Abstract
IntroductionStump appendicitis is defined as re-inflammation of residual appendix tissue after incomplete appendectomy. Clinically, it presents with acute abdominal pain. Early diagnosis is vital for avoiding potential complications. A history of appendectomy lowers clinical suspicion and increases morbidity. Stump appendicitis should be considered as the diagnosis in patients with appendectomy presenting with lower right quadrant pain and signs of peritonitis.Case PresentationIn this paper, we report a 51-year-old patient who was admitted to emergency department with signs of acute abdomen and diagnosed with stump appendicitis at laparoscopic examination 1 month after undergoing laparoscopic appendectomy operation.ConclusionIn addition to patient history and physical examination, abdominal tomography plays an important role in the diagnosis of stump appendicitis.
Keywords
Introduction
Appendectomy is one of the most commonly performed surgical procedures worldwide. As a result of its huge worldwide volume, it is typically associated with quite variable and frequent complications. Stump appendicitis is a rare, albeit highly fatal and morbid, late complication of appendectomy.1 Unless diagnosed early in the course, it may lead to a variety of complications such as gangrenized stump, perforation, intraabdominal abscess, and peritonitis. Therefore, stump appendicitis should definitely be considered in the differential diagnosis in patients presenting to emergency department with acute abdomen who also have a history of appendectomy operation.2 In this paper, we report a rare case of stump appendicitis presenting with signs of acute abdomen 1 month after undergoing laparoscopic appendectomy operation.
Discussion
Stump appendicitis was first described by Rose in 1945. It is a condition with potential life-threatening complications.1 Early diagnosis is crucial for avoidance of potential morbidity and mortality. Stump appendicitis, a rare complication of appendectomy (1/50000), may occur weeks or even years after appendectomy operation.3 In our patient, it took approximately 1 month for stump appendicitis to emerge. The current increase in the incidence of stump appendicitis most likely results from making an improper appendiceal dissection and leaving an appendiceal stump longer than 5 mm. An unduly long stump functions as a reservoir for fecaliths that eventually obstruct appendiceal stump lumen, precipitating complications.4 A stump longer than required may remain at the end of a procedure due to a subserous or retrocecal appendiceal location or surgical inexperience.1 Emergency physicians and general surgeons should be aware of and vigilant for stump appendicitis, and this condition should be considered in the differential diagnosis of patients presenting with lower right quadrant pain. A delay in diagnosis prolongs duration of hospital stay. Pain initially emerges around umbilicus and then it migrates to lower right quadrant; and it is also accompanied by loss of appetite and nausea. A clinical picture typical of appendicitis is usually present.5 Our patient also presented with a clinical picture typical of appendicitis.Radiological examinations are central to the workup for stump appendicitis, with ultrasonography and tomography being the main, effective imaging tools in suspected cases. Ultrasonography, with its ability to define lesions, is the initial imaging tool of choice although it yields non-specific findings. On the other hand, computed tomography can provide clinicians with more valuable information. Thickening of intestinal wall in pericecal region, changes compatible with abscess formation, and fluid collection in paracolic region are particularly helpful for making a diagnosis of stump appendicitis.1 Tomography showed a tubular structure compatible with both an abscess and an inflamed appendix in our patient. It has been reported that 68% of appendicites operated for acute abdominal pain are perforated. Duration of hospital stay is longer in stump appendicitis compared with acute appendicitis since the former’s diagnosis is delayed; the reported mean duration of hospital stay is 9 days.6 Our patient had an abscess in pericecal region at the laparoscopic examination and she was discharged seven days after the operation. There exists no standardized treatment approach for stump appendicitis. Either appendectomy is completed by laparoscopic or open technique or appendix stump is resected.4 Some studies have even reported that a conservative management without surgery can be implemented.7 In our case, the abscess was drained and appendectomy was completed by laparoscopic technique. In conclusion, stump appendicitis should definitelybe considered in the differential diagnosis of patients presenting with lower right quadrant pain and signs of peritonitis who have a clinical presentation suggestive of acute appendicitis even when they have a previous appendectomy operation. Such asceptic clinical attitude is vital for being able to make an early diagnosis.
Declarations
Informed Consent
Informed consent was obtained from all participants.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
None.
References
- Onder A, Kapan M, Böyük A, Tekbaş G, Gümüş M. Stump appendicitis after appendectomy. Kolon Rektum Hast Derg. 2010;20(4):188-191.
- Menteş O, Zeybek N, Oysul A, Onder SC, Tufan T. Stump appendicitis, rare complication after appendectomy: report of a case. Ulus Travma Acil Cerrahi Derg. 2008;14(4):330-332.
- Constantin V, Popa F, Carâp A, Socea B. Stump appendicitis: an overlooked clinical entity. Chirurgia (Bucur). 2014;109(1):128-131.
- Roberts KE, Starker LF, Duffy AJ, Bell RL, Bokhari J. Stump appendicitis: a surgeon’s dilemma. JSLS. 2011;15(3):373-378. doi:10.4293/108680811x13125733356954
- Truty MJ, Stulak JM, Utter PA, Solberg JJ, Degnim AC. Appendicitis after appendectomy. Arch Surg. 2008;143(4):413-415. doi:10.1001/archsurg.143.4.413
- Al-Dabbagh AK, Thomas NB, Haboubi N. Stump appendicitis: a diagnostic dilemma. Tech Coloproctol. 2009;13(1):73-74. doi:10.1007/s10151-008-0419-5
- Rios RE, Villanueva KM, Stirparo JJ, Kane KE. Recurrent (stump) appendicitis: a case series. Am J Emerg Med. 2015;33(3):480. doi:10.1016/j.ajem.2014.08.050
Figures

Figure 1. An axial section demonstrates heterogeneity of mesentery and a tubular structure with a size of approximately 2 cm that contains oral contrast material within at the anterior aspect of cecal floor in the lower right quadrant.
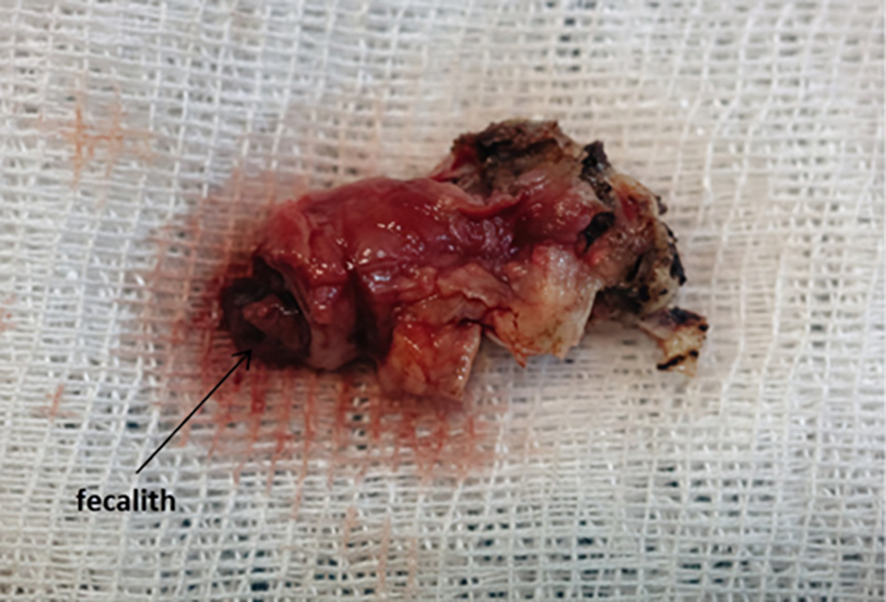
Figure 2. The view of the stump appendix resected intraoperatively.
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Mehmet Tolga Kafadar, Metin Yalaza, Gürkan Değirmencioğlu. A rare complication after laparoscopic appendectomy (stump appendicitis): A Case Report. Eu Clin Anal Med 2026;4(1):9-11. doi:10.4328/ECAM.66
- Received:
- 27.11.2015
- Accepted:
- 14.12.2015
- Published Online:
- 01.01.2016
- Printed:
- 01.01.2016