Abstract
AimOne of the causes of massive postpartum hemorrhage is preeclampsia, with a high risk of morbidity and mortality. Cesarean section is generally preferred for delivery in preeclamptic pregnant women and regional anesthesia is recommended in the absence of contraindications. Tranexamic acid (TXA), which has anti-fibrinolytic effect, has been shown to reduce the amount of bleeding when given within the first three hours in trauma or obstetric bleeding. For this purpose, we planned to evaluate the perioperative effects of TXA in preeclamptic patients undergoing cesarean section with spinal anesthesia.MethodsThis study was planned retrospectively after obtaining clinical ethical approval. A total of 98 preeclamptic patients who underwent cesarean section under spinal anesthesia between January 2022 and October 2022 were included in the study. Demographic data, ASA score, preoperative and postoperative laboratory values, infant APGAR scores, perioperative bleeding amount, total amount of fluid given, blood requirement, length of hospital stay and complications were evaluated.ResultsA total of 98 preeclamptic patients who underwent cesarean section under spinal anesthesia were divided into two groups: GNT (n=57) and GT (n=41). The mean age, BMI, comorbidities and duration of operation were similar in both groups. Mean preoperative Hb and Hct values and median creatinine values were higher in GNT. Median values of perioperative bleeding amounts were significantly lower in GT (p<0.05). Peroperative blood requirement was similar in both groups.ConclusionTranexamic acid can be used in obstetric patients with a high risk of bleeding on a risk-benefit ratio.
Keywords
Introduction
Postpartum hemorrhage is a life-threatening condition with high morbidity and mortality that may lead to a hysterectomy due to massive bleeding during pregnancy. This major bleeding may result in renal failure, disseminated intravascular coagulation, shock, acute respiratory distress syndrome and even the need for intensive care unit hospitalization.1 Postpartum hemorrhage has many risk factors for the mother, pregnancy and delivery. One of the pregnancy-related causes is preeclampsia.2 The only definitive preeclampsia treatment is delivery to prevent maternal hypertension and seizures and optimize fetal well-being [(https://www.nice.org.uk/guidance/ ng133)]. Cesarean section is generally preferred in pre-eclampsia. Anesthetic management and control of perioperative hemodynamics are important to prevent complications in pregnant women. Henke et al. reported that hemodynamic changes were minimally affected in cesarean section with spinal anesthesia in preeclamptic pregnant women.3 Another study showed that maternal hemodynamics was similar when spinal anesthesia was compared with general anesthesia.4 Regional anesthesia is recommended in pregnant women with preeclampsia in the absence of contraindication to the choice of anesthesia.5
Tranexamic acid (TXA) is a synthetic lysine receptor antagonist with an antifibrinolytic effect by inhibiting the interaction between plasmin and fibrin.6 TXA given in the first three hours in trauma or obstetric bleeding has decreased the amount of bleeding and the need for blood transfusion.7
For this purpose, we planned to evaluate the effect of TXA use on perioperative bleeding, blood requirement, laboratory values, hospital stay and complications in preeclamptic pregnant women operated under spinal anesthesia with high bleeding risk.
Materials and Methods
Data CollectionThis retrospective study was approved by the clinical ethics committee. Data from patients who underwent cesarean section under spinal anesthesia with a pre-diagnosis of pre-eclampsia between January 2022 and October 2022 were analyzed. Patients between 20-50 years old with a gestational age above 34 weeks were included in the study. Patients with a history of antithrombotic or anticoagulant use, concomitant placental invasion anomalies, known hypersensitivity to tranexamic acid or concentrated hydrochloric acid, cardiovascular, hepatic and renal diseases, and intraoperative general anesthesia were excluded. When the chi-square test was performed with p:0.05 significance (a), 90% test power (1-β), and d:0.5 effect size, the number of samples that should be taken in each group according to the use of tranexamic acid was determined as 53. One hundred twenty-five patients who underwent a cesarean section under spinal anesthesia with a pre-diagnosis of preeclampsia were examined, and 27 patients were excluded from the study. Patients were divided into 2 groups: the group not using tranexamic acid (GNT) and the group using tranexamic acid (GT) (Figure 1). Preoperative demographic data (age, BMI, comorbidity), ASA score, preoperative and postoperative blood hemoglobin (Hb), platelet (Plt), aspartate aminotransferase (AST), alanine aminotransferase (ALT), urea, creatinine, glomerular filtration rate (GFR), peroperative bleeding amount, the total amount of fluid given, blood requirement, Appearance Pulse Grimace Activity Respiration (APGAR) score at 1 and 5 minutes, postoperative blood requirement, hospital stay and complications were evaluated.Anesthesia ManagementIn our hospital, a six-hour fasting period is expected in patients scheduled for elective cesarean section. In the operating room, pulse oximetry, electrocardiogram, and non-invasive arterial blood pressure monitoring are routinely performed. An 18-gauge Angio-cut establishes peripheral vascular access, initiating intravenous (IV) crystalloid fluid infusion. In patients who accept spinal anesthesia, who have no contraindications to regional anesthesia and who have stable hemodynamics, 10-15 mcg bupivacaine and 20 mcg fentanyl are administered intrathecally with a 25-gauge pencil point spinal needle in the sitting position. Surgical incision is allowed after controlling the T6 level with a supine position. Patients are given oxygen through a mask. Hypotension is a 20% drop in systolic blood pressure and/or blood pressure below 90 mmHg. Patients with hypotension are administered 250 ml IV bolus crystalloid fluid and 5-10 mg IV ephedrine. A heart rate below 50/min is considered bradycardia, and 0.01 mg/kg iv atropine is administered. Tranexamic acid use varies according to the anesthesiologist’s clinical practice. Patients are administered 1 g tranexamic acid (100 ml 0.9% sodium chloride) as IV infusion in 10 minutes (min). Blood loss is calculated using aspiration cups, compresses and pads. Patients who are stable perioperatively and have a modified Aldreata score >9 in the postoperative recovery unit are transferred to the ward.Ethical ApprovalThe study was approved by the Ethics Committee of Başakşehir Çam and Sakura City Hospital (Date: 25.01.2023, Decision No: 31).Statistical AnalysisSPSS analyzed the parameters for Windows version 23.0. The Kolmogorov-Smirnov test and histogram were used to clarify whether the data were normally distributed. Continuous variables were non-normally distributed in each group; therefore, non-parametric tests were used. Continuous variables were expressed as standard deviation or median (interquartile range (IQR) 25-75), while categorical variables were expressed as n (%). The difference between continuous variables of the two groups was calculated by the Student’s T-test or the Mann-Whitney-U test. The Chi-square test was used in the analysis of categorical parameters. Changes in the perioperative findings between groups were evaluated with the mixed model for repeated measurements. P<0.05 was considered statistically significant.Reporting GuidelinesThe study was reported in accordance with STROBE guidelines.
Results
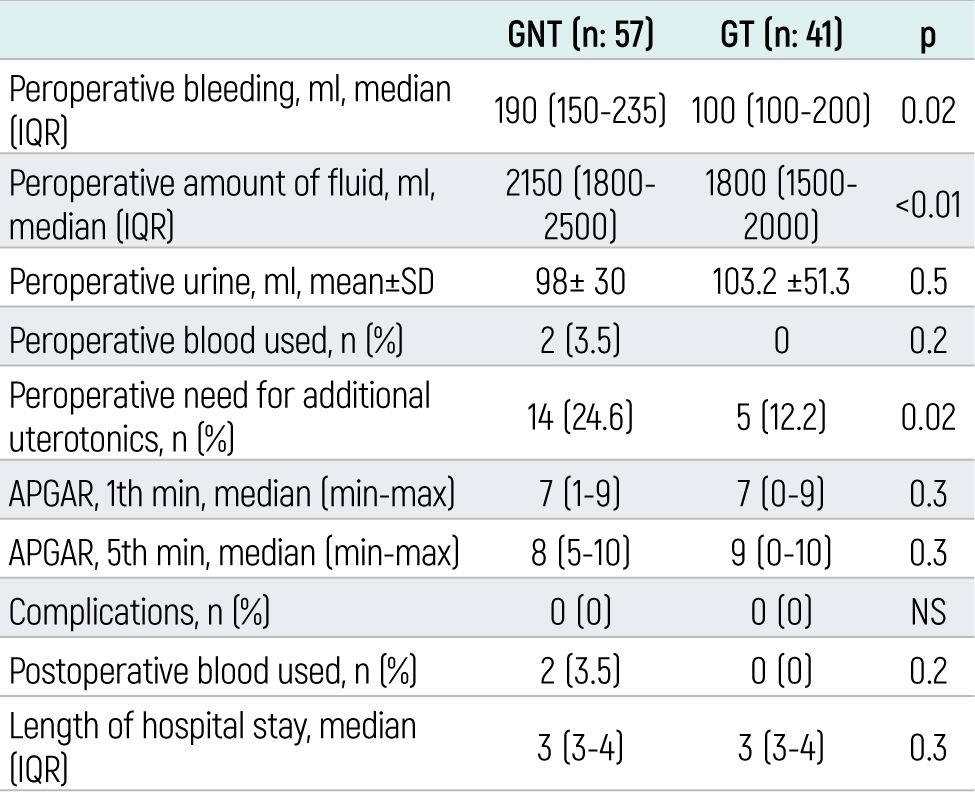
In this study, in which 125 patients were evaluated, 27 patients, 13 in GNT and 14 in GT, were excluded. A total of 98 preeclamptic patients who underwent caesarean section under spinal anesthesia were divided into two groups: GNT (n=57) and GT (n=41) (Figure 1). The mean ages of GNT and GT patients were 30±5.9 and 30±5.9 years, respectively. 5.3% of GNT patients and 17.1% of GT patients were in the ASAIII risk group. BMI, comorbidities and operation times were similar in both groups (Table 1). Preoperative and postoperative laboratory values of the patients are shown in Table 2. Mean preoperative Hb and Hct values were statistically significantly higher in GNT. Median preoperative creatinine values were higher in GNT (p<0.05). When other parameters were analyzed, AST, ALT, urea, and GFR values were similar in both groups. Postoperative laboratory values were similar in both groups (Table 2). The median values of perioperative bleeding amounts were 190 (150-235) and 100 (100- 200) for GNT and GT (p<0.05). Median values of the total amount of fluid used were statistically significantly higher in GNT. Peroperative need for additional uterotonic was higher in GNT (p<0.05). Perioperative urine volume, blood requirement and infant APGAR scores were similar in both groups (p>0.05). Postoperative hospital stays, complications and blood requirements did not differ between the two groups (Table 3).Discussion
In this retrospective study, it was observed that the amount of peroperative bleeding, the amount of fluid given peroperatively, and the need for additional uterotonics were less in patients who underwent cesarean section under spinal anesthesia with a pre-diagnosis of preeclampsia and used tranexamic acid. Perioperative blood requirement was similar in both groups.
Preeclampsia causes high morbidity and mortality for both mother and baby due to the risk of postpartum bleeding.8 The World Health Organization emphasizes the importance of tranexamic acid in the first three hours of postpartum hemorrhage [(https://www.who.int/publications-detail-redirect/WHO-RHR-17.21)]. Studies have shown the efficacy of tranexamic acid in perioperative bleeding in caesarean sections.9 Many studies have shown that the amount of bleeding was less in the group using TXA in caesarean operations compared to the control group.10-11 In meta-analyses in the literature, it has been reported that TXA reduces total blood loss. Despite all these studies, using tranexamic acid in postpartum hemorrhage in pregnant women is recommended, considering the risk- benefit ratio.12 Our study observed that the amount of perioperative bleeding decreased in the group using tranexamic acid, and the amount of fluid used decreased accordingly. Our findings are similar to other studies.
A randomized controlled study reported that the percentage of preoperative and postoperative hemoglobin change was less in the group using tranexamic acid.13 Another study observed that postoperative hemoglobin level was higher in the group using tranexamic acid.10 In our results, although the preoperative Hb level was higher in the group without tranexamic acid, there was no difference between the two groups postoperatively.
Many studies have reported that TXA reduces the need for uterotonic. Our results in the present study were similar.14
Gungorduk et al. evaluated the effect of tranexamic acid on infant APGAR scores and found no difference compared to the control group, which is similar to our findings.15
The risk of thromboembolism increases in pregnant women, and it has been shown to increase even more significantly in preeclampsia.16 TXA has serious side effects, including nausea, vomiting, diarrhea, headache, myocardial infarction and pulmonary embolism.17 In a randomized controlled study, 1 g tranexamic acid reduced the risk of perioperative bleeding without increasing the risk of postoperative thromboembolism.18 There is only one study evaluating the risk of thromboembolism in preeclamptic pregnant women, and it has been reported that tranexamic acid does not increase the risk of thromboembolism and can be used safely.19 In our study, only postoperative renal function and thromboembolism complications were evaluated, and it was observed that renal function was preserved and thromboembolism did not occur. When the renal functions of our patients were evaluated, it was shown that the use of TXA did not affect postoperative GFR. A meta-analysis showed that TXA used in patients with hematuria did not increase the risk of renal failure.20 Another study argued that it protects renal function in polycystic kidney disease by stopping hematuria attacks and preventing embolization and nephrectomy.21
Limitations
The first limitation of our study was that tranexamic acid administration time varied. The second limitation was the administration of 1 g TXA to each patient regardless of weight. Another limitation is that the drug’s long-term maternal and neonatal effects cannot be evaluated.
Conclusion
The authors declare that they are responsible for the article’s scientific content including study design, data collection, analysis and interpretation, writing, some of the main line, or all of the preparation and scientific review of the contents and approval of the final version of the article.
Declarations
Informed Consent
The requirement for informed consent was waived due to the retrospective study design.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare no conflict of interest.
Funding
None.
Abbreviations
ALT: Alanine aminotransferase
APGAR: Appearance Pulse Grimace Activity Respiration
ASA: American Society of Anesthesiologists
AST: Aspartate aminotransferase
BMI: Body mass index
GFR: Glomerular filtration rate
GT: Group using tranexamic acid
GNT: Group not using tranexamic acid
Hb: Hemoglobin
Hct: Hematocrit
IV: Intravenous
IQR: Interquartile range
Plt: Platelet
TXA: Tranexamic acid
References
- Solomon C, Collis RE, Collins PW. Haemostatic monitoring during postpartum haemorrhage and implications for management. Br J Anaesth. 2012;109(6):851-863. doi:10.1093/bja/aes361
- Neary C, Naheed S, McLernon DJ, Black M. Predicting risk of postpartum haemorrhage: a systematic review. BJOG. 2021;128(1):46-53. doi:10.1111/1471-0528.16379
- Henke VG, Bateman BT, Leffert LR. Spinal anesthesia in severe preeclampsia. Anesth Analg. 2013;117(3):686-693. doi:10.1213/ane.0b013e31829eeef5
- Dyer RA, Els I, Farbas J, Torr GJ, Schoeman LK, James MF. Prospective, randomized trial comparing general with spinal anesthesia for cesarean delivery in preeclamptic patients with a nonreassuring fetal heart trace. Anesthesiology. 2003;99(3):561-569. doi:10.1097/00000542-200309000-00010
- Gogarten W. Preeclampsia and anaesthesia. Curr Opin Anaesthesiol. 2009;22(3):347-351. doi:10.1097/aco.0b013e32832a1d05
- Cai J, Ribkoff J, Olson S, et al. The many roles of tranexamic acid: an overview of the clinical indications for TXA in medical and surgical patients. Eur J Haematol. 2020;104(2):79-87. doi:10.1111/ejh.13348
- Shakur H, Roberts I, Fawole B, et al. Effect of early tranexamic acid administration on mortality, hysterectomy, and other morbidities in women with post-partum haemorrhage (WOMAN): an international, randomised, double-blind, placebo-controlled trial. Lancet. 2017;389(10084):2105-2116. doi:10.1016/s0140-6736(17)30638-4
- Jauniaux E, Berghella V. The modern caesarean section. In: Jauniaux E, Grobman WA, eds. Textbook of Caesarean Section. 1st ed. Oxford University Press; 2016:49-68. doi:10.1093/med/9780198758563.003.0005
- Maged AM, Helal OM, Elsherbini MM, et al. A randomized placebo-controlled trial of preoperative tranexamic acid among women undergoing elective cesarean delivery. Int J Gynaecol Obstet. 2015;131(3):265-268. doi:10.1016/j.ijgo.2015.05.027
- Ali SA, Oof TF, Elmolla MF. Efficacy of intravenous tranexamic acid in reducing blood loss after elective cesarean section. Egypt J Hosp Med. 2019;74:1353-1358. doi:10.21608/ejhm.2019.26699
- Sentilhes L, Madar H, Mattuizzi A, et al. Tranexamic acid for childbirth: why, when, and for whom. Expert Rev Hematol. 2019;12(9):753-756. doi:10.1080/17474086.2019.1642744
- Wang Y, Liu S, He L. Prophylactic use of tranexamic acid reduces blood loss and transfusion requirements in patients undergoing cesarean section: a meta-analysis. J Obstet Gynaecol Res. 2019;45(8):1562-1575. doi:10.1111/jog.14013
- Shalaby MA, Maged AM, Al-Asmar A, et al. Safety and efficacy of preoperative tranexamic acid in reducing intraoperative and postoperative blood loss in high-risk women undergoing cesarean delivery: a randomized controlled trial. BMC Pregnancy Childbirth. 2022;22(1):201. doi:10.1186/s12884-022-04530-4
- Sentilhes L, Daniel V, Deneux-Tharaux C. TRAAP2-TRAnexamic acid for preventing postpartum hemorrhage after cesarean delivery: a multicenter randomized, double-blind, placebo-controlled trial—a study protocol. BMC Pregnancy Childbirth. 2020;20(1):63. doi:10.1186/s12884-019-2718-4
- Gungorduk K, Yildirm G, Asicioğlu O, Gungorduk OC, Sudolmus S, Ark C. Efficacy of intravenous tranexamic acid in reducing blood loss after elective cesarean section: a prospective, randomized, double-blind, placebo-controlled study. Am J Perinatol. 2011;28(3):233-240. doi:10.1055/s-0030-1268238
- Scheres LJJ, Lijfering WM, Groenewegen NFM, et al. Hypertensive complications of pregnancy and risk of venous thromboembolism. Hypertension. 2020;75(3):781-787. doi:10.1161/hypertensionaha.119.14280
- Calapai G, Gangemi S, Mannucci C, et al. Systematic review of tranexamic acid adverse reactions. J Pharmacovigil. 2015;3:171. doi:10.4172/2329-6887.1000171
- Sentürk MB, Cakmak Y, Yildiz G, Yildiz P. Tranexamic acid for cesarean section: a double-blind, placebo-controlled, randomized clinical trial. Arch Gynecol Obstet. 2013;287(4):641-645. doi:10.1007/s00404-012-2624-8
- Okoye HC, Othman M, Nwagha TU, Onwusulu DN, Onoh RC, Chigbu O. Evaluating the hemostatic effects of tranexamic acid in women with pre-eclampsia. Int J Gynaecol Obstet. 2023;162(3):931-936. doi:10.1002/ijgo.14779
- Lee SG, Fralick J, Wallis CJD, Boctor M, Sholzberg M, Fralick M. Systematic review of hematuria and acute renal failure with tranexamic acid. Eur J Haematol. 2022;108(6):510-517. doi:10.1111/ejh.13762
- Peces R, Aguilar A, Vega C, Cuesta E, Peces C, Selgas R. Medical therapy with tranexamic acid in autosomal dominant polycystic kidney disease patients with severe haematuria. Nefrologia. 2012;32(2):160-165. doi:10.3265/nefrologia.pre2011.dec.11210
Tables
Table 1. Demographic data of patients and operation times
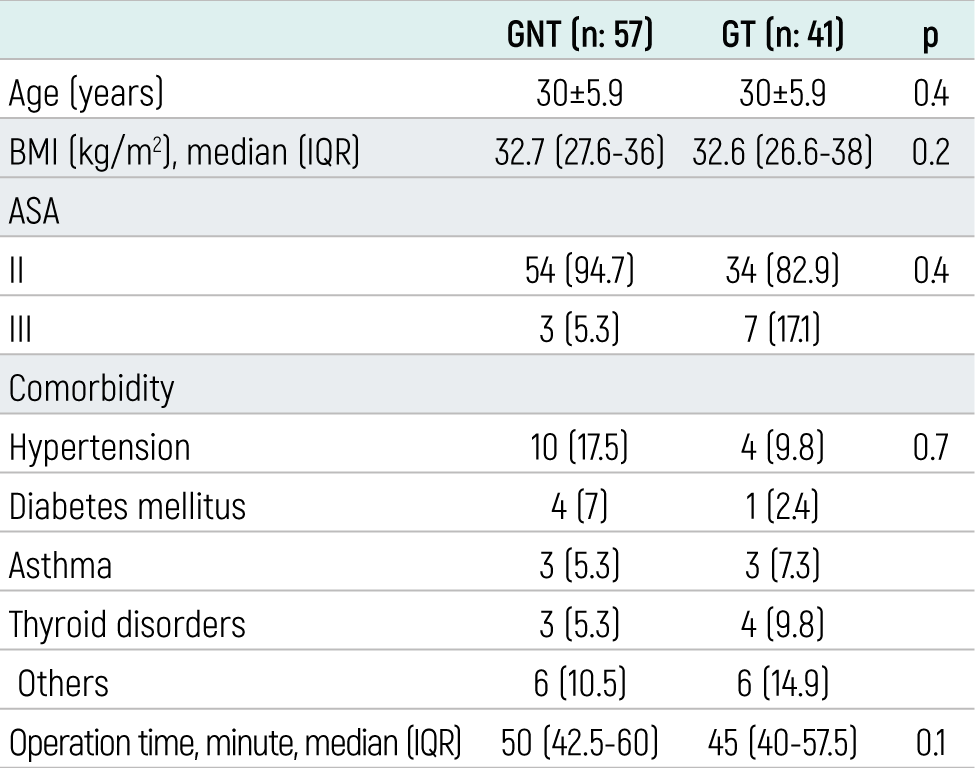
Table 2. Preoperative and postoperative laboratory values
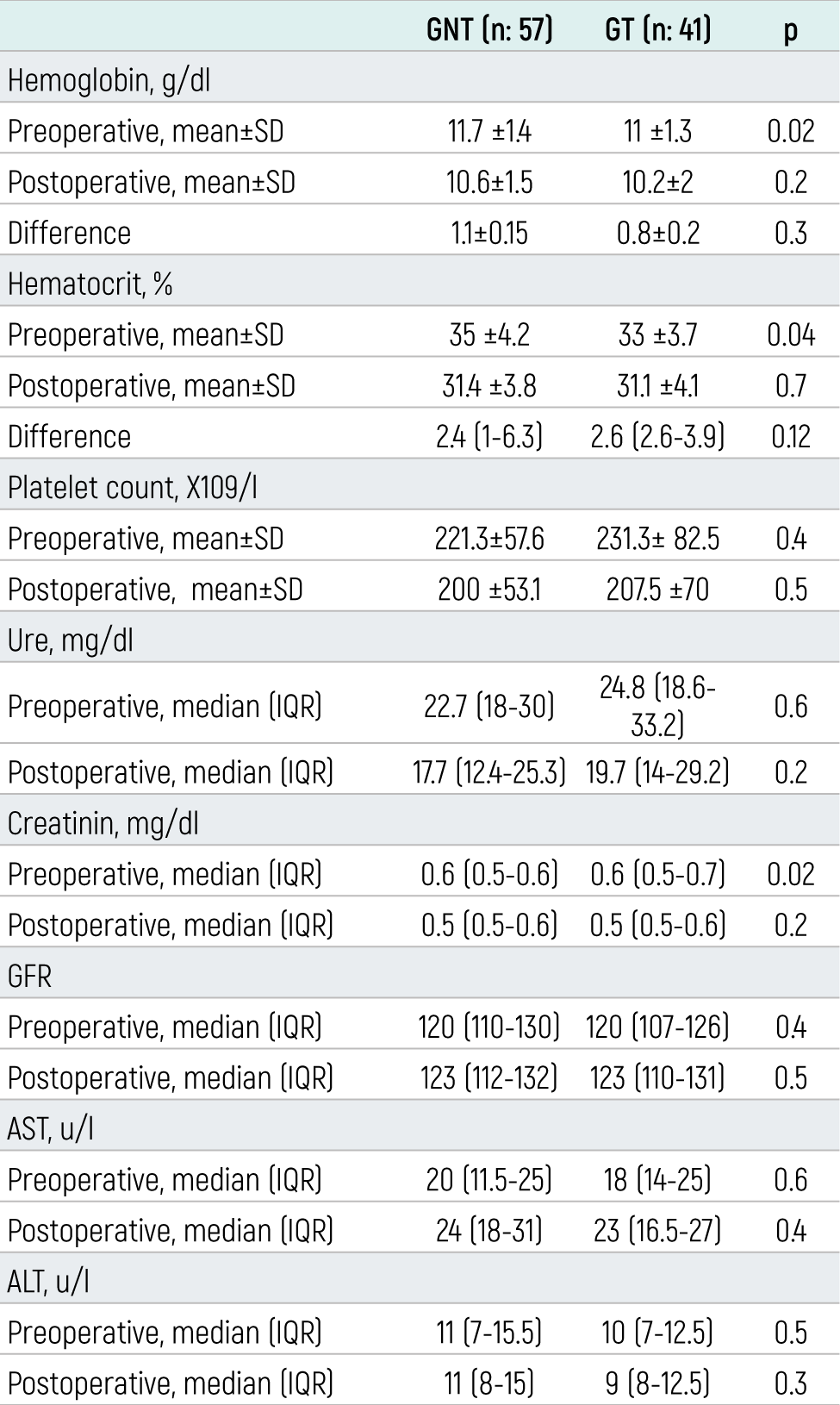
Table 3. Peroperative bleeding, amount of fluid used, blood used and uterotonic needs, APGAR scores and postoperative results
Figures
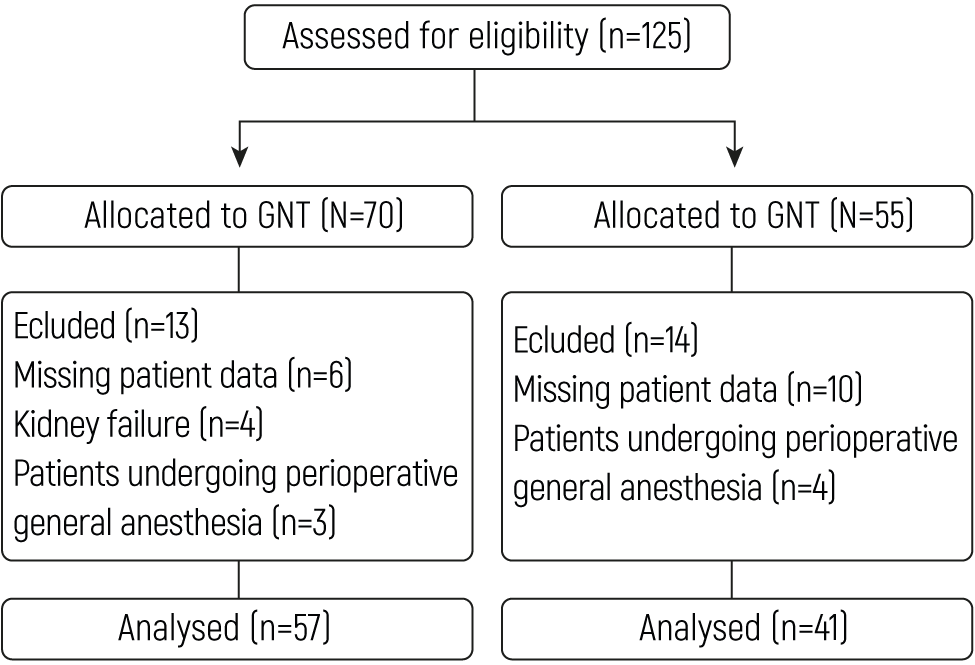
Figure 1. Consort diagram of the study
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Duygu Akyol, Necmiye Ay, İbrahim Polat, Funda Gümüş Özcan. Effect of tranexamic acid used in cesarean sections on perioperative bleeding in preeclamptic patients: a retrospective study. doi:10.4328/ECAM.10067
- Received:
- 17.09.2023
- Accepted:
- 13.10.2023
- Published Online:
- 14.10.2023
- Printed:
- 15.10.2023