Abstract
Mucoceles of the paranasal sinus are benign expanding lesions that primarily occur between the fourth and seventh decades of life. Sinus mucoceles may develop due to the obstruction of the normal passageway by trauma, inflammation, mass lesions, idiopathic, or iatrogenic causes. The most common site for the evolution of a mucocele is within the frontal sinuses, followed in frequency by the ethmoidal, maxillary, and sphenoid sinuses. The symptoms depend on the location and size of the mucocele. The symptoms can be classified as nasal, ophthalmologic, intracranial, and cosmetic. A mucocele can become infected, forming a mucopyocele, with a risk of infectious complications including meningitis, orbital cellulitis, and osteomyelitis. Today, the first choice of treatment is marsupialization of the mucoceles using endoscopic sinus surgery. External approaches to frontal sinus are still used, in erosion of the anterior frontal sinus wall and far lateral located lesions.
Keywords
Declarations
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
None of the authors received any type of financial support that could be considered potential conflict of interest regarding the manuscript or its submission.
Funding
None.
References
- Oliverio PJ, Zinreich SJ. Radiology of the nasal cavity and paranasal sinuses. In: Cummings CW, Fredrickson JM, Harker LA, Krause CJ, Richardson MA, Schuller DE, eds. Otolaryngology: Head and Neck Surgery. 3rd ed. Missouri: Mosby; 1998:1065-1091.
- Iannetti G, Cascone P, Valentini V, et al. Paranasal sinus mucocele: diagnosis and treatment. J Craniofac Surg. 1997;8:391-398. doi:10.1097/00001665-199708050-00011
- Fu CH, Chang KP, Lee TJ. The difference in anatomical and invasive characteristics between primary and secondary paranasal sinus mucoceles. Otolaryngol Head Neck Surg. 2007;136(4):621-625.
- Lai PC, Liao SL, Jou JR, et al. Transcaruncular approach for the management of frontoethmoid mucoceles. Br J Ophthalmol. 2004;88(5):725.
- Chahed H, Romdhane N, Zainine R, et al. Pediatric mucoceles: clinical aspects and therapeutic approaches. Rev Stomatol Chir Maxillofac. 2012;113(6):437-441.
- Shah A, Meyer DR, Parnes S. Management of frontoethmoidal mucoceles with orbital extension: is primary orbital reconstruction necessary? Ophthalmic Plast Reconstr Surg. 2007;23(4):267-271. doi:10.1097/iop.0b013e318073d19a
- Weitzel EK, Hollier LH, Calzada G, Manolidis S. Single-stage management of complex fronto-orbital mucoceles. J Craniofac Surg. 2002;13:739-745. doi:10.1097/00001665-200211000-00004
- Hejazi N, Witzmann A, Hassler W. Ocular manifestations of sphenoid mucoceles: clinical features and neurosurgical management of three cases and review of the literature. Surg Neurol. 2001;56:338-343.
- Stankiewicz JA. Sphenoid sinus mucocele. Arch Otolaryngol Head Neck Surg. 1989;115:735-740.
- Steven CM, Jorge DL, Robert HM. Mucoceles of the maxillary sinus. Otolaryngol Head Neck Surg. 1997;117:18-21.
- Bockmühl U, Kratzsch B, Benda K, Draf W. Surgery for paranasal sinus mucocoeles: efficacy of endonasal micro-endoscopic management and long-term results of 185 patients. Rhinology. 2006;44(1):62-67.
- Bockmühl U, Kratzsch B, Benda K, Draf W. Paranasal sinus mucoceles: surgical management and long-term results. Laryngorhinootologie. 2005;84(12):892-898.
- Mineck CW, Chandra RK, Cohen N. Orbital mucopyocele after the use of alloplastic materials in the management of frontal sinus fractures. Otolaryngol Head Neck Surg. 2006;135(6):974-976. doi:10.1016/j.otohns.2005.09.011
- Capra GG, Carbone PN, Mullin DP. Paranasal sinus mucocele. Head Neck Pathol. 2012;6:369-372.
- Thompson LDR, Wenig BM. Mucocele of paranasal sinus. In: Diagnostic Pathology: Head and Neck. Salt Lake City, UT: Amirsys; 2011:45.
- Obeso S, Llorente JL, Rodrigo JP, Sanchez R, Mancebo G, Suarez C. Paranasal sinuses mucoceles: our experience in 72 patients. Acta Otorrinolaringol Esp. 2009;60(5):332-339.
- Lund VJ. Fronto-ethmoidal mucoceles: a histopathological analysis. J Laryngol Otol. 1991;105:921-923. doi:10.1017/s0022215100117827
- Pierse JE, Stern A. Benign cysts and tumors of the paranasal sinuses. Oral Maxillofac Surg Clin North Am. 2012;24:249-264. doi:10.1016/j.coms.2012.01.007
- Bell GW, Joshi BB, Macleod RI. Maxillary sinus disease: diagnosis and treatment. Br Dent J. 2011;210:113-118. doi:10.1038/sj.bdj.2011.47
- Ng YH, Sethi DS. Isolated sphenoid sinus disease: differential diagnosis and management. Curr Opin Otolaryngol Head Neck Surg. 2011;19:16-20. doi:10.1097/moo.0b013e32834251d6
- Tal H, Altini M, Lemmer J. Multiple mucous retention cysts of the oral mucosa. Oral Surg Oral Med Oral Pathol. 1984;58:692-695. doi:10.1016/0030-4220(84)90036-7
- Caylakli F, Yavuz H, Cagici AC, Ozluoglu LN. Endoscopic sinus surgery for maxillary sinus mucoceles. Head Face Med. 2006;2:29. doi:10.1186/1746-160x-2-29
- Herndon M, McMains KC, Kountakis SE. Presentation and management of extensive fronto-orbital-ethmoid mucoceles. Am J Otolaryngol. 2007;28:145-147. doi:10.1016/j.amjoto.2006.07.010
- Chao-Jung L, Chuan-Hsiang K, Bor-Hwang K, et al. Frontal sinus mucocele presenting as oculomotor nerve palsy. Otolaryngol Head Neck Surg. 2002;126(5):588-590.
- Malhotra R, Wormald PJ, Selva D. Bilateral dynamic proptosis due to frontoethmoidal sinus mucocele. Ophthalmic Plast Reconstr Surg. 2003;19(2):156-157. doi:10.1097/01.iop.0000055829.79494.37
- Lee TJ, Li SP, Fu CH, et al. Extensive paranasal sinus mucoceles: a 15-year review of 82 cases. Am J Otolaryngol. 2009;30:234-238. doi:10.1016/j.amjoto.2008.06.006
- Kim YS, Kim K, Lee JG, Yoon JH, Kim CH. Paranasal sinus mucoceles with ophthalmologic manifestations: a 17-year review of 96 cases. Am J Rhinol Allergy. 2011;25:272-275. doi:10.2500/ajra.2011.25.3624
- Har-El G. Endoscopic management of 108 sinus mucoceles. Laryngoscope. 2001;111:2131-2134.
- Soon SR, Lim CM, Singh H, Sethi DS. Sphenoid sinus mucocele: 10 cases and literature review. J Laryngol Otol. 2010;124:44-47. doi:10.1017/s0022215109991551
- Trimarchi M, Bertazzoni G, Bussi M. Endoscopic treatment of frontal sinus mucoceles with lateral extension. Indian J Otolaryngol Head Neck Surg. 2013;65(2):151-156. doi:10.1007/s12070-012-0611-9
- Bockmühl U. Osteoplastic frontal sinusotomy and reconstruction of frontal defects. In: Kountakis S, Senior B, Draf W, eds. The Frontal Sinus. Berlin: Springer; 2005:281-289. doi:10.1007/3-540-27607-6_31
- Weber R, Draf W, Keerl R, et al. Osteoplastic frontal sinus surgery with fat obliteration: technique and long-term results using magnetic resonance imaging in 82 operations. Laryngoscope. 2000;110:1037-1044.
- Kennedy DW, Josephson JS, Zinreich SJ, Mattox DE, Goldsmith MM. Endoscopic sinus surgery for mucoceles: a viable alternative. Laryngoscope. 1989;99:885-895. doi:10.1288/00005537-198909000-00002
- Chiu AG, Vaughan WC. Management of the lateral frontal sinus lesion and the supraorbital cell mucocele. Am J Rhinol. 2004;18:83-86. doi:10.1177/194589240401800203
- Yanagisawa E, Scher DA. Laterally positioned mucocele of the frontal sinus. Ear Nose Throat J. 2002;81:202-204. doi:10.1177/014556130208100404
- Molony NC, Ah-See K, Rachmanidou A, Draf W. A survey of contemporary management of frontal sinus disease in the United Kingdom. Eur Arch Otorhinolaryngol. 2000;257(5):247-250. doi:10.1007/s004050050232
- Correa AJ, Duncavage JA, Fortune DS, Reinisch L. Osteoplastic flap for obliteration of the frontal sinus: five years’ experience. Otolaryngol Head Neck Surg. 1999;121(6):731-735. doi:10.1053/hn.1999.v121.a98218
- Weber R, Draf W, Keerl R, Kahle G, Schinzel S, Thomann S, et al. Osteoplastic frontal sinus surgery with fat obliteration: technique and long-term results using magnetic resonance imaging in 82 operations. Laryngoscope. 2000;110(6):1037-1044.
- Draf W. Endonasal micro-endoscopic frontal sinus surgery: the Fulda concept. Oper Tech Otolaryngol Head Neck Surg. 1991;2:234-240. doi:10.1016/s1043-1810(10)80087-9
- Draf W. Endonasal frontal sinus drainage type I-III according to Draf. In: Kountakis S, Senior B, Draf W, eds. The frontal sinus. Berlin: Springer; 2005:219-232. doi:10.1007/3-540-27607-6_24
- Busaba NY, Salman SD. Maxillary sinus mucoceles: clinical presentation and long-term results of endoscopic surgical treatment. Laryngoscope. 1999;109:1446-1449. doi:10.1097/00005537-199909000-00017
- Martin RJ, Jackman DS, Philbert RF, McCoy JM. Massive proptosis of the globe. J Oral Maxillofac Surg. 2000;58:794-799. doi:10.1053/joms.2000.7268
- Busaba NY, Siegel N, Salman SD. Bacteriology of nontraumatic maxillary sinus mucoceles versus chronic sinusitis. Laryngoscope. 2000;110:969-971. doi:10.1097/00005537-200006000-00016
- Khong JJ, Malhotra R, Selva D, Wormald PJ. Efficacy of endoscopic sinus surgery for paranasal sinus mucocele including modified endoscopic Lothrop procedure for frontal sinus mucocele. J Laryngol Otol. 2004;118:352-356. doi:10.1258/002221504323086534
- Busaba NY, Kieff D. Endoscopic sinus surgery for inflammatory maxillary sinus disease. Laryngoscope. 2002;112:1378-1383. doi:10.1097/00005537-200208000-00010
- Kosling S, Hintner M, Brandt S, Schulz T, Bloching M. Mucoceles of the sphenoid sinus. Eur J Radiol. 2004;51:1-5.
- Hadar T, Shvero J, Nageris BI, Yaniv E. Mucus retention cyst of the maxillary sinus: the endoscopic approach. Br J Oral Maxillofac Surg. 2000;38:227-229. doi:10.1054/bjom.1999.0160
- Rejab E, Said H, Saim L, Thim L. Sphenoid sinus mucocele: a possible late complication of radiotherapy to the head and neck. J Laryngol Otol. 1991;105:959-960. doi:10.1017/s002221510011792x
- Sethi DS. Isolated sphenoid lesions: diagnosis and management. Otolaryngol Head Neck Surg. 1999;120:730-736. doi:10.1053/hn.1999.v120.a89436
Figures
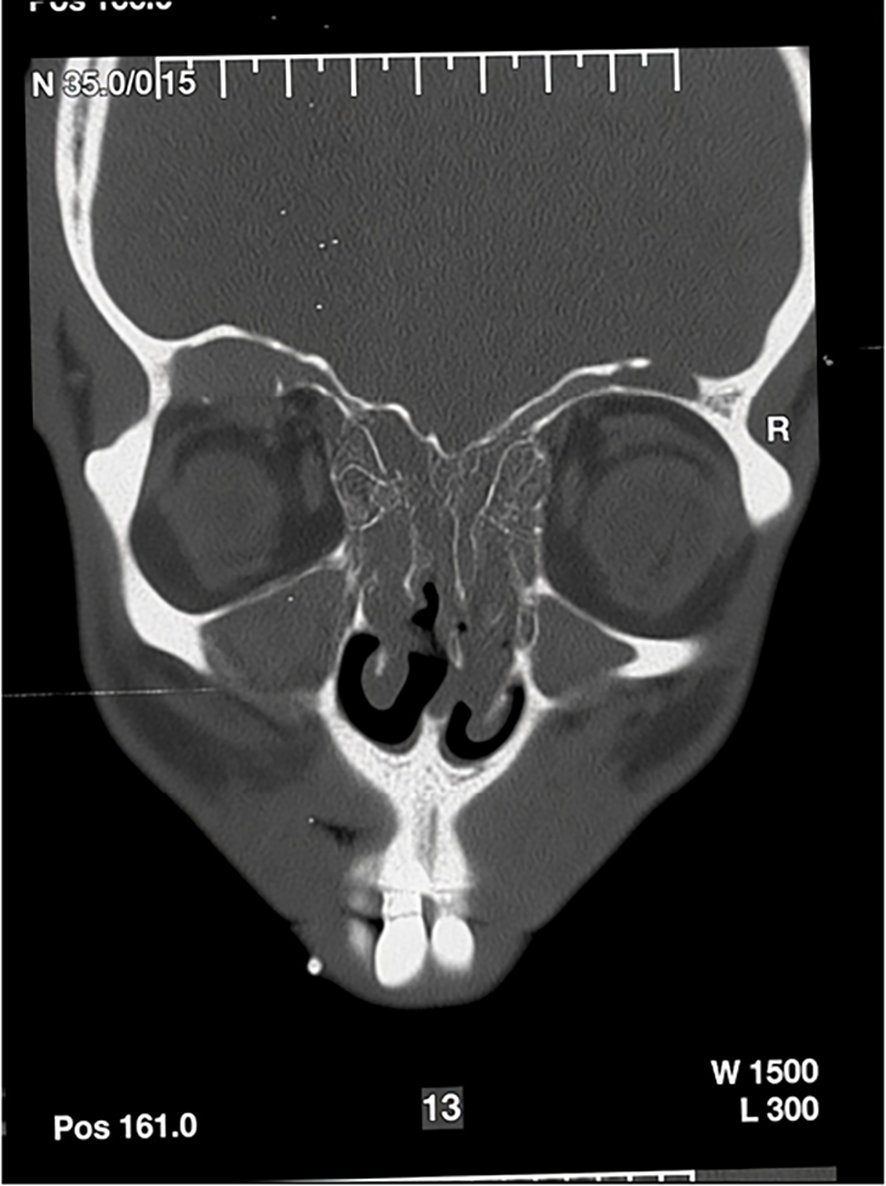
Figure 1. Frontal sinus mucocele due to nasal polyposis

Figure 2. The coronal plane CT image showing a mucocele (asteriks) in the right frontal sinus base that thinned the bone structure (A). In addition, thinning (arrows) and deformation can be observed in the right sinus roof (B) and anterior wall of the left frontal sinus (C).

Figure 3. Frontal sinus trephination in a patient that cannot be entubed due to giant hemangioma of the tongue
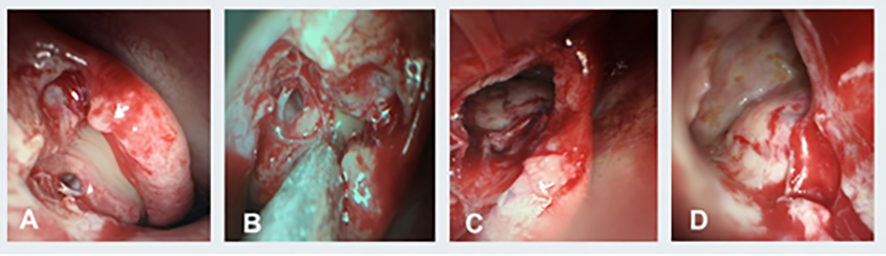
Figure 4. Endoscopic marsupialization of fronto-ethmoid mucocele
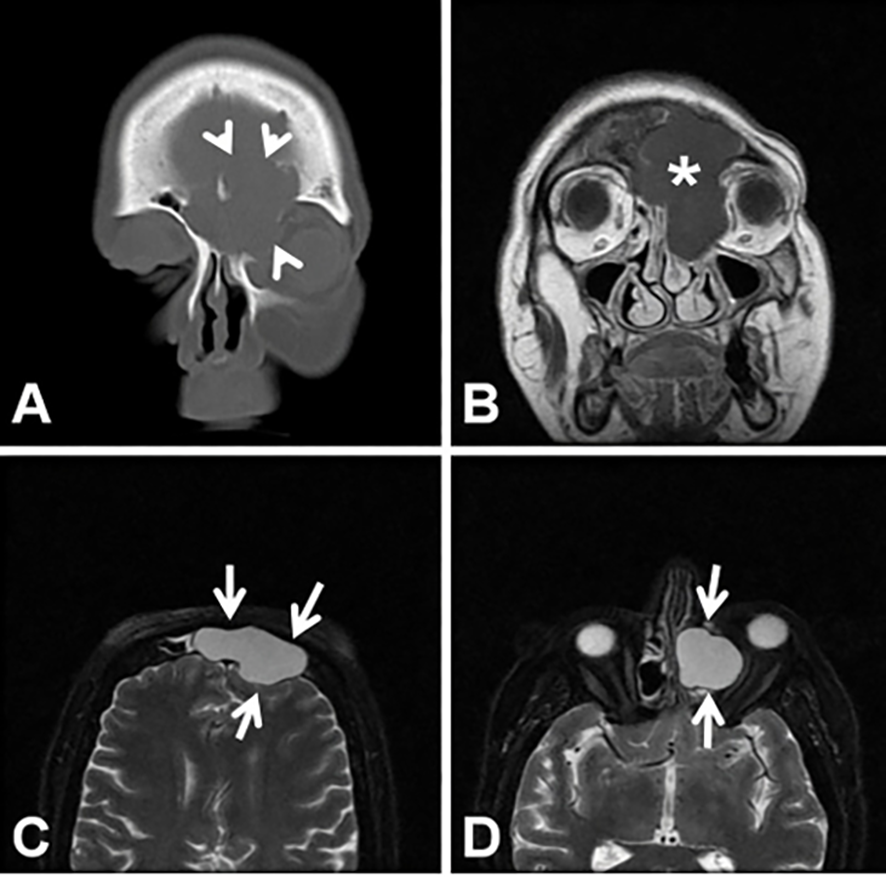
Figure 5. A huge fronto-ethmoidal located mucocele (asterisk) is shown. In the coronal CT (A) and T1 (B) and T2-weighted MR images (C, D) the expansile mucocele (arrows) causes thinning (arrowheads) of the frontal sinus walls.
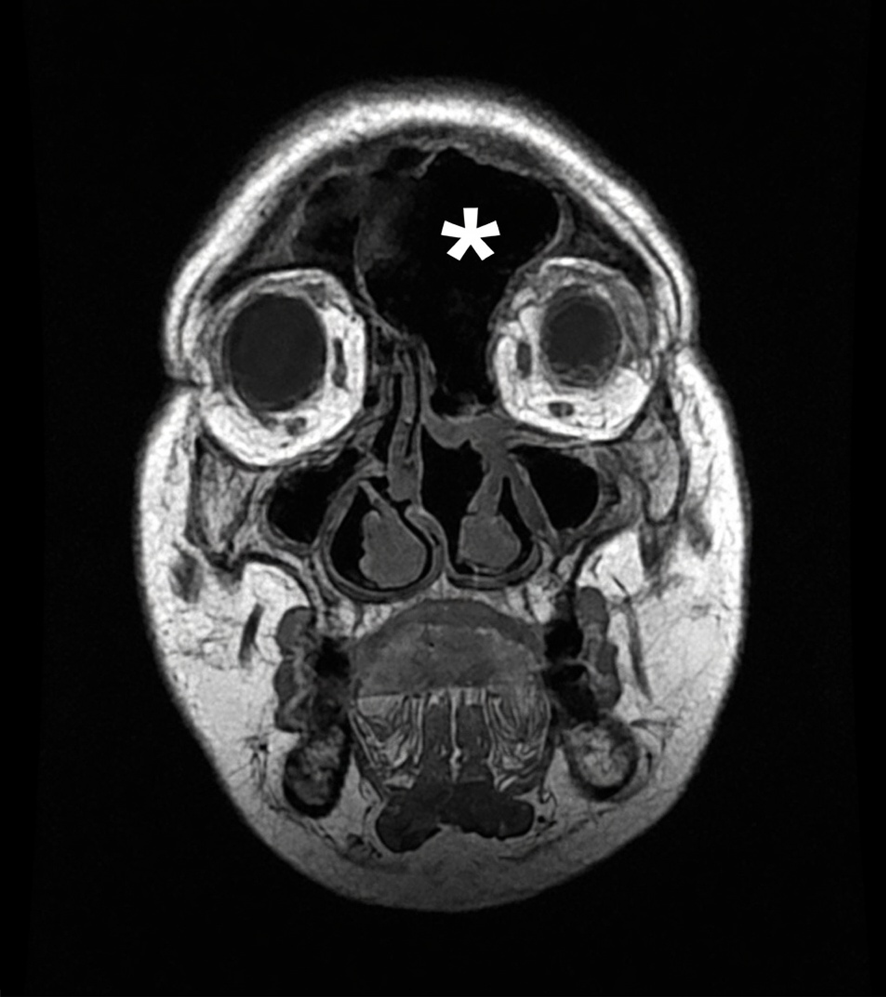
Figure 6. The coronal T1-weighted MR image after surgery (E). Air (asterisk) is observed in the left fronto-ethmoidal cavity
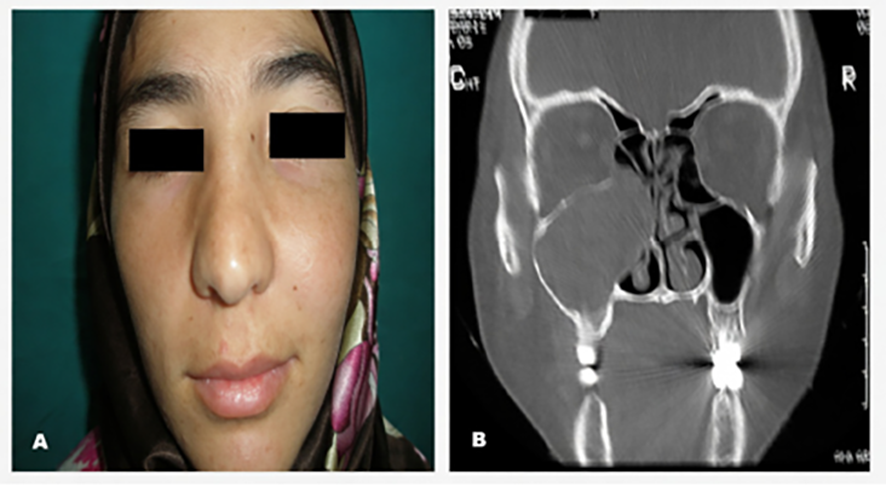
Figure 7. In the photograph, expansion of the maxillary bone and in CT scan; medial expansion of the wall of the maxillary sinus is seen.
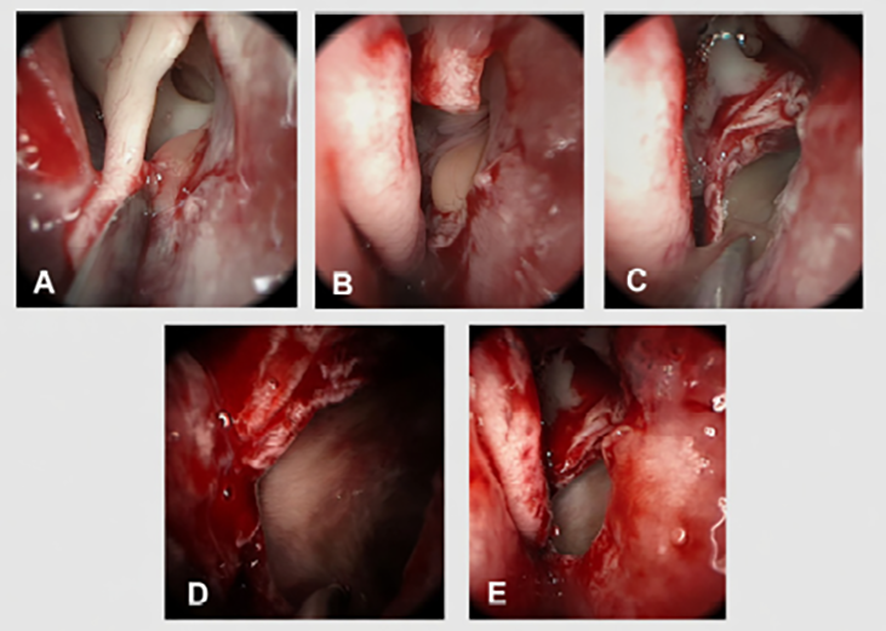
Figure 8. Endoscopic marsupialization of the maxillary sinus mucocele.
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Özer Erdem Gür, Mustafa Kaymakcı, Nevreste Didem Sonbay Yılmaz. Paranasal sinus mucoceles. Eu Clin Anal Med 2026;4(3):90. doi:10.4328/ECAM.97
- Received:
- 06.06.2016
- Accepted:
- 11.06.2016
- Published Online:
- 01.09.2016
- Printed:
- 01.09.2016