Abstract
Multiligament injury of knee is usually the result of sports injury and trauma. Multiligament injury that caused by high-energy trauma often shows the coexistence with fracture and fracture-dislocation. It is vital to perform the surgical procedure in the correct order. Disruption of at least 2 of the 4 primary knee ligaments is called multiligament injury of knee. In most cases that also accompanied by knee dislocation, may seem reduced radiologically, but it is important to keep an eye open for the risk of vascular and nerve pathologies. Decision making in the multiligament injury of knee has some controversies, especially surgical versus conservative treatment, repair versus reconstruction of injured ligamentous structures, acute versus late surgery, and single versus two-staged surgery of injured ligaments. This review investigates the diagnosis and treatment of the multiligament injuries of knee. Possible complications, surgical tip and tricks were also shared with our clinical experiences.
Keywords
Introduction
Knee ligaments plays a critical role in providing of static knee stability, the protection of kinematics, preventing abnormal rotation and dislocation. Injury of these structures is also cause damage in meniscal structure, chondral surface and knee dislocation.1 Traumas that containing two or more knee ligament injuries is called ‘’multiple ligament injuries’’. Multiligament injury of knee (MLIK) and knee dislocation (KD) can be classified in several different ways according to number of injured ligaments, direction of displacement (Kennedy.2 classification) and velocity of energy. MLIs are often seen together with knee dislocation however do not present as an obvious knee dislocation (KD) and most spontaneously reduce prior to evaluation.3 The most commonly preferred classification was described by Schenck which based on the pattern of multiligamentous injury of KD in practice (Table 1).6 The incidence of vascular injury in knee dislocations with multi ligament injuries has been estimated as 18% and the frequency of nerve injuries was 25%.4,5 The MLIK, although rare, is a life treating injury with the potential for loss of limb due to susceptibility of an associated vascular and neural injury.5,6 The structures that stabilizing the knee are divided into primary and secondary (Table 2). Primary structures are ACL, PCL, MCL and LCL. These four primary ligaments basis for the classification of multiligament injured-knee. Recent studies shows that the popliteal artery injury is 20-40%, neurological damage due to direction of dislocation was found 16-40% of all multiple ligament injuries.8,9 According to the anatomic classification of Schenck, vascular injury rate was highest in patients with Type IV. However, the management of multiple ligament injury is difficult and brings many complications. 80% of patients diagnosed with vascular injury are underwent surgical repair. 12% of patients who have vascular injury are amputated during this process.4 Neurovascular injuries and complications associated with knee dislocation must be demonstrated and emergency interventions should be implemented at the acute stage. Single or two-stage surgical procedures, open or closed surgical strategies is adopted in chronic process. Isolated Posterolateral corner (PLC) or Posteromedial corner (PMC) injuries considered as multiple ligament injuries; such as combination of Anterior Cruciate ligament (ACL), Posterior Cruciate ligament (PCL), Lateral Collateral (LCL) and Medial Collateral ligament (MCL) also described as multiple ligament injury.5,11 Physical Examination (PE) After limb-threatening pathologies are excluded, the surgeon must focus on the examination of ligaments. Lachman test, anterior drawer and pivot shift test for ACL, a posterior drawer for PCL, medial and lateral stress tests at 20-30° flexion for MCL/LCL and PLC/PMC is performed while examination. If the bucket-handle tear or another locked knee pathology has occurred, the physical examination may fail. Knee effusion, distal pulses and neurologic conditions must be checked starting from the emergency conditions to 48 hours after trauma. Knee must be reduced before vascular examination. Accuracy of PE of dislocated knee for injury of the popliteal artery can be safe and reliable method with a 94.3% positive predictive value.12 Coronal and sagittal plane or multidirectional instability can be found and knee could easily dislocate multidirectional in the examination (Figure 1). Knee extensor mechanism in favor of probable pathological as patellar tendon rupture. An initial examination is very important in order not to overlook the patellar tendon ruptures. Imagination After a detailed PE, anteroposterior and lateral x-ray images are taken (Figure 2). Immediate anterior-posterior knee radiographs may be helpful before manipulation for dislocation. Possible avulsion fractures and a second type fracture detected by plain radiographs may give an idea about injured ligaments. After a reduction maneuver, plain radiographs must be repeated. For further evaluation of detected intra-articular fracture, CT is needed. The patient with knee dislocation is under high risk of neurovascular injury (Figure 3). Although the ankle brachial index (ABI) is not a gold standard for every patient, it can be useful in emergency conditions. The associations of low (< 0.90) and high (> 1.40) ABI may predict the potential vascular damage. However, contrast-enhanced computed tomography (angiography) is the most useful imaging method for detecting vascular pathology. Hematoma draining can apply under sterile conditions for limiting acute hemorrhagic process, then can hospitalize with splint immobilization. A conventional MRI is necessary to evaluate ligamentous structure and for surgical planning (Figure 4). The necessity of Doppler ultrasonography is not clear, but it is useful for vascular integrity before CT angiography. Surgical strategy and algorithm Antibiotic prophylaxis is performed 30 minutes before surgery with 1 g of cefazolin iv. for closed wound injury. The surgical approach depends on the number of injured ligaments. Isolated ACL and PCL can be reconstructed via arthroscopic. However, MCL, LCL, PLC injuries needs open approach or combination of mini-open and arthroscopy. Before the surgical process, examination must be repeated under anaesthetic conditions. Routine arthroscopy is performed through standard anterolateral and anteromedial portals. If open approach is going to prefer, medial parapatellar or sub-vastus arthrotomy is useful for multiligament management. After the arthrotomy is made and appropriate releases performed, intra articular pathologies should be check for the overlooked injuries such as patellar tendon/Quadriceps rupture and osteochondral fractures. A complete debridement is performed for intra-articular ligament remnants via arthroscopic. After the detecting of existing pathologies, the procedure is applied as follows: Reduce the meniscal torn/bucket-handle and repair with sutures*. Prepare the tibial and femoral tunnels for posterior cruciate ligament**. If the double bundle ACL reconstruction is preferred 2 tunnels must be divergent with a 1- to 2-mm bone bridge at the aperture. Prepare the femoral and tibial tunnels for anterior cruciate ligament. Check the pin replacements by C-arm fluoroscopy. Firstly, PCL tendon graft is inserted to the PCL femoral and tibial tunnels with suture guides. PCL tendon graft is fixed on the femoral side. ACL tendon graft is inserted to the ACL femoral and tibial tunnels with suture guides. ACL tendon graft is fixed at the femoral side. Satisfy the leg alignment and palpate the tibiofemoral step-off while knee fixed 90° of flexion (The surgeon must ensure that the anatomic anterior step-off of the tibia has been re-established.) A single bundle PCL tendon graft is fixed on the tibial side by an interference screw while graft tensioned and posterior drawer test is applying. ACL tendon graft is fixed on the tibial tunnel with an interference screw while knee at near neutral extension and neutral position on sagittal plane. Both grafts is fixed by a tensile force of about 10 pounds. The knee is then cycled through repeated arcs of motion to ensure that the graft is well settled and tensioned. Once bi-cruciate ligament stability has been reestablished, collateral laxity can be re-evaluated. Medial collateral and lateral collateral ligaments is repaired/reconstructed after the fixation of ACL and PCL grafts. To avoid the increased risk of failure the MCL graft tibial insertion should be posteriorized to mimicking the anatomy.13 Menisco-capsular junction tears is repaired with primary sutures after achieving valgus-varus stability. Drainage set is applied in to the joint after repairing of capsule. A full extended, hinged knee brace is applied for immobilization. The patient who undergo primary repair and reconstruction of multi ligaments were allowed to bear weight on the surgical extremity with a hinged knee brace locked in extension. Use of brace is continued during 6 weeks after surgery. Active rehabilitation treatment and full weight bearing is started after 6 weeks of surgery. Second phase of rehabilitation contains gradually progress (10˚ per week, if it is possible) to full range of motion, quadriceps exercises, full weight bearing and normal gait pattern. It is easy to repair the meniscal tears before cruciate reconstruction. Make sure that the tibial tunnel entry points are not too close. The femoral footprint of the ACL is evaluated using the lateral intercondylar ridge as a reference and secure a 2-mm back wall. The tibial tunnel was prepared using a guide with an angle of 45 degrees, placed in the posterior region, at the midpoint of the lower part of the PCL facet. In the lateral fluoroscopic view, the guide pin must be 5.5 mm proximal to the champagne-glass drop-off on the posterior aspect of the tibia. With the knee flexed to 120, an eyelet guide pin is then placed in the femoral footprint, midway between the anteromedial and posterolateral bundles, through the accessory medial portal.Discussion
Knee dislocations are classified by two different ways. One of these classifications is defined according to the direction of the tibia is displaced. This results in 5 different categories: anterior, posterior, lateral, medial, or rotatory. The anterior-medial and lateral, posterior-lateral, and medial dislocations are classified as “rotatory” dislocation. This case is classified as posterior-lateral rotatory dislocation which occur less than 3% off all knee dislocations. Mechanism of knee injury determines the direction of the knee dislocation. A posterior-directed force applied to the proximal tibia when the knee is flexed to 90° is thought to produce a posterior dislocation, the so-called “dash-board” injury. Medial and lateral dislocations result from varus/valgus stresses applied to the knee. A combination of varus/valgus stress with hyperextension/blow to proximal tibia will likely produce one of the rotatory dislocations. The second classification is done according to the anatomical classification of multiple ligament injuries. Classification that is done according to the multiple ligament injuries, known as Schenck classification.14 Few recent studies in the literature have directly compared surgical treatment (repair) of multiligament knee injuries with nonoperative management.15,16 Bicruciate injured knee is a cause of instability in itself. From this perspective, surgical management is unavoidable for multiligament injury. While arthroscopic techniques have not yet been used, conservative treatments have been used in the past. Nowadays, it is technically impossible to compare surgical treatment with conservative treatment and surgical treatment of multiple ligament injury is no longer a matter of debate. Patients with both cruciate ligament reconstruction may lead to graft loss, if the posteromedial corner injury is neglected.17 Therefore, PMC repair has primary importance in multi-ligament injuries. Primary repair of PLC is known with high revision rates.18,19 Therefore, reconstruction of PLC should be preferred instead of repair in patients with PLC injuries. Meniscal tears and chondral damage is observed in most cases of knee dislocation with multiple ligament injuries. In our case, both side meniscal tears have been treated by primary sutures with early surgical procedures. Because of the late repair of meniscal tears, low IKDC scores and three compartmental chondral damage will be inevitable.20,21Surgical timingSurgical timing depends on the ligaments injured, the vascular compromise of the extremity, compartment syndrome, accompanied by open fracture, and irreducible dislocation. Reduction stability, and the overall health of the patient. The patients with knee dislocation must be examined for vascular compromise and nerve injury. After determining vascular injury, temporary external fixator must be applied urgently. There are conflicting results on timing of primary surgery in the literature. When the treatment of the patients with multiple ligament injuries is compared as surgical or conservative, and early or late surgical timing, excellent / good functional and clinical outcomes can be achieved.18,22 Jiang et al. reported a systematic review about the timing of surgical treatment of knee dislocations. They reported that was no difference in the surgical processes significantly between surgical timing groups such as acute, chronic, or staged.23 But we believe that the early diagnosis and treatment of multiple ligament injuries will improve the functional outcomes. If there are skin problems, vascular repair and additional injury (polytrauma, compartment syndrome, etc.) delayed
surgery (3w<) can be performed. Surgical algorithm of multi ligament injuries: The way to be followed in this stage will determine the success of the surgery. First step toward the multi ligament surgery is cruciate reconstruction. While setting the bi-cruciate reconstruction, PCL must be tensioned and fixed to the femoral and tibial tunnels before ACL graft replacement. PCL is cornerstone of multi ligament reconstruction. If the ACL graft attach to the tunnels before PCL reconstruction, tibial subluxation can provoke posteriorly.24 Second step is repairing of collateral ligaments that laxity is repeated under anesthesia to confirm the initial clinical impression and the findings suggested pre-operatively.25 Neglected injury of the PMC is one of the causes of ACL and PCL graft failures.7 Diagnosing and management of PMC injuries are critical for graft survey. Third step of MLKI surgery is includes the repair of concomitant injuries like medial patellofemoral ligament tear, quadriceps tendon and patellar tendon rupture. These structures can be left to the 2nd stage surgery. These structures may also lead to graft failures and results with poor clinical outcomes if neglected.17,25,26 Acute/immediate treatment of patients with knee dislocation that primary repair and reconstruction, requires a substantial experience and planning.RehabilitationCombination of primary repair and reconstruction of MLKI treatment by single stage open or closed surgical procedures can result with successful outcomes (Figure 5).24 Duration of prolonged immobilization has made it difficult to prevent arthrofibrosis in this case. Passive motion is necessary to prevent arthrofibrosis at the first 4 weeks after the reconstruction of multi-ligament injuries.16 Accompanying patellar tendon rupture or avulsion fractures adversely affect the rehabilitation process.
Conclusion
In this article, depending on the traumatic knee dislocation; the surgical management of MLIK is discussed. Vascular injury following a knee dislocation is a potentially devastating component that could result in loss of life or limb. Care must be taken because of the high incidence of vascular and nerve injuries after knee dislocation. MLIK should be treated in the acute setting whenever possible. The followed order of the multiligament reconstruction has a key role for the success of the surgery. Approximately, all of the multiligament injury can be treated in a single stage. A second stage procedure can be needed for the reconstruction of secondary stabilizers such as MPFL. Postoperative rehabilitation of multiligament injured knees necessitates close follow-ups and longer periods of supervision by an experienced physical therapist.
Declarations
Informed Consent
Not applicable.
Conflict of Interest
The authors declare no conflict of interest.
Funding
None.
References
- DeLee JC, Drez D, Miller MD, Abdollahi K, Adelson PD, Albright JP, et al. DeLee & Drez’s orthopaedic sports medicine: principles and practice. Vol 4. Saunders; 2014.
- Kennedy JC. Complete dislocation of the knee joint. J Bone Joint Surg Am. 1963;45:889-904. doi:10.2106/00004623-196345050-00001
- Cook S, Ridley TJ, McCarthy MA, Gao Y, Wolf BR, Amendola A, et al. Surgical treatment of multiligament knee injuries. Knee Surg Sports Traumatol Arthrosc. 2015;23(10):2983-2991. doi:10.1007/s00167-014-3451-1
- Medina O, Arom GA, Yeranosian MG, Petrigliano FA, McAllister DR. Vascular and nerve injury after knee dislocation: a systematic review. Clin Orthop Relat Res. 2014;472(9):2621-2629. doi:10.1007/s11999-014-3511-3
- Matthewson G, Kwapisz A, Sasyniuk TM, MacDonald PB. Vascular injury in the multiligament injured knee. Clin Sports Med. 2019;38(2):199-213. doi:10.1016/j.csm.2018.11.001
- Buyukdogan K, Laidlaw MS, Miller MD. Surgical management of the multiple-ligament knee injury. Arthrosc Tech. 2018;7(2):e147-e164. doi:10.1016/j.eats.2017.08.079
- Başal Ö. Biyomekanik ve biyomateryaller. In: Baki C, ed. Ortopedi ve spor yaralanmaları. Derman Medical Publishing; 2019:24-43.
- Brautigan B, Johnson DL. The epidemiology of knee dislocations. Clin Sports Med. 2000;19(3):387-397. doi:10.1016/s0278-5919(05)70213-1
- Wilson SM, Mehta N, Do HT, Ghomrawi HMK, Lyman S, Marx RG. Epidemiology of multiligament knee reconstruction. Clin Orthop Relat Res. 2014;472(9):2603-2608. doi:10.1007/s11999-014-3653-3
- Wascher DC. High-velocity knee dislocation with vascular injury: treatment principles. Clin Sports Med. 2000;19(3):457-477. doi:10.1016/s0278-5919(05)70218-0
- Başal Ö, Burç H. Orthopaedics and sport medicine for researchers. 1st ed. Derman Medical Publishing; 2015.
- Miranda FE, Dennis JW, Veldenz HC, Dovgan PS, Frykberg ER. Confirmation of the safety and accuracy of physical examination in the evaluation of knee dislocation for injury of the popliteal artery: a prospective study. J Trauma. 2002;52(2):247-251. doi:10.1097/00005373-200202000-00008
- Ferrari MB, Chahla J, Mitchell JJ, Moatshe G, Mikula JD, Marchetti DC, et al. Multiligament reconstruction of the knee in the setting of knee dislocation with a medial-sided injury. Arthrosc Tech. 2017;6(2):e341-e350. doi:10.1016/j.eats.2016.10.003
- Schenck RC Jr. Classification of knee dislocations. In: The multiple ligament injured knee. Springer; 2004:37-49. doi:10.1007/978-0-387-22522-7_3
- Taylor AR, Arden GP, Rainey HA. Traumatic dislocation of the knee: a report of forty-three cases with special reference to conservative treatment. J Bone Joint Surg Br. 1972;54(1):96-102. doi:10.1302/0301-620x.54b1.96
- Levy BA, Freychet B. Knee multiligament injury. Clin Sports Med. 2019;38(2):xv-xvi. doi:10.1016/j.csm.2019.01.001
- Lundquist RB, Matcuk GR Jr, Schein AJ, Skalski MR, White EA, Forrester DM, et al. Posteromedial corner of the knee: the neglected corner. Radiographics. 2015;35(4):1123-1137. doi:10.1148/rg.2015140166
- Levy BA, Dajani KA, Whelan DB, Stannard JP, Fanelli GC, Stuart MJ, et al. Decision making in the multiligament-injured knee: an evidence-based systematic review. Arthroscopy. 2009;25(4):430-438. doi:10.1016/j.arthro.2009.01.008
- Geeslin AG, Moulton SG, LaPrade RF. A systematic review of the outcomes of posterolateral corner knee injuries, part 1: surgical treatment of acute injuries. Am J Sports Med. 2015.
- King AH, Krych AJ, Prince MR, Sousa PL, Stuart MJ, Levy BA. Are meniscal tears and articular cartilage injury predictive of inferior patient outcome after surgical reconstruction for the dislocated knee? Knee Surg Sports Traumatol Arthrosc. 2015;23(10):3008-3011. doi:10.1007/s00167-015-3671-z
- Krych AJ, Sousa PL, King AH, Engasser WM, Stuart MJ, Levy BA. Meniscal tears and articular cartilage damage in the dislocated knee. Knee Surg Sports Traumatol Arthrosc. 2015;23(10):3019-3025. doi:10.1007/s00167-015-3540-9
- Gella S, Whelan DB, Stannard JP, MacDonald PB. Acute management and surgical timing of the multiligament-injured knee. Instr Course Lect. 2015;64:521-530.
- Jiang W, Yao J, He Y, Sun W, Huang Y, Kong D. The timing of surgical treatment of knee dislocations: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2015;23(10):3108-3113. doi:10.1007/s00167-014-3435-1
- Miller MD, Wiesel SW. Operative techniques in sports medicine surgery. Lippincott Williams & Wilkins; 2012.
- Romeyn RL, Jennings J, Davies GJ. Surgical treatment and rehabilitation of combined complex ligament injuries. N Am J Sports Phys Ther. 2008;3(4):212-225.
- Gulabi D, Erdem M, Bulut G, Saglam F. Neglected patellar tendon rupture with anterior cruciate ligament rupture and medial collateral ligament partial rupture. Acta Orthop Traumatol Turc. 2014;48(2):231-235.
Tables
![Table 1. Anatomic classification of knee dislocations using Schenck classification with Wascher modification.[10]](https://eurasianmedicine.com/archive/vol7/issue3/10.4328-ECAM.10014/table-1.png)
![Table 2. Primary and secondary stabilizing structures of knee.[7]](https://eurasianmedicine.com/archive/vol7/issue3/10.4328-ECAM.10014/table-2.png)
Figures
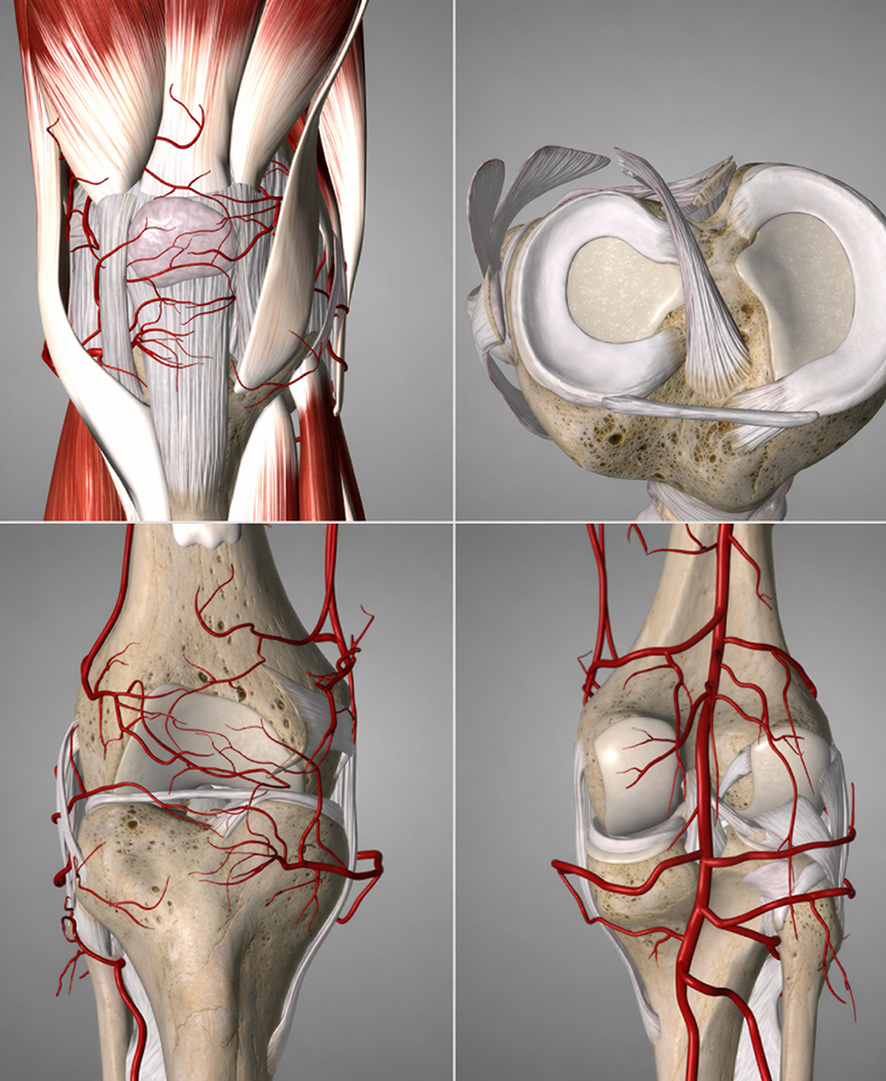
Figure 1. MRI scan has shown total rupture of ACL, PCL, MCL, Patellar tendon and meniscal tear
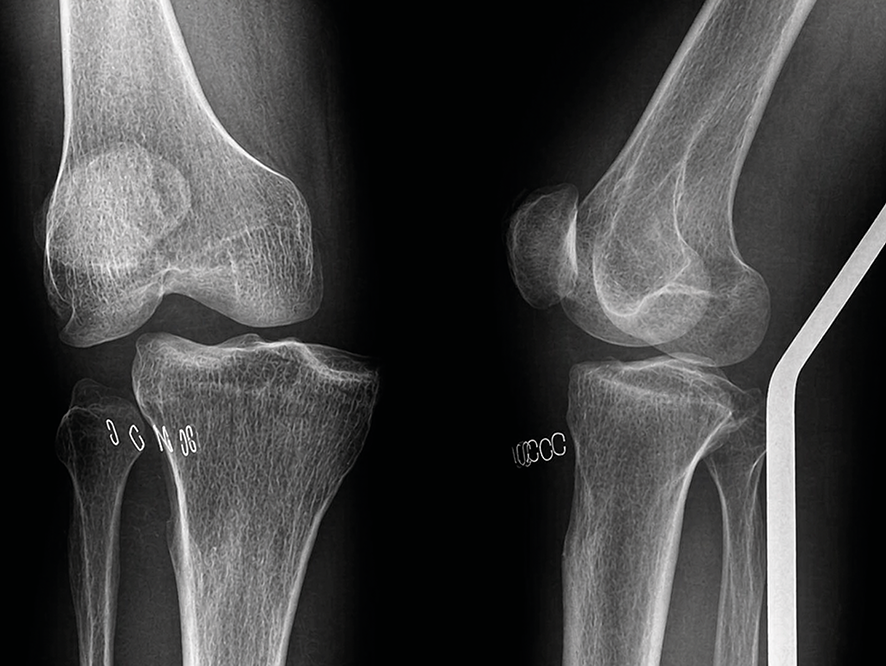
Figure 2. Anteroposterior and lateral radiography of a patient with rotational dislocation of right knee
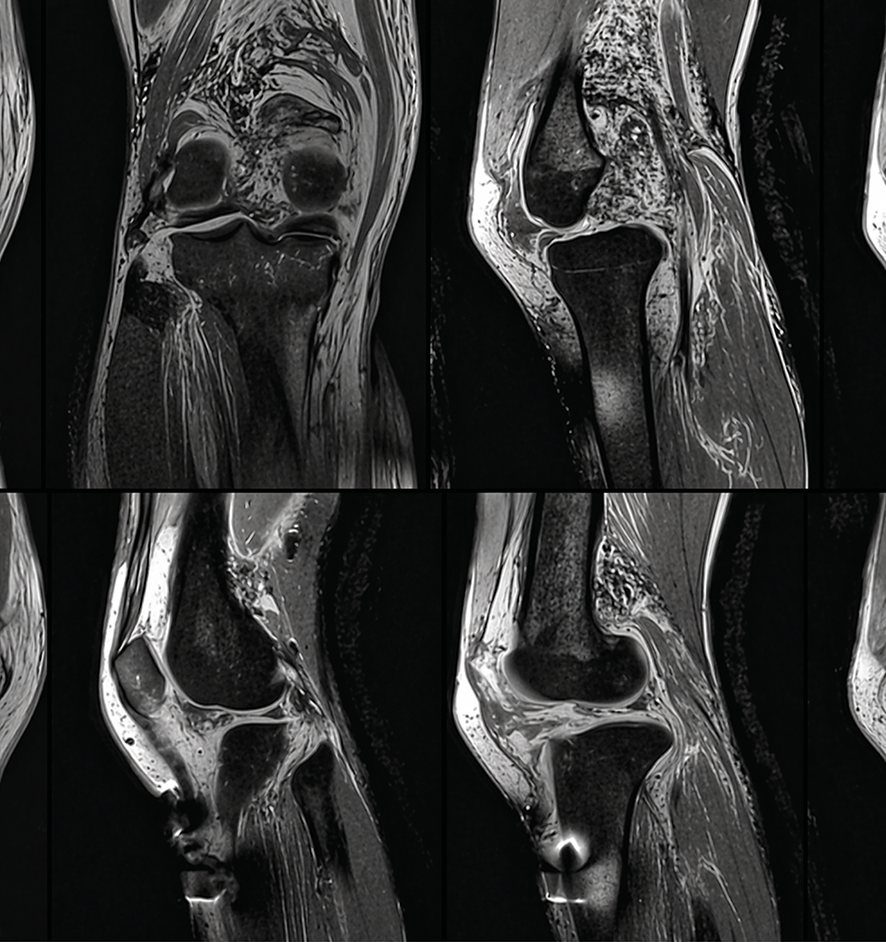
Figure 3. Anteroposterior and lateral radiography of a patient with rotational dislocation of right knee

Figure 4. Knee anatomy and vascular supply
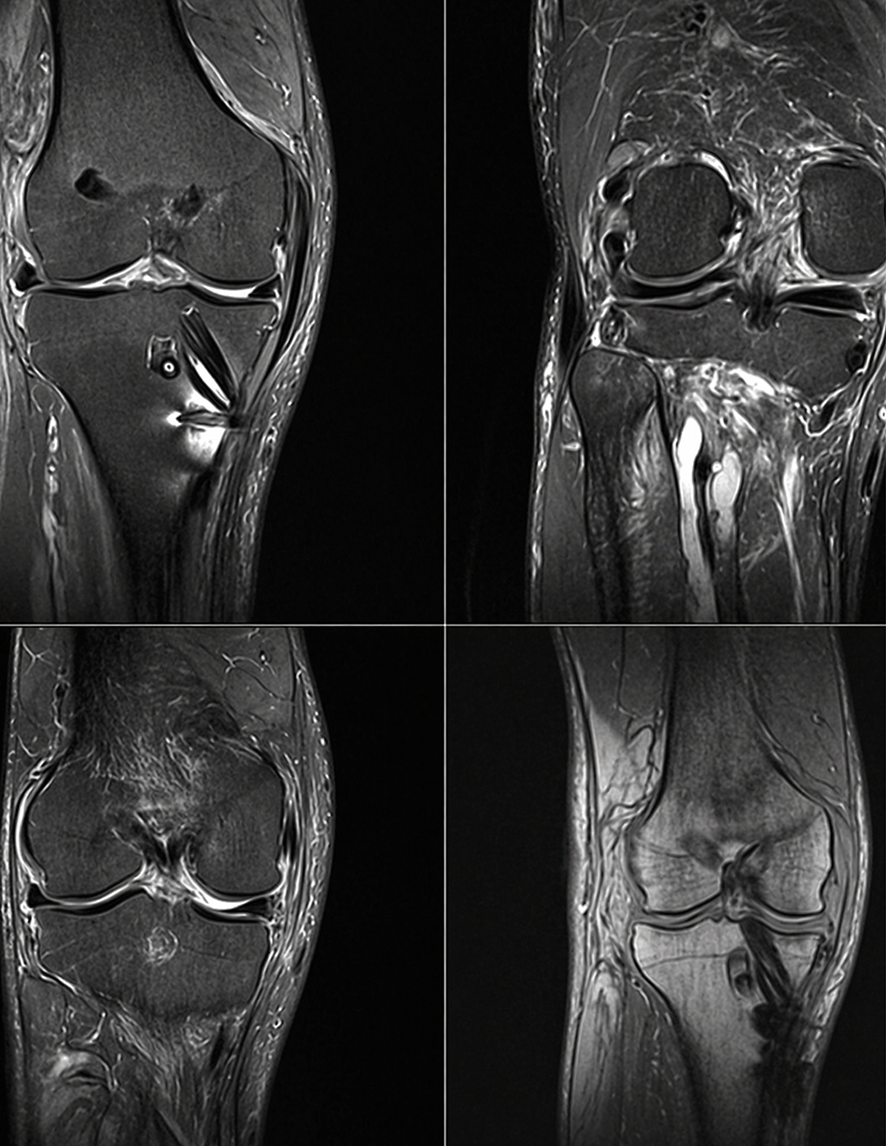
Figure 5. MRI scans of a multiligament injured knee, postoperative 6th month; ACL, PCL, PT, MCL and the meniscal structure was intact, the LCL was re-ruptured.
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Ozgur Basal, Recep Dinçer. Multiligament injury and knee dislocation: current approaches tosurgical management. Eu Clin Anal Med 2026;7(3):22. doi:10.4328/ECAM.10014
- Received:
- 13.08.2019
- Accepted:
- 12.09.2019
- Published Online:
- 12.09.2019
- Printed:
- 01.09.2019