Abstract
AimThe treatment strategy for tibial fractures differs with fracture location, displacement, soft tissue condition and comminution. Intramedullary nailing is considered the gold standard treatment for tibial fractures.MethodsIn this study, the functional and radiographic results of tibial shaft fractures repaired with the inflatable intramedullary nail method were evaluated.ResultsFrom 2013 to 2015, 17 patients (10 males, 7 females; 8 right, 9 left; mean age 40.7 years) with closed tibial fractures repaired with inflatable intramedullary nails were assessed. The time from injury to surgery was an average of 2 days (range, 0–6 days). The mean time of hospital stay was 6 days (range, 2–19 days). The mean follow-up time was 15.4 months (range, 9–25 months). The mean time for patients to return to normal daily activities was 4.5 months (range, 4–6 months). The mean operation time was 47.5 min (range, 35–80 min). None of the patients had major perioperative or postoperative complications such as deep vein thrombosis, fat embolism, infection, or neurovascular complications except for the occurrence of delayed union in one patient. Only 4 patients had anterior knee pain and ankle pain during the early postoperative period. ConclusionInflatable intramedullary nails seem to be safe and effective in the treatment of tibial AO/OTA type A and B midshaft fractures.
Keywords
Introduction
Tibial fractures are the most common long bone fractures with an annual incidence of 2 in 1000.1-2 The treatment strategy for tibial fractures differs with fracture location, displacement, soft tissue condition and comminution.1 Conservative treatment is the most common strategy; however, in adults, displaced and communited fractures are usually surgically repaired. Plate and screws, external fixators and intramedullary nails are used in surgery.2-3 Intramedullary nailing is considered the gold standard treatment for tibial fractures.2-3-4 Intramedullary nailing has many advantages such as minimal invasiveness, rapid fracture stabilisation, early mobilisation and weight bearing and it can be used either with a locked or unlocked system.2-3-4 The hydraulically expandable nail consists of an expandable stainless steel tube with four reinforcement bars connected by thin folded stainless steel membranes, with a conical distal end. Normal saline is injected into the hollow inner core of the nail under pressure through a proximal valve to expand it and increase its effective diameter.5-6-7-8 The inflatable intramedullary nail has some advantages such as easy application, short surgical time and less exposure to radiation.5 However, proximal displacement of the nail, malunion, and the frequent requirement of additional treatment such as cast fixation, most especially rotational instability, are the drawbacks of this method.6-7-8-9 In this study, the functional and radiographic results of tibial shaft fractures repaired with inflatable intramedullary nail method were evaluated.
Materials and Methods
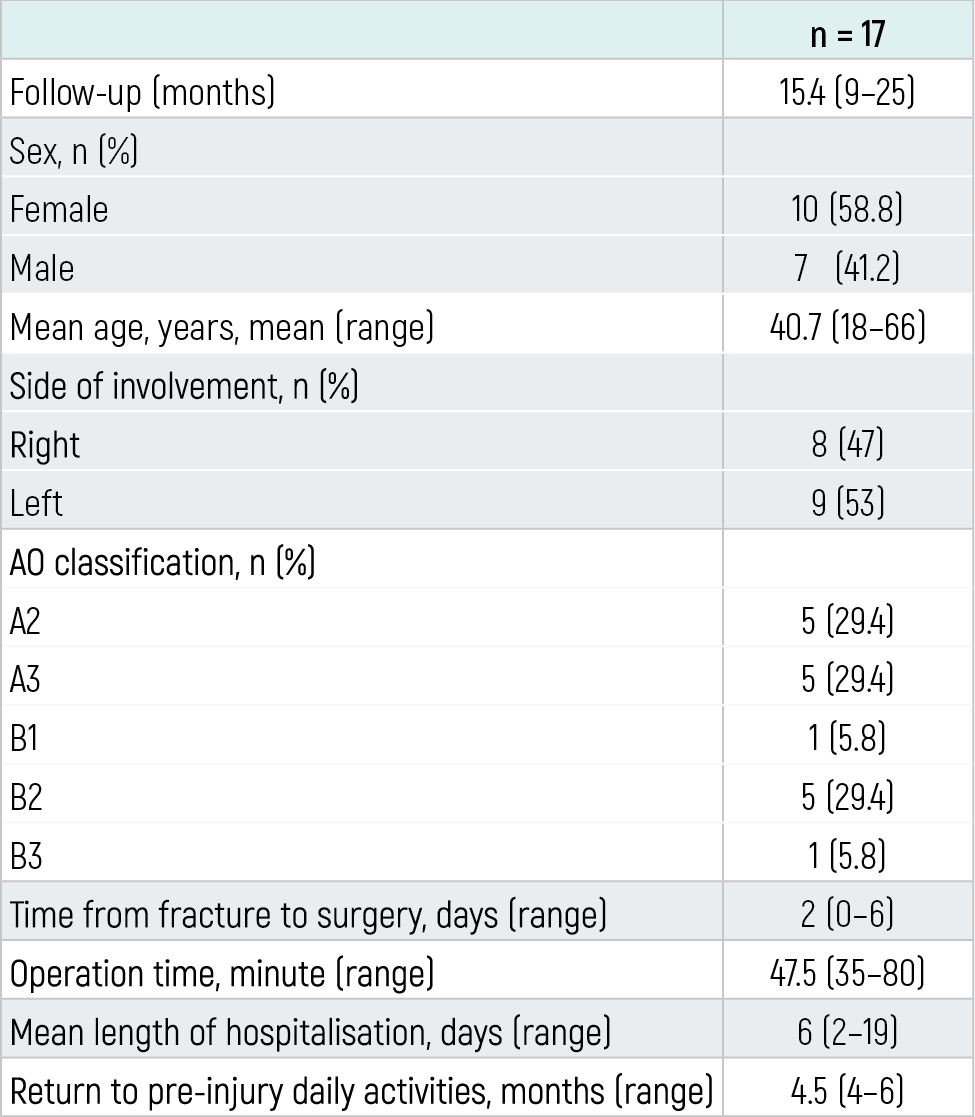
From 2013 to 2015, 17 patients (10 males, 7 females; 8 right, 9 left; mean age 40.7 years; range 18–66 years) with closed tibial fractures repaired with inflatable intramedullary nails (Fixion® IM Nail, Dic-O-Tech, St. Herzliya, Israel) were evaluated retrospectively in this study. The character
istics of the patients are presented in Table 1.The patients were administered a short leg plaster splint for 3 weeks postoperatively. The splint was then removed and partial load bearing was allowed so long as the patients could tolerate. Quadriceps exercises for the knee joint and ankle exercises were started. After 1.5 months, the patients were allowed full load bearing.At the last follow up, all the patients were evaluated radiologically for bone union. In addition, the patients were investigated for the presence of pain, infection, neurovascular disorders and deformities (varus/valgus, anteversion/recurvatum, rotation and shortening).
This study was conducted in accordance with the principles of the Declaration of Helsinki and an informed consent was obtained from each patient.
Results
Patient fractures were classified according to the AO/OTA classification as follows: A2 in 5 (29.4%), A3 in 5 (29.4%), B1 in 1 (5.9%), B2 in 5 (29.4%), and B3 in 1 (5.9%).The most common cause of injury was traffic accident in 12 cases (70.8%) while 5 (29.2%) of fractures were fall-related. Two patients also had fractures in other extremities. The mean time from injury to surgery was 2 days (range, 0–6 days). The mean time of hospital stay was 6 days (range, 2–19 days). The mean follow-up time was 15.4 months (range, 9–25 months). The mean time for patients to return to normal daily activities was 4.5 months (range, 4–6 months). The mean operation time was 47.5 min (range, 35–80 min) (Figure 1).None of the patients had major perioperative or postoperative complications such as deep vein thrombosis, fat embolism, infections, or neurovascular complications except the occurrence of delayed union in one patient (5.8%). For this, a second surgery was performed to support the fractured side by autogenous bone graft and full union was achieved at the end of follow-up (Figure 2). Only 4 (23.5%) patients had anterior knee pain and ankle pain during the early postoperative period. However, the pains spontaneously resolved 12 weeks postoperatively.
Discussion
Today, intramedullary nailing has become the gold standard procedure for closed shaft fractures of long bones.2-3,6-7 Reamed intramedullary nails provide more rigid fixation by increasing the bone contact surface; however, the reaming process disrupts the endosteal blood supply.2,5,8 In addition, the increase of intramedullary pressure can lead the oil cysts, lipids and medullary waste, which interfere with blood circulation and may result in cardiopulmonary complications.3,5-6 Reamed intramedullary nails provide faster healing by stimulating internal local bone graft supply while reaming.5,7-8 Thus, in cases such as nonunion and implant failure, it has been emphasised that reamed intramedullary nails are superior to unreamed nails.5,7-8 The application of unreamed inflatable intramedullary nails may lead to nail-specific complications such as nonunion and implant failure, which also occur with unreamed intramedullary nails.1,5,9-10 Inflatable intramedullary nails have advantages for unions as a system allowing axial compression; however, for metadiaphyseal region fractures and multi-part fractures, collapse and shortness may occur, resulting in instability.1,5,9-10 In our study, 10 patients had AO type A tibial fractures and 7 patients had type B.On the other hand, the inflatable nail is ideal for diaphyseal involvement.9 Lepore et al.10 treated 43 patients with the inflatable nail and compared them with a matched cohort treated with statically locked nails. They concluded that the inflatable nail allows for effective management of diaphyseal fractures of the femur and that interlocking was unnecessary. In addition, operation times are reduced and fluoroscopy exposure is minimized. Some authors prefer inflatable intramedullary nails, particularly in osteoporotic patients.11 because they support the idea that drilling the cortex several times while inserting the distal screws weakens the cortex and may cause the cut out of the screw.11-12 Compared to locked intramedullary nails, inflatable intramedullary nails do not provide sufficient stability for multi-part unstable fractures and also have less resistance against the rotational forces of transverse fractures.1-2,5,9,12 Blomquist et al. in their biomechanical study on cadavers found that inflatable intramedullary nails had high bending stiffness and low torsional strength as compared with locked intramedullary nails. They also reported that inflatable intramedullary nails made slippage movement during torsional tests.1 It can be difficult to remove the nail during a second surgery when a deformity occurs on the nail during osteosynthesis. In this study, we did not identify any problems such as nonunion, nail breakage or bending during follow up. Patients were administered a short leg plaster splint for 3 weeks postoperatively to prevent rotational failure. None of our patients had nonunion. Upon the detection of delayed union in one patient, a secondary surgery supporting the fractured side by autogenous bone graft was performed and full union was achieved at the end of follow-up without any complaints.In some studies, it was observed that the bars surrounding the inflatable intramedullary nails, which make contact with the medulla, achieve multiplanar stability. The surface area of the nail was increased in axial section after the expansion of the nails.1,5,13 In addition, inflatable intramedullary nails are superior to interlocking intramedullary nails in terms of the frequency of bending but are comparable in terms of rotational stiffness.1,5 The most important advantages of the inflatable intramedullary nails are shortening of surgical time and reducing the exposure of fluoroscopy dose.4-5,8-9,14 In our study, we determined the mean operation time as 47.5 min. In similar studies for tibia fractures; Kapoor et al.4 reported the mean operation time as 55 min, Smith et al.14 reported this as 41 min, while Fortis et al.15 reported an average operation time of 40 min.In our study, the mean time for patients to return to normal daily activities was 4.5 months. In the literature, we observed similar results in the healing time of fractures repaired using expandable IM nails. Ghafi et al.12 reported a mean healing time of 3.9 months, Kaapor et al.4 reported 4.8 months, while Serbest et al.16 reported 4.2 months.This study has some limitations. First, it was retrospective. Second, our sample size and follow-up time were small. Third, we did not use any clinical scoring systems for patient satisfaction. Moreover, there was no control group with locked IM nailing system against which to compare our results. In summary, inflatable intramedullary nails seem to be applicable, safe and effective for tibial AO/OTA type A and B midshaft fractures. The non-use of locking screws and reaming minimized the operation time. In cases of multiple injuries that require rapid intervention, the use of inflatable intramedullary nails may be appropriate. However, it must be considered that inflatable intramedullary nails may fail to provide sufficient stability for metaphyseal and multi-part fractures.
Declarations
Informed Consent
Informed consent was obtained from all participants.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
None.
References
- Blomquist J, Lundberg OJ, Gjerdet NR, Molster A. Are inflatable nails an alternative to interlocked nails in tibial fractures? Clin Orthop Relat Res. 2008;466(5):1225-1231. doi:10.1007/s11999-008-0169-8
- Petrisor BA, Bhandari M, Schemitsch EH. Tibia and fibula fractures. In: Bucholz RW, Court-Brown CM, Heckman JD, Tornetta P III, eds. Rockwood and Green’s fractures in adults. 7th ed. Lippincott Williams & Wilkins; 2010:1867-1927.
- Hooper GJ, Keddell RG, Penny ID. Conservative management or closed nailing for tibial shaft fractures: a randomized prospective trial. J Bone Joint Surg Br. 1991;73(1):83-85. doi:10.1302/0301-620x.73b1.1991783
- Kapoor SK, Kataria H, Boruah T, Patra SR, Chaudhry A, Kapoor S. Expandable self-locking nail in the management of closed diaphyseal fractures of femur and tibia. Indian J Orthop. 2009;43(3):264-270. doi:10.4103/0019-5413.53457
- Bekmezci T, Baca E, Kocabas R, Kaynak H, Tonbul M. Early results of treatment with expandable intramedullary nails in tibial shaft fractures. Acta Orthop Traumatol Turc. 2005;39(5):421-424.
- Court-Brown CM, Christie J, McQueen MM. Closed intramedullary tibial nailing: its use in closed and type I open fractures. J Bone Joint Surg Br. 1990;72(4):605-611. doi:10.1302/0301-620x.72b4.2380211
- Anglen JO, Blue JM. A comparison of reamed and unreamed nailing of the tibia. J Trauma. 1995;39(2):351-355. doi:10.1097/00005373-199508000-00027
- Saruhan CS, Algün R, Barış B, Budak K. Unlocked use of interlocked intramedullary nails in tibial shaft fractures. Eklem Hastalik Cerrahisi. 2013;24(1):23-29. doi:10.5606/ehc.2013.06
- Siegel HJ, Sessions W, Casillas MA Jr. Stabilization of pathologic long bone fractures with the Fixion expandable nail. Orthopedics. 2008;31(2):143-148. doi:10.3928/01477447-20080201-31
- Lepore L, Lepore S, Maffulli N. Intramedullary nailing of the femur with an inflatable self-locking nail: comparison with locked nailing. J Orthop Sci. 2003;8(6):796-801. doi:10.1007/s00776-003-0709-8
- Lorich DG, Geller DS, Yacoubian SV, Leo AJ, Helfet DL. Intramedullary fixation of humeral shaft fractures using an inflatable nail. Orthopedics. 2003;26(10):1011-1014. doi:10.3928/0147-7447-20031001-10
- Ghafil D, Ackerman P, Baillon R, Verdonk R, Delince P. Expandable intramedullary nails for fixation of tibial shaft fractures. Acta Orthop Belg. 2012;78(6):779-785.
- Daglar B, Bayrakci K, Tasbas BA, Gürkan I, Agar M, Günel U. Short-term results of treatment of humeral and tibial fractures with new inflatable intramedullary nails. Acta Orthop Traumatol Turc. 2002;36(4):322-327.
- Smith WR, Zirar B, Agudelo JF, Morgan SJ, Steven NM, Lahti Z, et al. Expandable intramedullary nailing for tibial and femoral fractures: a preliminary analysis of perioperative complications. J Orthop Trauma. 2006;20(5):310-314. doi:10.1097/00005131-200605000-00002
- Fortis AP, Dimas A, Lamprakis AA. Expandable nailing system for tibial shaft fractures. Injury. 2008;39(8):940-945. doi:10.1016/j.injury.2008.01.022
- Serbest S, Tosun HB, Gökçe H. Results in the treatment of tibial diaphyseal fractures with expandable intramedullary nails. J Clin Anal Med. 2015;6(5):565-568.
Tables
Table 1. Patients’ demographic characteristics and clinical outcomes.
Figures
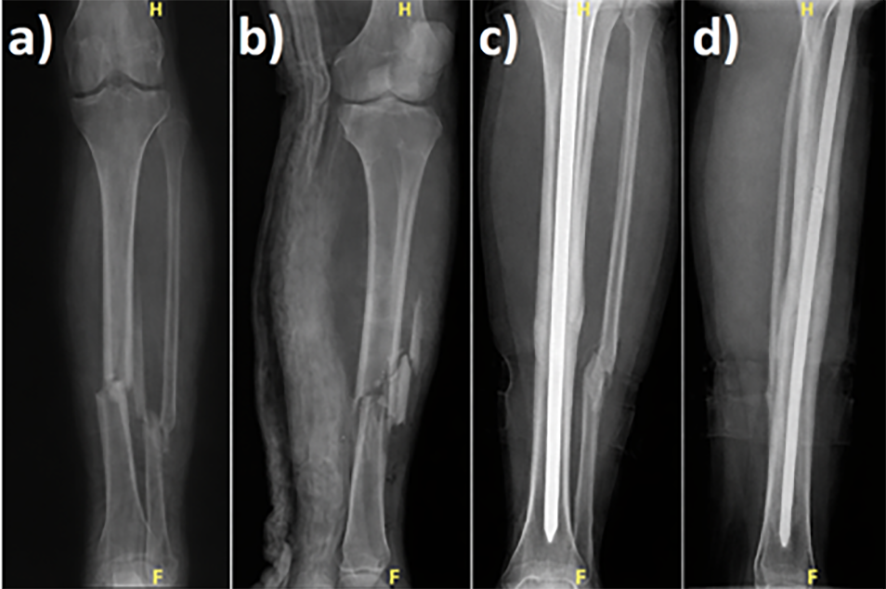
Figure 1. Patient with tibial AO type B3 fracture; (a, b) preoperative imaging, (c, d) after 1 year postoperatively.
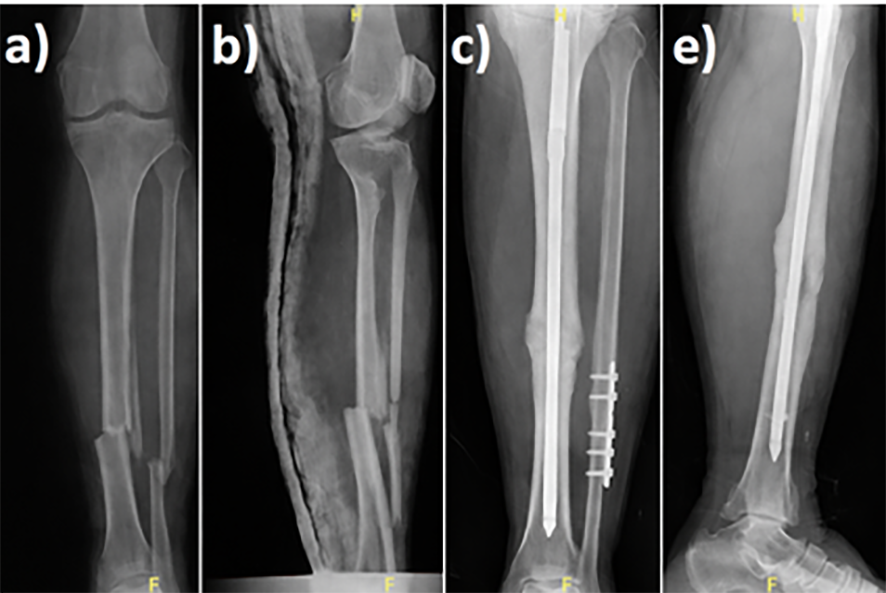
Figure 2. Patient with tibial AO type B2 fracture; (a, b) preoperative imaging, (c) postoperative view after 10 months with delayed union, (d, e) after performing autogenous bone grafting full union was achieved at the first year postoperatively.
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Kürşat Gençer, Fırat Ozan, Kaan Gürbüz, Erdal Uzun, Mustafa Özyalçın, Eyyüp Sabri Öncel, Fuat Duygulu. Result of the fixation of tibial shaft fractures by the inflatable intramedullary nail. Eu Clin Anal Med 2026;4(2):21-23. doi:10.4328/ECAM.79
- Received:
- 05.02.2016
- Accepted:
- 07.02.2016
- Published Online:
- 01.05.2016
- Printed:
- 01.05.2016