Abstract
AimThe purpose of this in vitro study was to evaluate the working length determination of four electronic apex locators (EALs): iPex, Apex ID, MM Control and Root ZX.MethodsThe actual working length of thirty-five extracted human teeth was determined visually as 0.5 mm short of the apical foramen. After the actual working length measurements, the electronic working length was measured with four different EALs (iPex, Apex ID, MM Control and Root ZX). The measurements were repeated three times by different operators. The data were analyzed using ANOVA and Bonferroni post hoc tests. The significance level was set at p ≤ 0.05.ResultsThe mean differences between electronic and actual working length were -0.403 mm, 0.086 mm, 0.027, and 0.094 mm for the iPex, MM Control, the Root ZX, and the Apex ID, respectively. Multiple paired comparisons also showed that iPex was significantly different from other EALs.Conclusion All EALs showed an acceptable determination of the working length between the ranges of ±0.5mm except for the iPex device, which had the lowest accuracy. Further studies may be beneficial especially to better evaluate the accuracy of the iPex.
Keywords
Introduction
Root canal treatment (RCT) procedures should be confined within the root canal system. The working length (WL) is defined as the distance between a coronal reference point and the point at which canal preparation and obturation should terminate.1 Commonly, the minor apical foramen or apical isthmus is considered the end of the area for canal preparation and filling. The minor apical foramen is the border line between the dental pulp and periodontal area, which is approximately 0.5-1 mm from the anatomic apex.1 Failure to determine the root canal length can result in both over- and underestimation of the root canal length, which later causes failure of root canal treatment.2
The use of electronic devices to determine the WL was proposed first by Custer3 in 1918, and the first electronic apex locator (EAL) was developed following the investigation by Suzuki4 of the electrical resistance properties of oral tissues. The function of EALs is based on measurement of alternating current impedances. To accomplish these measurements, 2 or more different frequencies are used and processed by using different mathematical algorithms.5 These EALs are widely accepted by dentists because they are more accurate than radiographs and can reduce the number of diagnostic radiographs required to obtain working length determinations.6 The first generation of EALs was based on resistance, whereas the second generation worked on the basis of impedance. The main drawback of both these types, namely poor accuracy in the presence of electrolytes, was overcome by the introduction of third-generation EALs such as the Root ZX (J. Morita Corp, Tokyo, Japan)7 The Root ZX apex locator is considered to be the gold standard against which newer EALs are evaluated.8 The Fourth generation EALs measure capacitance and resistance simultaneously to determine the location of the file tip in the canal.8 One of them is Apex ID (SybronEndo, Orange, CA, USA), which operates on the same principle as Root ZX II (for 0.5 and 5 kHz), localizing the AF with the same accuracy as this later one.3,4 The other one is the iPex (NSK, Tochigi, Japan), its precision has only been evaluated in vitro.8 MM Control (Micro Mega, Besancon, France) provides simultaneous length control during root canal preparation. There has been no study comparing their precision with each other. Therefore, the present study aimed to assess the accuracy of 3 recently developed EALs, that use different operating mechanisms, iPex, Apex ID and MM Control, to detect the WL and to compare their accuracy with each other and to compare their precision with that of Root ZX, accepted as the gold standard.
Materials and Methods
Preparation of TeethThirty-five human maxillary central incisors extracted for periodontal or orthodontic reasons were selected. The selected teeth had a single canal and fully formed roots and were devoid of caries, endodontic treatments, and restorations. Specimens were radiographed buccolingually and mesiodistally to identify aberrant canal morphology and confirm the presence of a single canal. The teeth were then placed in a 5.25% sodium hypochlorite for 2 hours. Soft tissue and calculus remnants were removed with an ultrasonic scaler. After being cleaned, each root was carefully examined by stereomicroscopy (Meiji Techno, Saitama, Japan) at 10× magnification for the detection of external cracks, open apices, or apices undergoing resorption, which might alter the accuracy of the WL measurements. After microscopic examination, the teeth were stored in a 2% thymol solution at room temperature and used within one week. The teeth were decoronated at the cementoenamel junction, and Gates-Glidden drills (Dentsply-Maillefer, Ballaigues, Switzerland) numbers 1 through 3 were used to flare the coronal two thirds of each root canal. A sodium hypochlorite solution (1%) was used for irrigation during the process, and the patency of the apical foramen was maintained with a #10 K-file.Actual Working Length (AWL) Determination Under MicroscopeThe root canal length was determined under 20× magnification (Carl Zeiss GmbH, Oberkochen, Germany) of the stereomicroscope. A #15 K-file with a silicone stop was advanced apically until the tip was visible at the level of the most coronal border of the apical foramen; when the tip was visible, the stop was stabilized at the coronal edge of the tooth, the file was removed, and the distance between the stop and the file tip was measured with a digital caliper (TCM, Tchibo GmbH, Hamburg, Germany) to the nearest 0.01mm. Each measurement was repeated twice and the average value was recorded. Then, 0.5 mm was subtracted from the average value and the result was recorded as the actual working length (AWL).5Electronic Working Length (EWL) DeterminationAfter access preparation, the teeth were embedded in an alginate model. The working length was determined for each canal using four EALs following the manufacturers’ instructions. All canals were irrigated with 2.5% solution of sodium hypochlorite. The lip electrode was immersed in the respective orifice in contact with the conductive medium, and the same size K-file used for the AWL measurement was then connected to the other electrode for electronic measurement. For each one of the appliances, the file was gently inserted into the root canal until the ‘APEX’ signal was seen on the LED or display screens. This reading was confirmed by the audible signal emitted from the EAL. A rubber stop was then carefully adjusted to the reference level, and the distance between the rubber stop and the file was measured with the digital caliper to the nearest 0.01 mm. Because four EALs were used with each canal, we alternated the first EAL to be used in each successive canal. After finishing the EWL measurements of all specimens with the first EAL, we reinserted the same size K-file to determine the working length using the second, third and fourth EALs and measured in the same manner. To assess the repeatability, each measurement was made with each electronic device in triplicate, and the mean value was calculated and recorded as the EWL. EWLs were compared with AWLs by deducting the AWL from the EWL. A resulting positive value indicates that the EWL exceeds the AWL, while a negative value indicates that EWL measurement is short of the AWL.Ethical ApprovalEthical approval was not required for this in vitro study.Statistical AnalysisStatistical analysis was performed using MedCalc Statistical Software, version 12.7.7 (MedCalc Software bvba, Ostend, Belgium; http://www.medcalc.org; 2013). The data were analyzed using ANOVA and Bonferroni post hoc tests. The significance level was set at p≤0.05.Reporting GuidelinesNo specific reporting guideline was applicable to this in vitro study.
Results
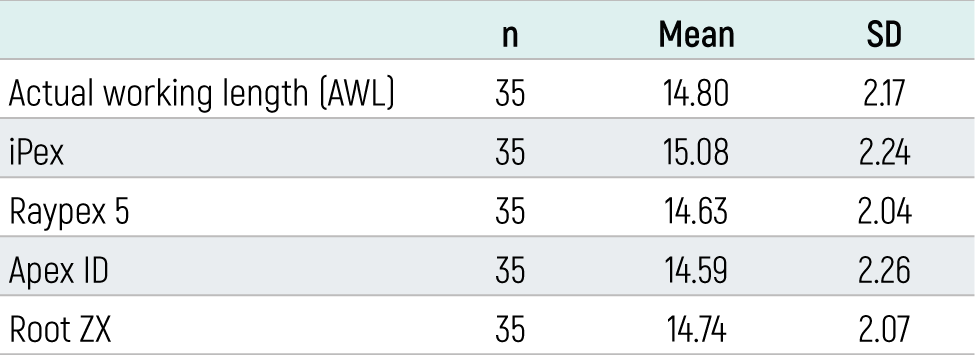
The means and standard deviations for the measurements obtained with each EAL are shown in Table 1. The mean differences between electronic and actual working length were -0.403 mm, 0.086 mm, 0.027, and 0.094 mm for the iPex, MM Control, the Root ZX, and the Apex ID, respectively.
Multiple paired comparisons (Bonferroni test) also showed that iPex was significantly different from the MM Control, the Root ZX, and the Apex ID (p = 0.001, p = 0.000, and p = 0.001, respectively). No significant differences were found between MM Control and Root ZX (p = 1.000) or between MM Control and Apex ID (p = 1.000) or between Root ZX and Apex ID (p = 1.000). The accuracy of the iPex, MM Control, Apex ID and Root ZX in locating the minor diameter within ±0.5 mm was 50%, 90%, 88%, and, 94% respectively.
Discussion
The recently introduced fourth-generation EALs are claimed by their manufacturers to be successful in WL determination. Given the absence of reports related to the accu¬racy of the 4th generation EALs, the aim of this study was to evaluate the ability of 3 developed EALs, iPex, Apex ID and MM Control to detect the WL and compare their accuracy with each other and with that of a third-generation gold standard EAL (Root ZX).
Among the four EALs tested, the MM Control, the Root ZX, and the Apex ID showed similar and more accurate WL measurements when compared with iPex. The results showed that there was no significant difference in the accuracy between the MM Control, the Root ZX, and the Apex ID in determining the WL. Considering a clinically acceptable variation of ±0.5 mm in relation to the actual WL (control) as suggested by various studies,9,10 the results of the present study showed 90%, 94%, and 88% accuracy for the MM Control, the Root ZX, and the Apex ID, respectively, in relation to the control measurement. Within the limits of ±1 mm, these 3 EALs measured the WL accurately over 90.6% of specimens. These results are in line with previous findings,9-10-11 These results indicate that the accuracy of 4th generation EALs is enhanced compared to Root ZX.
The present methodology used an in vitro model. Some authors have compared the accuracies of EALs in establishing the final working lengths under in vivo and in vitro conditions and concluded that these accuracies are not significantly different between the in vivo and in vitro models.12 However, it is important to highlight that there was no direct comparison of in vivo and in vitro techniques because the teeth used were not the same teeth.13 Precise comparison of the accuracy of different types of EAL in determining the WL is possible only if the same teeth are assessed by all the devices. Therefore, we fol¬lowed the protocol used by Wrbas et al.,14 which al¬lowed us to calculate the accuracy of the four EALs in the same teeth. The diameter and location of the AC are factors affecting the accuracy of EALs. In order to avoid the effects of these factors, only single-rooted premolars and incisors were included in the present study. Pre-flaring of root canals before measurement with EALs can increase the precision of WL determination.15 Thus, the canals were pre-flared in the current study before WL measurement.
Conclusion
All EALs showed an acceptable determination of the working length between the ranges of ±0.5mm except for the iPex device, which had the lowest accuracy. Further studies may be beneficial especially to better evaluate the accuracy of the iPex.
Declarations
Informed Consent
Not applicable.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare no conflict of interest.
Funding
None.
Abbreviations
AWL: Actual working length
EAL: Electronic apex locator
EWL: Electronic working length
RCT: Root canal treatment
WL: Working length
References
- Thorley W. Working length determination. Br Dent J. 2021;230(1):5. doi:10.1038/s41415-020-2562-y
- Chen C, Zhang W, Liang Y. Evaluation of apical root defects during canal instrumentation with two different nickel-titanium systems by optical coherence tomography scan. J Dent Sci. 2022;17(2):763-770. doi:10.1016/j.jds.2021.10.009
- Custer LE. Exact method of locating the apical foramen. Dent Regist. 1918;72(9):420-425.
- Suzuki K. Experimental study on iontophoresis. Jpn J Stomatol. 1942;16:411-429.
- Nekoofar MH, Ghandi MM, Hayes SJ, Dummer PM. The fundamental operating principles of electronic root canal length measurement devices. Int Endod J. 2006;39(8):595-609. doi:10.1111/j.1365-2591.2006.01131.x
- Vieyra JP, Acosta J, Mondaca JM. Comparison of working length determination with radiographs and two electronic apex locators. Int Endod J. 2010;43(1):16-20. doi:10.1111/j.1365-2591.2009.01620.x
- Davalbhakta RN, Gokhale NS, Hugar SM, Badakar CM, Gowtham A, Soneta SP. Comparative evaluation of Root ZX Mini apex locator and radiovisiography in determining the working length of primary molars: an in vivo study. J Oral Biol Craniofac Res. 2021;11(2):257-262. doi:10.1016/j.jobcr.2021.02.007
- de Vasconcelos BC, do Vale TM, de Menezes AS, et al. An ex vivo comparison of root canal length determination by three electronic apex locators at positions short of the apical foramen. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;110(2):e57-e61. doi:10.1016/j.tripleo.2010.03.005
- Aydin U, Karataslioglu E, Aksoy F, Yildirim C. In vitro evaluation of Root ZX and Raypex 6 in teeth with different apical diameters. J Conserv Dent. 2015;18(1):66-69. doi:10.4103/0972-0707.148899
- Lucena C, López JM, Martín JA, Robles V, González-Rodríguez MP. Accuracy of working length measurement: electronic apex locator versus cone-beam computed tomography. Int Endod J. 2014;47(3):246-256. doi:10.1111/iej.12140
- Yolagiden M, Ersahan S, Suyun G, Bilgec E, Aydin C. Comparison of four electronic apex locators in detecting working length: an ex vivo study. J Contemp Dent Pract. 2018;19(12):1427-1433. doi:10.5005/jp-journals-10024-2444
- da Silva TM, Alves FR. Ex vivo accuracy of Root ZX II, Root ZX Mini and RomiApex A-15 apex locators in extracted vital pulp teeth. J Contemp Dent Pract. 2014;15(3):312-314. doi:10.5005/jp-journals-10024-1534
- Somma F, Castagnola R, Lajolo C, Paternò Holtzman L, Marigo L. In vivo accuracy of three electronic root canal length measurement devices: Dentaport ZX, Raypex 5 and ProPex II. Int Endod J. 2012;45(6):552-556. doi:10.1111/j.1365-2591.2011.02010.x
- Wrbas KT, Ziegler AA, Altenburger MJ, Schirrmeister JF. In vivo comparison of working length determination with two electronic apex locators. Int Endod J. 2007;40(2):133-138. doi:10.1111/j.1365-2591.2006.01199.x
- de Camargo EJ, Zapata RO, Medeiros PL, et al. Influence of preflaring on the accuracy of length determination with four electronic apex locators. J Endod. 2009;35(9):1300-1302. doi:10.1016/j.joen.2009.05.030
Tables
Table 1. Mean and standard deviation (SD) of measurements using four EALs
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Yelda Erdem Hepsenoglu, Seyda Ersahan. Comparison of working length determination with four electronic apex locators. doi:10.4328/ECAM.10061
- Received:
- 04.09.2023
- Accepted:
- 13.10.2023
- Published Online:
- 14.10.2023
- Printed:
- 15.10.2023