Abstract
Aim We aim to evaluate osteopathy in patients with thalassemia major (TM) by performing bone mineral densitometry (BMD) and biochemical indices and to emphasize preventive measures and the importance of early diagnosis of osteoporosis. Methods 37 TM patients (18 female, 19 male) were included in the study. The age, gender, biochemical parameters were recorded. BMD was determined using dual energy X-ray absorptiometry from lumbar vertebrae. Z scores were calculated automatically by the device. According to Z scores; <-1 was normal, -1-2 was osteopenia, >-2 was considered as osteoporosis. Results 9 patients’ Z scores (24.3%) were normal, 5 patients were osteopenic (13.5%), and 23 patients were osteoporotic (62.2%). In the osteoporotic group, parathyroid hormone (PTH) was low in 2 patients (5.4%) and vitamin D was deficient in 12 (32.4%) patients. Lumbar BMD was positively correlated with age (r=0.625, P=0.000), height (r = 0.759, P =0.000), weight (r=0.830, P=0.000), and BMI (r=0.730, P=0.000), and was negatively correlated with ALP (r=-0.422, P=0.010). In the osteopenic group, vitamin D was deficient in 2 patients (5.4%); all other biochemical parameters were within normal limits. Lumbar BMD was positively correlated with age (r=0.625, P=0.000), height (r=0.759, P=0.000), weight (r=0.830, P=0.000), and body mass index (BMI) (r=0.730, P= 0.000), and was negatively correlated with alkaline phosphatase (ALP) (r= -0.422, P= 0.010). Conclusion Despite regular transfusions, osteopathy may occur at high rates in patients with thalassemia.Keywords
Introduction
Beta thalassemias are a group of autosomal inherited disorders characterized by globin chain mutations in the hemoglobin tetramer and are due to defective hemoglobin synthesis; severe anemia, bone marrow expansion, skeletal deformity, and increased gastrointestinal iron absorption can be seen. Thalassemia major (TM) is the severe form of the disease and clinical symptoms appear between 6 months and 2 years. In this form, the patient requires regular blood transfusion and iron-chelating therapy throughout life, beginning in early childhood.1-2-3Recently, therapeutic approaches have increased the life expectancy and quality in thalassemia patients. However, osteoporosis has become the most important cause of morbidity of the disease and of skeletal findings that can lead to pathological fractures. The etiopathogenesis of TM-induced osteoporosis is known to be multifactorial. Genetic and acquired factors both play roles in the demineralization of bone in thalassemia. Bone marrow expansion secondary to ineffective erythropiesis with cortical thinning, hypogonadotropic hypogonadism, hypothyroidism, hypoparathyroidism, diabetes mellitus, direct toxic effects of iron overload on osteoblast numbers and activity, deleterious effects of desferrioxamine on the bone metabolism, the negative impact of chelation therapy on fibroblast proliferation and collagen synthesis, calcium and zinc deficiencies, low vitamin D levels due to aberrant vitamin D–parathyroid hormone axis, and reduced physical activity are responsible acquired factors.4-5-6-7-8-9 Osteoporosis is more common in women than in the general population, but men are more
commonly and more severely affected by thalassemia. It is presumed that this is due to lower compliance of male adolescents to desferrioxamine therapy.1 The most reliable and most commonly used method for measuring BMD is Dual Energy X-ray Absorptiometry (DEXA) which assesses bone mass at the lumbar spine and proximal femur.8 True bone density is volumetric BMD which can only be assessed by quantitative computed tomography, but this technique involves high radiation exposure.10 In this study TM patients followed regularly in our hospital were evaluated. Bone mineral density (BMD) and the parameters that may affect BMD and their relationshipto each other were assessed. Early diagnosis and preventive measures were implemented in cases where osteoporosis might develop.
Materials and Methods
The study included a total of 37 patients in the 5-33 year range followed in internal medicine and pediatrics clinics, whose diagnoses were confirmed with (hemoglobin) Hb electrophoresis and who were in need of transfusion at least once a month. Ethics committee approval was granted by our hospital. Signed consents were obtained from all patients and/or parents participating in the study. Patients not receiving regular treatment or who use osteoporosis preventive medicine (calcium and vitamin D) or therapeutic (bisphosphonates, etc.) agents, and those having chelation therapy, a history of a drug use that can affect bone metabolism, and those with any type of skeletal dysplasia were excluded.Age, sex, and drugs chelator agents were noted. Height and weight were measured. Body mass index (BMI) was calculated. Before the transfusion, Hb, ferritin, fasting blood glucose (FBG), alanine aminotransferase (ALT), aspartate aminotransferase (AST), Ca, phosphorus (P), alkaline phosphatase (ALP), thyroid stimulating hormone (TSH), free thyroxine (FT4), and intact parathyroid hormone (iPTH) and vitamin D levels were measured. Bone mineral densities of the patients included in the study were evaluated by a radiologist by the DEXA method. Bone mineral density of the lumbar spine (L1-L4) was measured in g/cm2. Z scores were calculated automatically by the device. Z score <-1 was normal, -1-2 was osteopenia and > -2 was considered as osteoporosis.The statistical analyses were carried out by Statistical Package for the Social Sciences (SPSS). Variables were expressed as mean±SD. Comparisons of variables were performed using unpaired Student t test. Bivariate associations of the variables were assessed using Pearson’s correlation coefficients and p value <0.05 was considered statistically significant.Results
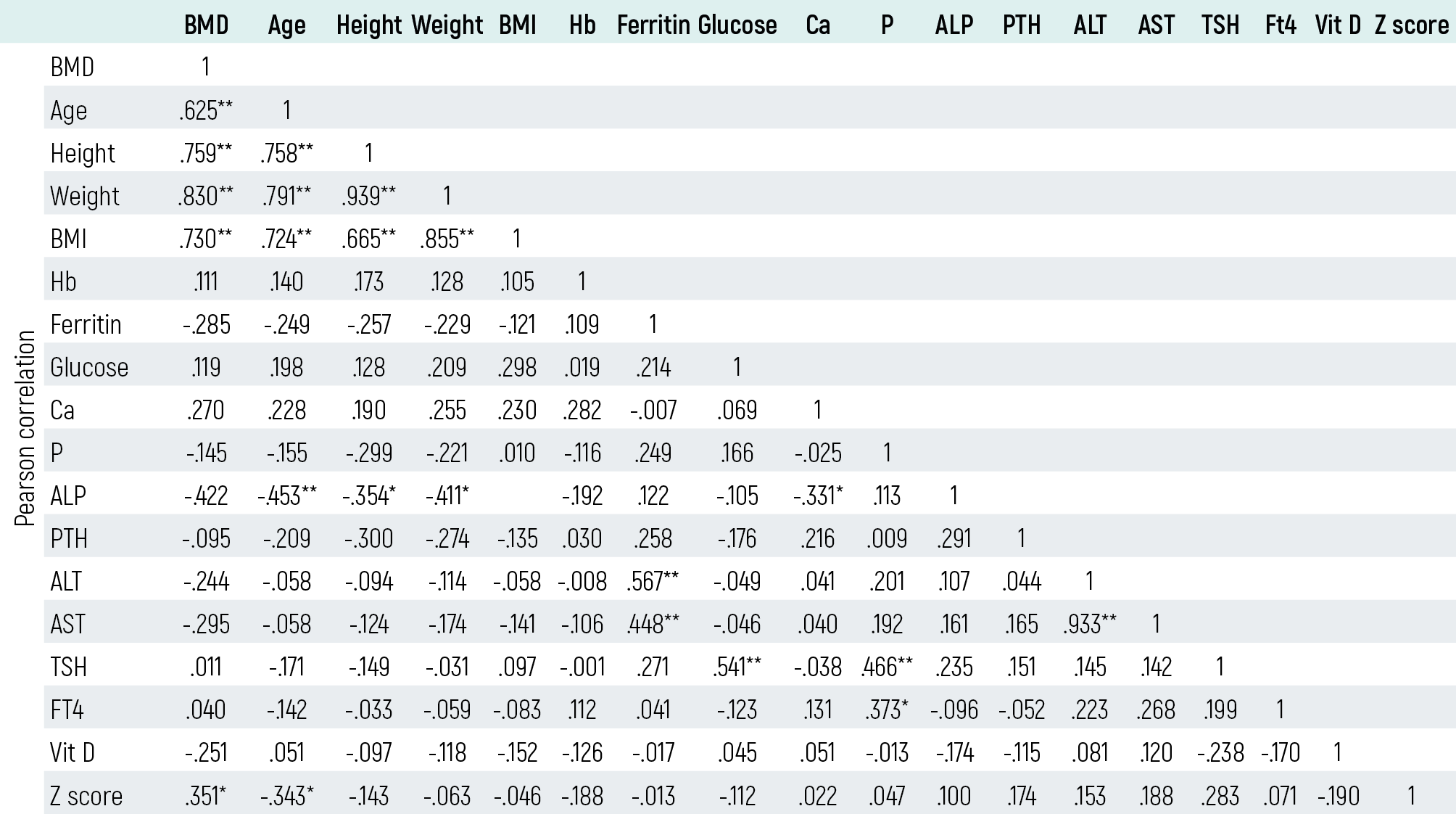
The total of 37 TM patients included 18 females and 19 males. The average age was 15.48±6.96 (5-33) years, height 145±19.91 cm, and weight 43.62±17.17 kg. Mean BMI was 19.67±3.26 kg/m2. Patients were grouped according to the lumbar region Z score; >-1 as normal, -1 -2 osteopenic, and <-2 as osteoporotic. Accordingly,lumbar region Z scores were: normal - 9 patients (5 females and 4 males) (24.3%), osteopenic – 5 patients (2 female, 3 male) (13.5%), and osteoporotic - 23 patients (11 females and 12 males) (62.2%). The average data of all three groups are summarized in Table 1. In the osteoporotic group, the following parameters were higher than normal: ALP in 6 patients (16.2%), AST in 5 patients (13.5%), ALT in 8 patients (21.6%), TSH in 2 patients (5.4%), fT4 in 6 patients (16.2%), and fasting blood glucose in 4 patients (10.8%); ferritin was high in all. Ca and P were normal in all. PTH was low in 2 patients (5.4%), vitamin D was severely deficient in 3 (<10 ng/mL) (8.1%) and deficient in 9 (<20 ng/mL) (24.3%).In the osteopenic group, FBG, Ca, P, PTH, ALT, AST, TSH, and FT4 levels were all within normal limits. One patient had high ALP value (2.7%). Vitamin D was severely deficient in 1 patient (11 ng/mL) (2.7%) and deficient in 1 (18 ng/mL) (2.7%). Lumbar BMD in the osteopenic group was positively correlated with age (r= 0.951, P= 0.013), weight (r = 0.916, P= 0.029), and BMI (r = 0.932, P= 0.021) and was negatively correlated with serum ferritin levels (r= -0906, P= 0.034).Of those patients with Z scores within normal levels, 2 had severely low vitamin D levels (5.4%) and 2 patients had low levels (5.4%). Ca, P, ALT, AST, TSH, PTH, and ALP values were within normal limits and fT4 was high in 2 patients (5.4%).In TM patients, Lumbar BMD was positively correlated with age (r = 0.625, P= 0.000), height (r= 0.759, P= 0.000), weight (r= 0.830, P= 0.000), and BMI (r= 0.730, P= 0.000) and negatively correlated with ALP (r = -0.422, P= 0.010) [Table 2].
Discussion
Osteoporosis is the most common disorder of the skeletal system and represents an important cause of morbidity in adult patients.2,10-11-12 It is characterized by reduced bone mass, disruption of bone architecture, and increased risk of bone fragility and fractures.4,11,13 Bone loss is a common feature even in well-treated thalassemia patients and despite adequate transfusion and iron chelation. In well-treated TM patients, the frequency of osteoporosis is approximately 40-50% and osteopenia, 45%.3,9,12 In a study of Chinese TM children, BMD deficit was detected in 62% at the spine and in 35% at the hip.8 Peak bone mass is also adversely affected; as a result, low bone mass can be seen in patients with TM, even those younger than age 12.1 To avoid possible complications (bone fractures and deterioration in the quality of life of these patients), bone densitometry screening should be done; it is important to start early, appropriate treatment. Late diagnosis and delayed treatment of osteoporosis in thalassemia patients can cause pain, fractures, and spinal deformities. This morbidity is multifactorial. Early screening, prevention, and treatment are so important. Therefore, annual BMD is advisable.9 Genetic and many acquired factors have been implicated in the patho genesis of osteoporosis in patients with thalassemia. Collagen type LA1 (COLIA1) polymorphism in the Sp1 gene is associated with severe osteoporosis. Also, vitamin D receptor (VDR) BsmI and Fokl polymorphism have been shown to be effective in bone mineralization and low bone density.9 Acquired factors that cause osteoporosis in thalassemia include: cortical and trabecular thinning of the bones as a result of bone marrow expansion because of increased ineffective erythropoiesis, calcium and phosphorus metabolism disorders, low PTH levels, low 1,25- (OH) 2 vitamin D3 level, hypogonadotropic hypogonadism, GH / IGF-1 deficiency, delayed puberty, hypothyroidism, diabetes mellitus, increased osteoclast function and decreased osteoblast function, developing iron overload secondary to blood transfusion, the toxic effects of desferrioxamine chelation therapy, male gender, and sedentary lifestyle..9-10,14-15 Of the 37 thalassemic patients enrolled in the study, 5 (13.5%) were osteopenic and 23 (62.1%) had osteoporosis. A total of 28 patients (75.6%) were osteopathic. Consistent with the literature, men were more likely (M/F=17/11) to be osteopathic. In studies of thalassemic male patients it is suggested that the presence of COLLIER II genes carried on the Sp1 polymorphism causes severe osteoporosis.16 However, in the literature there are studies demonstrating that gender does not affect the development of osteopathy.1,17 In the study of Kyriakou et al. of 76 thalassemia patients, vertebral osteoporosis was present in 89.5% and femoral neck osteoporosis was present in 84.2%. The incidence was higher in men than women.18 Çizmeci et al. reported osteopathy as present in 66%.17 In TM patients, due to the pathogenesis and secondary to treatment modalities, osteoporosis incidence increases with age. A negative correlation between age and the BMD Z scores.19 and increased incidence of osteoporosis with age has been reported in different studies.20-21 In our study there was also negative correlation between age and BMD Z scores (r= -0.343, P= 0.38).Body weight is one of the important determinants of bone mass. Putting strain on the mechanical skeleton leads to an increase in bone density. A positive correlation between BMI and BMD has been reported in the literature.20,22 In the current study there was a significant positive correlation between lumbar BMD and BMI (r= 0.730, P= 0.000). Our results are consistent with the literature. All our pre-transfusion Hb values were lower, as expected. There was no significant correlation between lumbar BMD and Hb values. The reason for this may be that our patients receive regular treatment and adequate transfusion. Similar to our results, there are studies available that report no relationship between BMD and meanpre-transfusion Hb levels.19,23 Excess iron accumulation in the bones can cause disruption of the number and activation of osteoid and bone mineralizations that can lead to osteoporosis. In our study, serum ferritin levels were high in all cases and we could not show such a relationship between ferritin and BMD in TM patients.In TM patients, progressive iron overload in the body as well as in the liver causes tissue damage and deterioration of the functions correlated with age.24 Impairment of hepatic vitamin D metabolism contributes to osteoporosis. Although definitive diagnosis of liver tissue damage requires biopsy, elevated liver enzymes may also provide guidance for suspected tissue damage.20,24 In one study, liver enzymes were found significantly higher than in the control group and negative correlation was reported between AST and femoral BMD.20 In our study, AST was high in 5 patients (13.5%) in the osteoporosis group and ALT was high in 8 patients (21.6%). There was no correlation between BMD, ALT, and AST in TM patients.Endocrine disorders in patients with thalassemia, impaired vitamin D metabolism due to liver damage, degradation of Ca and P absorption from the intestine connected to iron chelation drugs.20,25 are factors that cause imbalances in the Ca-P-ALP metabolism, which may result in a decreased BMD.20 In our study, ALP levels were high in 4 patients in the osteoporotic group and in 1 patient in the osteopenic group. Z scores were normal with values of ALP, Ca and P levels normal in all patients. In the literature, there are different results of serum Ca, P and ALP levels in patients with TM. Again, similar to our results, there are studies reporting that patients’ serum Ca levels are normal.26-27 But some other studies report that hypocalcemia can be seen in TM patients.6,19 There are studies showing that serum P levels are normal as we found in our study.26-27 but some studies indicate that serum P levels are hig.h28-29 Mahachoklertwatt et al. reported that serum ALP levels of child-adolescent patients with thalassemia were normal.6 and Pirinççioğlu et al. reported unusually low ALP levels.20 In our study group, high ALP values were found in 6 patients in the osteoporotic group and in 1 patient in the osteopenic group. In correlation analysis here was no relationship between BMD and Ca, P levels but a negative correlation between ALP levels and BMD was found. Çizmeci et al. could not find correlation between BMD and Ca, P, ALP levels.17 In the study of Bakan et al., Ca and ALP values were normal in all patients and P levels were high in 38%; they could not find a correlation between these values and BMD.30 ALP value increases in bone turnover and has been reported to be regarded as a marker of bone formation.31 Endocrine complications including thyroid gland and the hypothalamus-pituitary-thyroid axis disorders may arise during clinical follow-up of thalassemia major patients. Hypothyroidism was found in 2 patients in the osteoporotic group in this study. Hypothyroidism in patients with thalassemia is seen in 6-31% of patients. Iron accumulation in the thyroid gland causes thyroid dysfunction and this is one of the main causes of hypothyroidism in these patients.32 In the osteoporotic group, 2 (5.4%) had low iPTH values. There was no significant relationship between iPTH value and lumbar BMD (P= 0.173). In some studies PTH levels were found to be high and were negatively correlated with BMD.20,30 Mahachoklertwattana et al.6 found iPTH levels were higher than in healthy controls. Aslan et al. found high serum PTH levels in TM patients but reported no relationship between PTH and BMD.33 Diabetes is the most common endocrine complication in thalassemia. The frequency of diabetes is reported to be between 2.3% and 24%.34 Iron deposits in the pancreatic interstitial cells lead to storing more collagen and to microcirculation disorders. Impaired tissue oxygenation causes insulin deficiency over time.35 The onset of impaired glucose tolerance begins to appear in the twenties.36 4 of the osteoporotic patients had slightly high FBG levels, but none of these had diabetic symptoms. We found no association between FBG levels and lumbar BMD.25-OH vitamin D levels indicate the level of storage reserves in the liver and reflect the level of vitamin Din the body. In the study of Samsihraz et al., low vitamin D levels were not associated with low BMD. In our study, 3 of the osteoporotic patients were seriously insufficient, while 9 patients had insufficient vitamin D levels. In the osteopenic group 1 patient was seriously insufficient and again 1 patient had insufficient vitamin D levels. No correlation was found between BMD and vitamin D levels.In conclusion, osteopathy in patients with thalassemia occurs at high rates. Close monitoring of bone mineral density and the metabolic profiles of patients during routine follow-up of TM patients and early treatment will reduce complications.
Declarations
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
None of the authors received any type of financial support that could be considered potential conflict of interest regarding the manuscript or its submission.
Funding
None.
References
- Jensen CE, Tuck SM, Agnew JE, Koneru S, Morris RW, Yardumian A, et al. High prevalence of low bone mass in thalassaemia major. Br J Haematol. 1998;103(4):911-915.
- Kidson-Gerber GL, Francis S, Lindeman R. Management and clinical outcomes of transfusion-dependent thalassaemia major in an Australian tertiary referral clinic. Med J Aust. 2008;188(2):72-75.
- Borgna-Pignatti C, Gamberini MR. Complications of thalassemia major and their treatment. Expert Rev Hematol. 2011;4(3):353-366.
- Chatterjee R, Bajoria R. Osteopenia-osteoporosis syndrome in patients with thalassemia: understanding of type of bone disease and response to treatment. Hemoglobin. 2009;33(Suppl 1):136-138.
- Scacchi M, Danesi L, Cattaneo A, Valassi E, Pecori Giraldi F, Argento C, et al. Bone demineralization in adult thalassaemic patients: contribution of GH and IGF-I at different skeletal sites. Clin Endocrinol (Oxf). 2008;69(2):202-207.
- Mahachoklertwattana P, Chuansumrit A, Sirisriro R, Choubtum L, Sriphrapradang A, Rajatanavin R. Bone mineral density, biochemical and hormonal profiles in suboptimally treated children and adolescents with beta-thalassaemia disease. Clin Endocrinol (Oxf). 2003;58(3):273-279.
- Pietrapertosa AC, Minenna G, Colella SM, Santeramo TM, Renni R, D’Amore M. Osteoprotegerin and RANKL in the pathogenesis of osteoporosis in patients with thalassaemia major. Panminerva Med. 2009;51(1):17-23.
- Leung TF, Chu Y, Lee V, Cheng FW, Leung WK, Shing MM, et al. Long-term effects of pamidronate in thalassemic patients with severe bone mineral density deficits. Hemoglobin. 2009;33(5):361-369.
- Haidar R, Musallam KM, Taher AT. Bone disease and skeletal complications in patients with β-thalassemia major. Bone. 2011;48(3):425-432.
- Gaudio A, Morabito N, Xourafa A, Macrì I, Meo A, Morgante S, et al. Bisphosphonates in the treatment of thalassemia-associated osteoporosis. J Endocrinol Invest. 2008;31(2):181-184.
- Perrotta S, Cappellini MD, Bertoldo F, Servedio V, Iolascon G, D’Agruma L, et al. Osteoporosis in beta-thalassaemia major patients: analysis of the genetic background. Br J Haematol. 2000;111(2):461-466.
- Mamtani M, Kulkarni H. Bone recovery after zoledronate therapy in thalassemia-induced osteoporosis: a meta-analysis and systematic review. Osteoporos Int. 2010;21(1):183-187.
- Hamed HM, Galal A, Ghamrawy ME, Abd El Azeem K, Hussein IR, Abd-Elgawad MF. An SP1-binding site polymorphism in the COLIA1 gene and osteoporosis in Egyptian patients with thalassemia major. Blood Coagul Fibrinolysis. 2011;22(2):81-85.
- Tyler PA, Madani G, Chaudhuri R, Wilson LF, Dick EA. The radiological appearances of thalassaemia. Clin Radiol. 2006;61(1):40-52.
- Terpos E, Voskaridou E. Treatment options for thalassemia patients with osteoporosis. Ann N Y Acad Sci. 2010;1202:237-243.
- Wonke B, Jensen C, Hanslip JJ, Prescott E, Lalloz M, Layton M, et al. Genetic and acquired predisposing factors and treatment of osteoporosis in thalassaemia major. J Pediatr Endocrinol Metab. 1998;11(Suppl 3):795-801.
- Çizmeci MN, Akçay A, Akçay T, Şalcıoğlu Z, Tuğcu D, Akıcı F, et al. Evaluation of bone mineral density in patients with beta thalassemia major. Yeni Tıp Derg. 2013;30(2):109-114.
- Kyriakou A, Savva SC, Savvides I, Pangalou E, Ioannou YS, Christou S, et al. Gender differences in the prevalence and severity of bone disease in thalassaemia. Pediatr Endocrinol Rev. 2008;6(Suppl 1):116-122.
- Bielinski BK, Darbyshire P, Mathers L, Boivin CM, Shaw NJ. Bone density in the Asian thalassaemic population: a cross-sectional review. Acta Paediatr. 2001;90(11):1262-1266.
- Pirinççioğlu AG, Akpolat V, Köksal O, Haspolat K, Söker M. Bone mineral density in children with beta-thalassemia major in Diyarbakir. Bone. 2011;49(4):819-823.
- Wonke B. Bone disease in β-thalassemia major. Br J Haematol. 1998;103(4):897-901.
- Mahachoklertwattana P, Pootrakul P, Chuansumrit A, Choubtum L, Sriphrapradang A, Sirisriro R, et al. Association between bone mineral density and erythropoiesis in Thai children and adolescents with thalassemia syndromes. J Bone Miner Metab. 2006;24(2):146-152.
- Jensen CE, Tuck SM, Agnew JE, Koneru S, Morris RW, Yardumian A, et al. High incidence of osteoporosis in thalassaemia major. J Pediatr Endocrinol Metab. 1998;11(Suppl 3):975-977.
- Pollak RD, Rachmilewita E, Blumenfeld A, Idelson M, Goldfarb AW. Bone mineral metabolism in adults with beta-thalassaemia major and intermedia. Br J Haematol. 2000;111(3):902-907.
- Baytan B, Sağlam H, Erdal Ş, Beyazıt AN, Özgür T, Güneş AM, et al. Evaluation of endocrine complications in patients with thalassemia major. Güncel Pediatri. 2008;6:58-65.
- Mahachoklertwattana P, Chuansumrit A, Choubtum L, Sriphrapradang A, Sirisriro R, Rajatanavin R. Bone mineral density in children and young adults with beta-thalassemia trait. J Pediatr Endocrinol Metab. 2002;15(9):1531-1535.
- Di Stefano M, Chiabotto P, Roggia C, Garofalo F, Lala R, Piga A, et al. Bone mass and metabolism in thalassemic children and adolescents treated with different iron-chelating drugs. J Bone Miner Metab. 2004;22(1):53-57.
- Salama OS, Al-Tonbary YA, Shahin RR, Eldeen OA. Unbalanced bone turnover in children with beta-thalassemia. Hematology. 2006;11(3):197-202.
- de Vernejoul MC, Girot R, Gueris J, Cancela L, Bang S, Bielakoff J, et al. Calcium phosphate metabolism and bone disease in patients with homozygous thalassemia. J Clin Endocrinol Metab. 1982;54(2):276-281.
- Bakan B, Eser ÖG, Özkan F, Berk A, Yılmaz MA, Garipardıç M, et al. Evaluation of bone mineral density in children with thalassemia major. Turk J Osteoporos. 2012;18:72-77.
- Benigno V, Bartelloni S, Baroncelli GI, Bertacca L, Di Peri S. Effects of thalassemia major on bone mineral density in late adolescence. J Pediatr Endocrinol Metab. 2003;16(Suppl 2):337-342.
- Gamberini MR, De Sanctis V, Gilli G. Hypogonadism, diabetes mellitus, hypothyroidism, hypoparathyroidism: incidence and prevalence related to iron overload and chelation therapy in patients with thalassaemia major followed from 1980 to 2007 in the Ferrara Centre. Pediatr Endocrinol Rev. 2008;6(Suppl 1):158-169.
- Aslan I, Canatan D, Balta N, Kacar G, Dorak C, Ozsancak A, et al. Bone mineral density in thalassemia major patients from Antalya, Turkey. Int J Endocrinol. 2012;2012:573298.
- Arrigo T, Crisafulli G, Meo A, Sturiale M, Lombardo F, Miceli M, et al. Glucose tolerance, insulin secretion and peripheral sensitivity in thalassaemia major. J Pediatr Endocrinol Metab. 1998;11(Suppl 3):863-866.
- Wonke B. Clinical management of β-thalassemia major. Semin Hematol. 2001;38(4):350-359.
- Gamberini MR, Fortini M, Gilli G, Testa MR, De Sanctis V. Epidemiology and chelation therapy effects on glucose homeostasis in thalassaemic patients. J Pediatr Endocrinol Metab. 1998;11(Suppl 3):867-869.
Tables
Table 1. Demographic features and laboratory findings of thalassemic patients

Table 2. Pearson’s correlations between bone mineral densitometry and other laboratory parameters in thalassemic children
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Esra Akyüz Özkan, Zeynep Tuba Özdemir, Ayşe Neslin Akkoca. The evaluation of bone mineral density in patients with thalassemia major. Eu Clin Anal Med 2016;4(2): 24-28. doi:10.4328/ECAM.82
- Received:
- 03.03.2016
- Accepted:
- 08.03.2016
- Published Online:
- 01.05.2016
- Printed:
- 01.05.2016