Abstract
AimThis study is to investigate the comparison of the pre-diagnosis vs final diagnosis of the cases consulted to the perinatology specialist who started working in state hospital.MethodsThis retrospective study included 527 pregnant women who had presented to the Department of Obstetrics and Perinatology. Data included age, gestational week, and various fetal congenital or structural anomalies. In the presence of any of the following, women were excluded from the study: incomplete clinical or hospital data.ResultsDuring the study period, 527 pregnant women were analyzed. Of 527 pregnant women, 214, 174, and 136 were shown at least suspected fetal congenital or structure anomalies on ultrasonography findings by obstetricians, perinatology specialists, and newborn, respectively. The reasons for consulting perinatology were examined, it was observed that the most the common cause was fetal anomaly screening with 44.7%. The percentage of obstetricians requesting perinatology consultation according to their work experience and the institution they graduated from, it was observed that physicians with more than five years of work experience and training in education and research clinics wanted less consultation. In the obstetrician’s and perinatology specialist’s evaluation, On ultrasonography revealed that the suspected anomalies were diagnosis of the 56.4%) and 46.9%), respectively. Diagnostic performances of obstetricians compared to perinatology specialists according to birth diagnosis; the accuracy rate was 63.5% and 76.2%, respectively.ConclusionThe top three reasons for consulting a perinatology specialist were fetal anomaly screening delivery timing, and fetal anomaly suspicion.
Keywords
Introduction
Perinatology specialist is defined as a sub-branch after gynecology and obstetrics specialty.1 Perinatology specialists, together with other disciplines, fetal anomalies and high-risk pregnancies in the perinatal period were diagnosed by gynecology and obstetrics specialty or perinatology specialists.1
The American College of Obstetricians and Gynecologists (ACOG), The Society for Maternal-Fetal Medicine (SMFM), and the Association of Perinatology Specialists (PUDER) have published a recommendation for the perinatology specialists and obstetricians to work in coordination both in the United States of America (USA) and in our country.1-2-3 PUDER recommended working in collaboration with obstetricians and perinatology specialists in harmony on the detection of fetal anomalies, diagnosis, and management of high-risk pregnancies, deciding on the timing of delivery, and the need for invasive diagnostic methods.1 Although perinatology clinics in our country are becoming more and more professional each year, there is still a need for both perinatology specialists and obstetricians to work in more up-to-date cooperation and harmony, especially in rural areas.
In this study, we aimed to investigate the diagnostic differences between obstetricians and perinatologists in the diagnosis and management of patients after the perinatology specialist started to work for the first time in our rural hospital. This study aims to reduce maternal and fetal mortality and morbidity in the perinatal period by diagnosing/managing. The patients were consulted to the perinatology outpatient clinic due to suspected abnormality by 13 obstetricians. Obstetricians’ pre-diagnosis, perinatology specialist final diagnosis, and newborn diagnosis of the patients were compared between the two groups.
Materials and Methods
Study Design and ParticipantsThis retrospective study included 527 pregnant women who had presented between January 1, 2018,-2020 to the Department of Obstetrics and Perinatology of Batman state hospital in Batman, a secondary care facility performing nearly 21,000 pregnant women presented to obstetric outpatients clinic each year. Data included age at presentation, gestational age, and various fetal gross congenital or structural anomalies (fetal major/minor anomaly, Intrauterine growth retardation (IUGR)/ Small for gestational age (SGA), Oligohydramnios/Polyhydramnios, Placental disorders, etc.) at before delivery and newborn
Inclusion criteria included between 16 and 46 years, pregnancy, gestation of week, and at delivery time. In the presence of any of the following, women were excluded from the study: incomplete clinical or hospital data.Ethical ApprovalThe study was approved by the Batman Training and Research Hospital Ethics Committee (Date: 16.07.2020, Decision No: 2020-04).Statistical AnalysisData were processed using the Statistical Package for Social Sciences (SPSS) version 26 (IBM Corp., Armonk, N.Y.; USA). For pairwise comparisons and multigroup comparisons of nominal variables was Pearson’s Chi-square(χ²) test. Mean Standard Deviation, Median, and IQR values were given in descriptive statistics for continuous data, and number and percentage values were given in discrete data. All variables were expressed with 95% confidence intervals (CI). p<0.05 value is accepted as statistically significant.Reporting GuidelinesThe study was reported in accordance with STROBE guidelines.
Results
During the study period, a total of 758 pregnant women were consulted at the perinatology outpatient clinic by obstetricians. Of pregnant women, 231 had incomplete clinical or hospital data. As a result, 527 pregnant women were analyzed.
The sociodemographic and obstetric characteristics of the participants are summarised in Table 1. Of 527 pregnant women, 214, 174, and 136 were shown at least suspected fetal congenital and/or structure anomalies on ultrasonography findings by obstetricians, perinatology specialists, and newborn, respectively. The reasons for consulting perinatology were examined, it was observed that the most the common cause was fetal anomaly screening with 44.7%.
When the percentage of obstetricians requesting perinatology consultation according to their work experience and the institution they graduated from, it was observed that physicians with more than five years of work experience and training in education and research clinics wanted less consultation (Table 2, Figure 1).
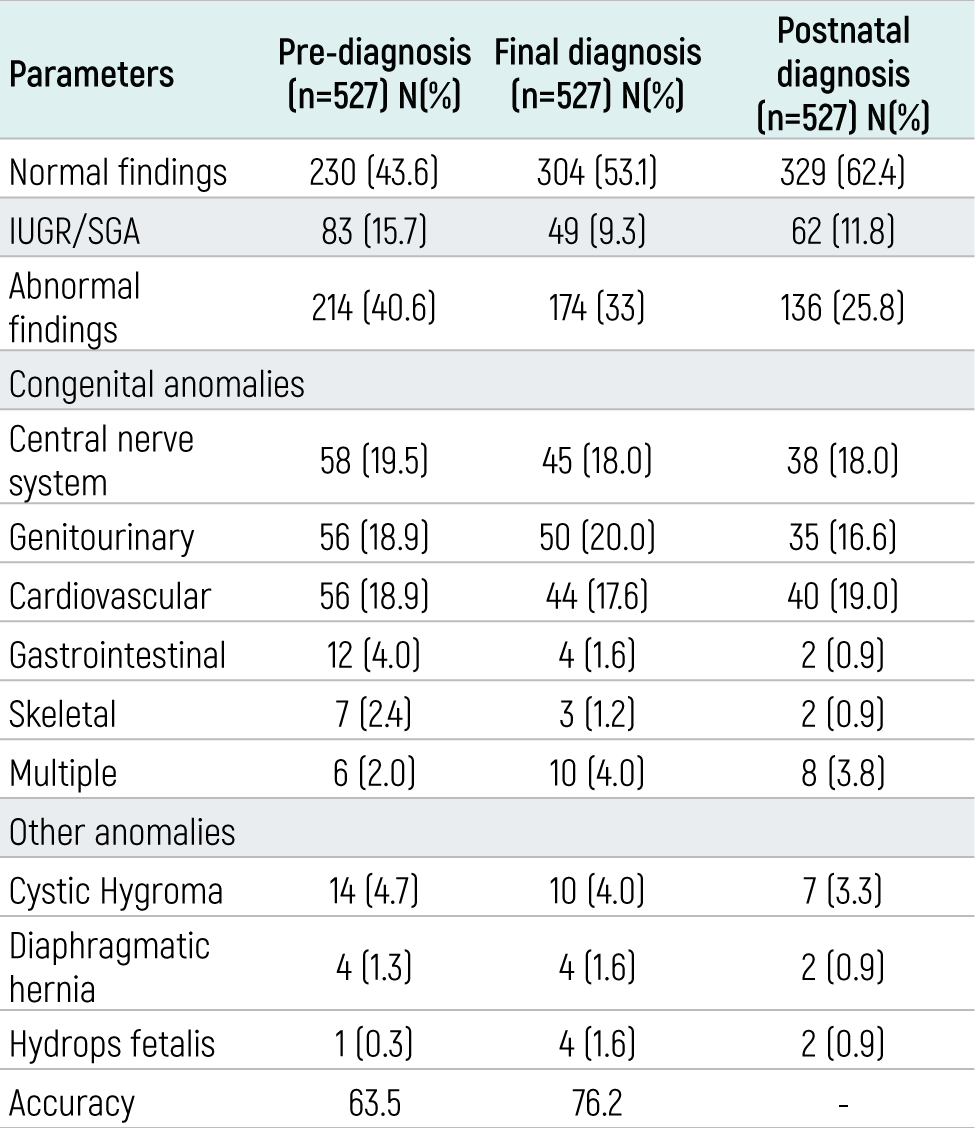
In the obstetrician’s evaluation, On ultrasonography revealed that the suspected abnormalies were diagnosis of the 297 (56.4%). The majority of anomaly consisted of IUGR/SGA, followed by central nerve system, genitourinary, and cardiovascular system. In the perinatology specialist’s evaluation, who made the diagnosis of 223 (46.9%) of the patients. The majority of anomaly was detected genitourinary system, followed by IUGR/SGA, central nerve system, and cardiovascular system. Newborn was made the final diagnosis of 298 (37.6%) of the patients. The majority of anomalies were cardiovascular system, followed by Central nerve system, genitourinary system, and IUGR/SGA. Diagnostic performances of obstetricians compared to perinatology specialists according to birth diagnosis; the accuracy rate was 63.5% and 76.2%, respectively (Table 3).
Discussion
Perinatology specialists are mostly limited to obstetricians in rural cities where they have the opportunity to work multidisciplinary in cities with a higher socioeconomic and development level. Even if the working styles of perinatologists in the world are affected by the patient population, the practice of referral from specialist physicians, and the preferences of obstetricians, it offers a unique opportunity to prevent perinatal mortality/morbidity,4,5 with the perinatology specialist starting to work in the secondary branch center for the first time throughout its history; In the diagnosis/treatment decisions of pregnant women, obstetricians and perinatology specialists started to manage patients together.6
In our study, while the diagnostic performance of obstetricians with 13 different professional experiences and perinatology specialist were compared with newborn findings, the accuracy rate was determined as 63.5% and 76.2, respectively. We considered that multiple factors contributed to this low rate, such as pregnancies without follow-up, pregnant women with irregular follow-up, clinical experience of obstetricians, differences on ultrasonographic device technical characteristics of obstetricians, and compatibility between obstetricians working with a perinatologist for the first time can be listed.
Although there were discrepancies between the diagnostic performance rates, which draws our attention to our data, this discrepancy was not observed when newborn diagnoses were compared with perinatology final diagnoses. Naturally, reasons such as working practices, medicolegal hesitations, geographical problems, abilities, and work motivations of obstetricians or perinatologists working in a secondary center who did not have a perinatology inpatient service appear as variables in their practical approaches. The top three reasons for consulting a perinatology specialist were fetal anomaly screening delivery timing, and fetal anomaly suspicion. We consider that the reason why the diagnosis of the timing of birth and the suspected fetal anomaly is so high was due to the medicolegal reservations of the obstetricians.
The patients who were consulted to the perinatology specialist; while obstetricians were compared according to their work experience and the institutions, they graduated from it was observed that those with five or more years of work experience were consulted to perinatology at a lower rate (78% vs. 22%). However, due to the fact that multiple factors (such as the variability of pregnancy rates without follow-up among physicians) played a role in the formation of this difference, the effect of our result was limited. In addition, when the institutions they graduated from were compared (University vs. Education and Research Hospital), the percentage differences due to the variables in the diagnoses of the patients who applied to the physicians prevented us from reaching a definite conclusion. Another limitation of our study was the comparison of maternal/fetal mortality/morbidity rates before & after the perinatology specialist.
Limitations
Although our study includes a considerably large sample size of patients, it is limited to one center and one perinatology specialist. More studies from our countries are needed the perinatology specialist and obstetricians, particularly rural areas.
Conclusion
Based on the results of our study, it is obvious that the need for perinatology specialists will increase with each passing year, and it will become a necessity to benefit from the experience of obstetricians and simultaneous pregnancy management. We see those perinatology specialists who take an active role in management together with obstetricians need professional solutions for work efficiency.
Declarations
Ethics Declarations
The authors declare that all procedures performed in this study were conducted in accordance with institutional, national, and international ethical standards.
Informed Consent
Due to the retrospective design of the study, the requirement for informed consent was waived by the Ethics Committee.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
None of the authors received any type of financial support that could be considered potential conflict of interest regarding the manuscript or its submission.
Funding
None.
Abbreviations
ACOG: American College of Obstetricians and Gynecologists
CI: Confidence interval
IUGR: Intrauterine growth restriction
IQR: Interquartile range
PUDER: Perinatology and Perinatal Medicine Specialists Association
SGA: Small for gestational age
SMFM: Society for Maternal-Fetal Medicine
SPSS: Statistical Package for the Social Sciences
STROBE: Strengthening the Reporting of Observational Studies in Epidemiology
References
- Altınordu Atcı A, Doğru Ş, Akkuş F. Türkiye’de kadın hastalıkları ve doğum hekimlerinin perinatoloji uzmanı görev tanımları hakkındaki farkındalıkları. Pam Tip Derg. 2022;15:682-692.
- Wenstrom KD, D’Alton ME, O’Keefe DF. Maternal-fetal medicine workforce survey: are we ready for regionalized levels of maternal care? Am J Perinatol. 2018;35(11):1044-1049.
- Sisson MC, Witcher PM, Stubsten C. The role of the maternal-fetal medicine specialist in high-risk obstetric care. Crit Care Nurs Clin North Am. 2004;16(2):187-191. doi:10.1016/j.ccell.2004.02.007
- Berlin L. Radiologists versus perinatologists when interpreting prenatal ultrasound examinations. AJR Am J Roentgenol. 2012;199(6):W781.
- Chervenak FA, Makatsariya A, Bitsadze V, McCullough LB. Perinatal critical care and ethics in perinatal medicine: the role of the perinatologist. J Perinat Med. 2017;45(9):991-997. doi:10.1515/jpm-2016-0324
- Sciscione A, Berghella V, Blackwell S, et al. Society for Maternal-Fetal Medicine Special Report: the maternal-fetal medicine subspecialists’ role within a health care system. Am J Obstet Gynecol. 2014;211(6):607-616. doi:10.1016/j.ajog.2014.09.013
Tables
Table 1. Socio-demographic, obstetric characteristics and reasons to consult a perinatologist
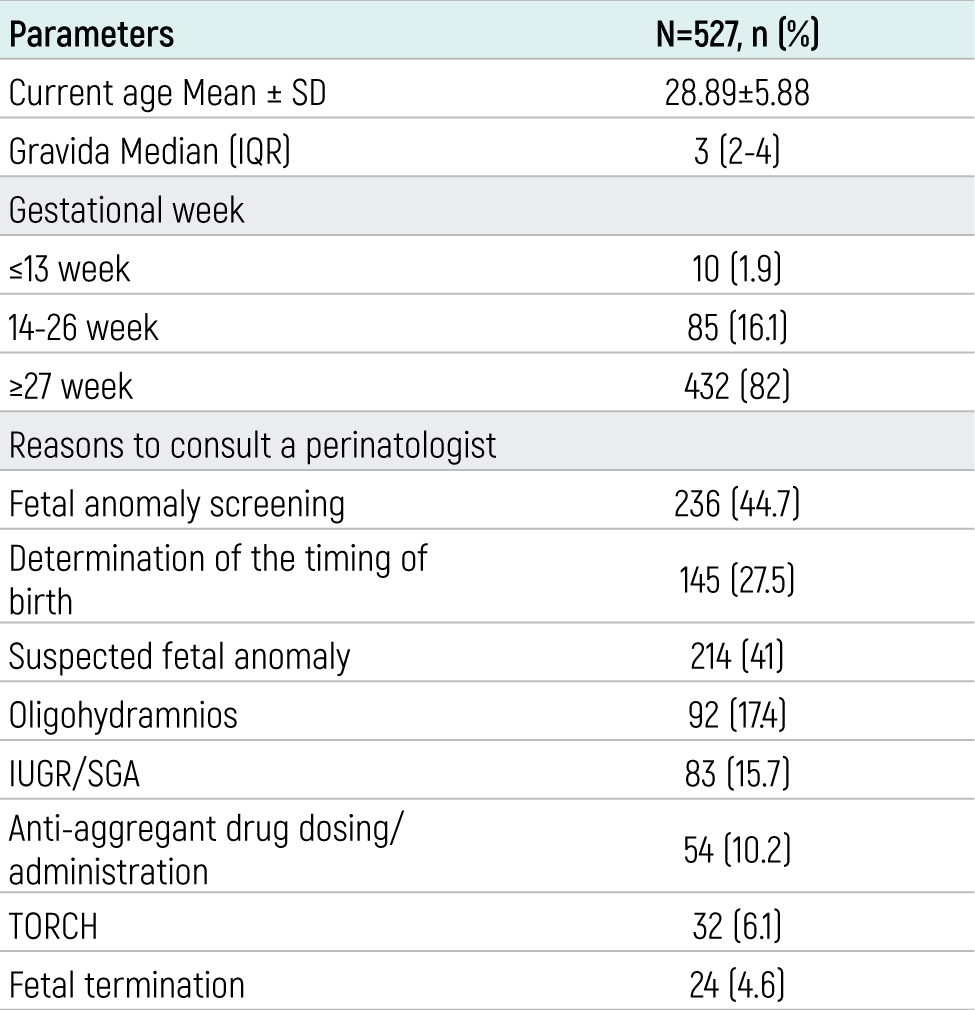
Table 2. Perinatology consultation rates by obstetricians according to their work experience and education institution
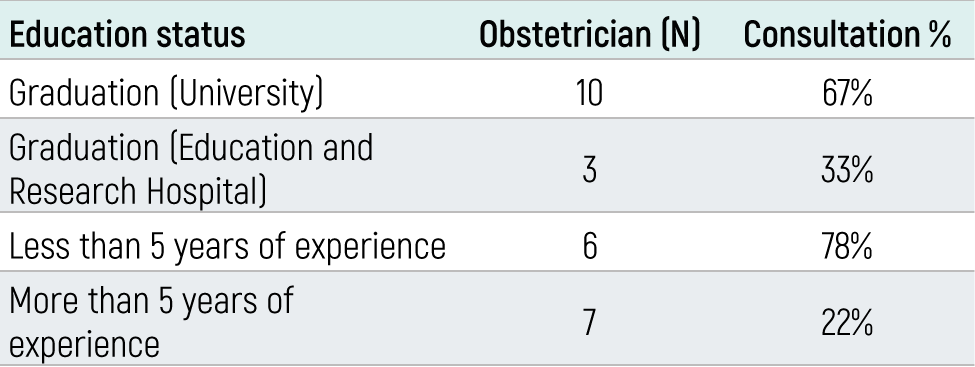
Table 3. The distributions pre-diagnosed made by obstetricians and final diagnoses made by perinatology specialists, postnatal diagnosis of patients, and diagnostic performance
Figures
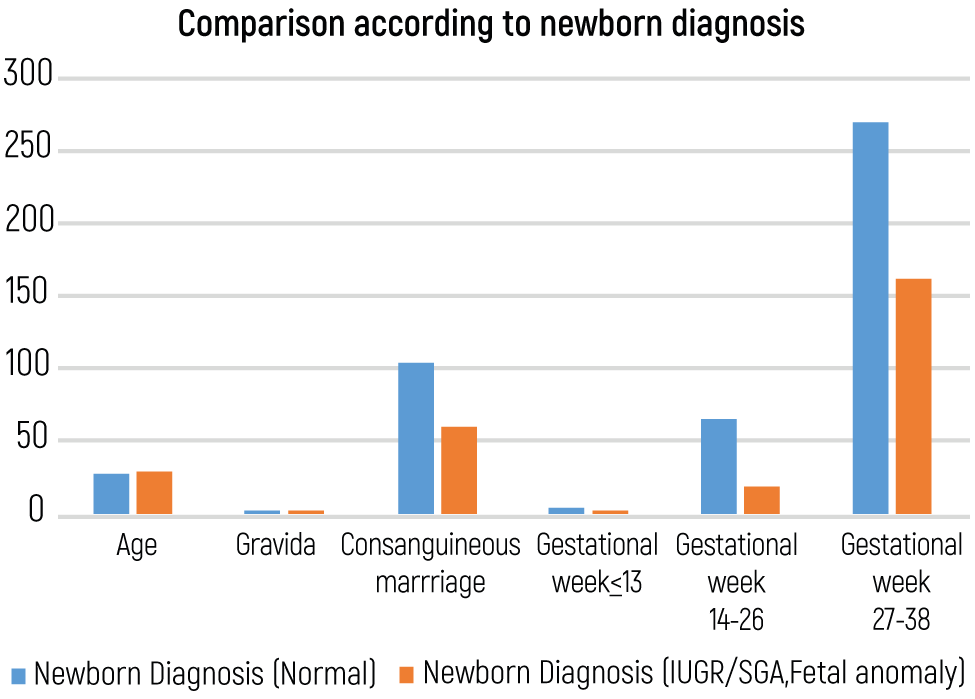
Figure 1. Comparison of maternal age, the number of births, consanguineous marriage, gestational week of patients according to newborn diagnosis
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Adil Barut, Erhan Okuyan, Lena Tureyici, Selahattin Mısırlıoglu, Özgür Çoban. The actual need for perinatal screening for pregnant women: a validation analysis. doi:10.4328/ECAM.10059
- Received:
- 27.08.2023
- Accepted:
- 12.10.2023
- Published Online:
- 14.10.2023
- Printed:
- 15.10.2023