Engl J Med. 1992;326(14):910-915. doi:10.1056/nejm199204023261402
- McBurney PG, Hanevold CD, Hernandez CM, et al. Risk factors for microalbuminuria in children with sickle cell anemia. J Pediatr Hematol Oncol. 2002;24(6):473-477. doi:10.1097/00043426-200208000-00013
- Aloni MN, Mabidi JL, Ngiyulu RM, et al. Prevalence and determinants of microalbuminuria in children suffering from sickle cell anemia in steady state. Clin Kidney J. 2017;10(4):479-486. doi:10.1093/ckj/sfx058
- Geard A, Pule GD, Chetcha CB, et al. Clinical and genetic predictors of renal dysfunctions in sickle cell anaemia in Cameroon. Br J Haematol. 2017;178(4):629-639. doi:10.1111/bjh.14724
- Oksenhendler E, Bourbigot B, Desbazeille F, et al. Recurrent hematuria in white patients with sickle cell trait. J Urol. 1984;132(6):1201-1203. doi:10.1016/s0022-5347(17)50097-x
- Ephraim RK, Osakunor DN, Cudjoe O, et al. Chronic kidney disease is common in sickle cell disease: a cross-sectional study in the Tema Metropolis, Ghana. BMC Nephrol. 2015;16(1):75. doi:10.1186/s12882-015-0072-y
- Drawz P, Ayyappan S, Nouraie M, et al. Kidney disease among patients with sickle cell disease, hemoglobin SS and SC. Clin J Am Soc Nephrol. 2016;11(2):207-215. doi:10.2215/cjn.03940415
- Novelli EM, Hildesheim M, Rosano C, et al. Elevated pulse pressure is associated with hemolysis, proteinuria and chronic kidney disease in sickle cell disease. PLoS One. 2014;9(12):e114309. doi:10.1371/journal.pone.0114309
- Asnani MR, Reid ME. Renal function in adult Jamaicans with homozygous sickle cell disease. Hematology. 2015;20(7):422-428. doi:10.1179/1607845414y.0000000213
Tables
Table 1. Patient’s laboratory data

Table 2. Albumin excretion during idiopathic SCA crisis and after 15 days
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Can Huzmeli, Edip Uçar, Ali Borazan, Hasan Kaya. Changes in renal functions of sickle cell anemia patients during and afterpainful crisis. Eu Clin Anal Med 2026;5(3):45. doi:10.4328/ECAM.119
- Received:
- 10.08.2017
- Accepted:
- 20.08.2017
- Published Online:
- 01.09.2017
- Printed:
- 01.09.2017