Abstract
AimInflammatory Bowel Disease (IBD) is an autoimmune disease characterized by chronic inflammation in the digestive system. Tramadol is an opioid analgesic drug, and it is known to play a role in the inflammation process in IBD disease. While the anti-inflammatory effect of tramadol is known, its role in protecting enterocytes against the cytokine storm is still being investigated. In our study, we aimed to analyze the effect of tramadol on enterocytes before and after cytokine storm in an in vitro inflammation model created with an intestinal epithelial cell line (IEC-6).MethodsThe cytotoxicity of tramadol on the IEC-6 cells was determined by MTT analysis. An in vitro inflammation model was created by treating IEC-6 cells with 50 ng/ml TNF-α+100 ng/ml IFN-ɣ for 48 hours. The IEC-6 cells were divided into four groups as follows: group 1 (control: only culture medium), group 2 (inflammation model: TNF-α and IFN-ɣ combine treatment), group 3 (prophylactic: tramadol treatment before TNF-α and IFN-ɣ combination) and group 4 (treated: tramadol treatment after TNF-α and IFN-ɣ combination). The IL-8 and TNF-α levels in the culture medium were detected by ELISA. The immunoreactivity of caspase-1, caspase-3, IL-6, IL-8, MLKL, RIPK-1 and TNF-α by immunocytochemistry was evaluated.ResultsIncreased RIPK-1 immunoreactivity in IEC-6 cells was indicative of necroptosis in the inflammation model. The pre-treatment of inflammation with tramadol reduced caspase-1 and RIPK-1 immunoreactivities. Additionally, a decrease in IL-8 and TNF-α levels was observedConclusionTramadol, with its anti-inflammatory effect, may be protective for cytokine release and necroptosis in enterocytes.
Keywords
Introduction
Hemostasis of intestinal epithelial cells is maintained through programmed cell death (PCD), which involves substantial removal of damaged cells and the renewal of enterocytes.1 The main forms of PCD are apoptosis, pyroptosis, and necroptosis, yet the mechanisms responsible for PCD in the inflammation process are not yet fully understood.1 Loss of control of innate immune mechanisms due to excessive or defective activation of inflammatory pathways in the gut can lead to dysregulated immune responses that increase susceptibility to infection: Crohn’s disease (CD) and ulcerative colitis (UC) are the two main forms of inflammatory bowel diseases (IBD).1,2 While UC predominantly affects the colon, CD can affect any part of the gastrointestinal tract.2
Tramadol is mainly utilized as an opioid analgesic for the effective management of moderate to moderately severe pain.3 In cases of active IBD, the µ opioid receptor (MOR) is found to be overexpressed in the small intestine and colon.4 This suggests that opioid signaling itself may play a role in the inflammatory process of IBD.4 Studies on mice with chemically-induced colitis demonstrated that treatment with MOR agonists, such as morphine, had an anti-inflammatory effect and could alleviate colitis.4 Wybran et al. published data on the influence of opioids on the immune system, revealing that various opioids can dampen the activation state of T cells.4 However, the described immunomodulatory or immunosuppressive effects on the immune system are unintended and may lead to misinterpretations in experimental inflammation2
Studies have demonstrated that tramadol can inhibit peristalsis in the guinea pig small intestine at micromolar concentrations.5 However, the clinically relevant plasma concentrations of tramadol are lower than those required to abolish peristalsis in the guinea pig small bowel.5 This suggests that tramadol may serve as an alternative to classical opiate therapy.5 Therefore, for patients with IBD, tramadol could be a preferred opioid option.
Cytokine storm is a severe immune reaction in which the body releases excessive amounts of cytokines into the blood too quickly.6 Cytokines play an important role in normal immune responses but excessive cytokine release can be inflammatory cell death pathways such as pyroptosis and necroptosis may trigger.6
We aim to determine the protective effect of tramadol treatment on enterocytes with an in vitro inflammation model that mimics the cytokine storm induced by TNF-α+IFN-ɣ.7,8 Uncovering the correlation between tramadol and IBD may reveal data that tramadol is not only a pain killer, but a suitable drug for possible drug side effects and treatment protocols. Tramadol, which is mostly used as a pain killer, can be used for a different purpose.
Materials and Methods
Cell CultureIntestinal epithelial cell line (IEC-6,CRL-1592,ATCC®) cultured in 10% α-MEM medium (MEMA-RXA,CAPRICORN), containing 90% fetal bovine serum (FBS-11B,CAPRICORN) and 1% penicillin/streptomycin (PS-B,CAPRICORN) in a humidified 5% CO2 atmosphere at 37°C until they were 80% confluent.Determination of the Cytotoxic Dose of Tramadol on EnterocytesThe IEC-6 cells (2x103 cells/per well) were seeded into 96 well culture plates. The following day, tramadol (Contramal ampul, Abdi Ibrahim) was diluted (6 µg/ml, 9 µg/ml, 12 µg/ml and 15 µg/ml) in completed cell culture media and applied to the cells for 24 h and 48 h.9,10 MTT (2,5-diphenyl-2H-tetrazolium bromide, GC4568, Glentham life sciences) was prepared in 5 mg/mL of phosphate buffered saline (PBS) before use and was filtered. After the incubation time, 1:10 dilution of MTT was added to each well for 4 h at 37˚C. The addition of 50 µl dimethyl sulfoxide (DMSO, GK2245, Glentham life sciences) measurements were performed with a microplate reader (ELX800UV,BİOTEK,USA), using 490-540 nm as the reference wavelength.Experimental Groups and Cell StimulationIEC-6 cells were seeded into 8-well plates at a concentration of 1x103 cells/well and cultured for 48 h. TNF-α+IFN-ɣ combination was used for in the vitro inflammation model.7,8 The cells were then divided into groups: Group 1 was the control group and cultured with only culture medium; Group 2 was in vitro inflammation model treated with 50 ng/ml of TNF-α (315-01A-50UG,PeproTech) and 100 ng/ml of IFN-ɣ (315-05-100UG,PeproTech) for 48 h; Group 3 was prophylactic group and 12 µg/ml tramadol was used before TNF-α+IFN-ɣ combine treatment for 24 h; Group 4 was the treatment group and the cells were treated with 12 µg/ml tramadol after TNF-α+IFN-ɣ combine treatment.
Enzyme-linked Immunosorbent Assay (ELISA)
Culture media from all groups were centrifuged at 300xg for 5 min and 40 µl of culture medium was added each well that was coated with TNF-α (201-12-0083,SunRedBio) or IL-8 (SRB-T-83151,SunRedBio). Every sample was replicated three times. Primarily 10 µl biotin-containing TNF-α or IL-8 antibodies and then 50 µl streptavidin-HRP were added to each well and incubated at 37˚C for 60 min. They were washed five times with buffer, chromogen solution A and B were then added and incubated in the dark at 37˚C for 10 min. Finally, the reaction was stopped with a stop solution and the absorbance values were measured at 450 nm. The sample densities were calculated with the standard curve, equation and the corresponding density value of each kit.ImmunocytochemistryBriefly, fixed cells were washed with PBS (PBS404.100, Bioshop). Permeabilization did with 0.1% Triton-X-100 (A4975,0100, Applichem) at 4˚C for 15 min. Endogenous peroxidase activity was quenched by incubation with 3% H2O2 (1.08597.2500, MERCK) for 5 min at room temperature. The cells were incubated with blocking solution (TA-125-UB, THERMOFISHER) for 1 h then primary antibodies [caspase-1 (BT-AP01191,BT-LAB), caspase-3 (BT-AP01199,BT-LAB), IL-6 (SC-1265,SantaCruz), IL-8 (BT-AP04514,BT-LAB), MLKL (BS-5513R,Bioss), RIPK-1 (BS-5805R,Bioss) and TNF-α (BT-AP09103, BT-LAB) were applied for overnight at 4°C. After incubation, the cells incubated with seconder antibodies [biotinylated goat anti rabbit/mouse IgG (TP-125-UB, THERMOFISHER) and peroxidase-conjugated streptavidin (TS-125-UB, THERMOFISHER)] for 30 min each. Diaminobenzidine (DAB,TA-125-HD, THERMOFISHER) was applied to the cells for 5 min. The cells counterstained with Mayer’s hematoxylin (TA-125-MH, THERMOFISHER) for 1 min. Immunolabelling was evaluated semi-quantitatively by two independent observers according to its intensity, as negative (-), mild (+), moderate (++) and strong (+++).Ethical ApprovalThis study did not need ethical approval because of in vitro cell line research.Statistical AnalysisAnalysis graphs were created using the Graphpad Prism (8.0.1.) program. Statistical significance was determined by assessment of differences using one-way analysis of variance (ANOVA) test. All data expressed as mean ± SD with values of p<0.05 were deemed significant.Reporting GuidelinesNo specific reporting guideline was applicable guidelines.
Results
CytotoxicityBased on the MTT results, cell viability remained consistent between the 24 and 48-hour cultures in the control group treated with the standard culture medium. However, when 6 µg/ml and 12 µg/ml of tramadol were administered, there was an observable increase in viability after 48 hours compared to 24 hours. Conversely, with doses of 9 µg/ml and 15 µg/ml, cell viability decreased in the 48-hour culture compared to the 24-hour culture. In our study, we selected the 12 µg/ml dosage and 24-hour application, as it doubled cell viability compared to the control application (Figure 1A).Cell CultureIEC-6 cells were epithelioid structure and adhesive properties during culture. After the combined treatment of TNF-α+IFN-ɣ, cytoplasmic accumulations were present in group 2, while the epithelioid feature was preserved in the cells. Both the morphology of IEC-6 cells in groups 3 and 4 resembled the IEC-6 cells in the control group (Figure 2).Levels of IL-8 and TNF-α in IEC-6 Culture MediumThe ELISA assay successfully detected and quantified IL-8 and TNF-α in the culture medium. The mean OD value of IL-8 for group 1 was 755±0.02, while the mean OD value for groups 2, 3 and 4 were 817.22±0.03, 850.55±0.02 and 760.55±0.03, respectively. The level of IL-8 was similar to group 1, increased level of IL-8 was detected in groups 2 (p=0.3467), 3 (p=0.0266) and 4 (p>0.9999) (Figure 1B). The mean OD value of TNF-α for group 1 was 112.23±0.01, while the mean OD value for groups 2, 3 and 4 were 160.57±0.07, 154.38±0.06 and 81.76±0.006, respectively. Elevated level of TNF-α was measured in groups 2 (p=0.3467), and 3 (p>0.9999), and the level of TNF-α in group 4 (p>0.9999) was less than all other groups (Figure 1C).ImmunocytochemistryCaspase-1 immunoreactivity were observed to be strong (+++) in groups 1, 2 and 4. However, it was moderate (++) and decreased in group 3. The decrease in group 3 compared to group 1 was statistically significant (p=0.04363) (Figure 1D and 2). In addition, caspase-3 was generally weak (+) and similar in all groups (Figure 1E and 2).
IL-6 was negative (-) in both groups 1 and 2. In groups 3 and 4, IL-6 was weak (+) and increased compared to groups 1 and 2, and there was a statistically significant increase (p=0.0436) (Figure 1F and 2). IL-8 was similar and weak (+) in all groups (Figure 1G and 2), and these results were correlated with ELISA assay (Figure 1B).
MLKL was detected in all groups, however, less immunolabelling was observed in group 1 (Figure 1H and 2). RIPK-1 was observed to be similar and weak (+) in group 3 compared to the group 1. Additionally, both the group 2 and 4 showed mild/strong (++/+++) immunoreactivity. The increase in group 2 (p=0.0194) and group 4 (p=0.0060) compared to group 1 was statistically significant. Besides, a statistically significant difference was observed between the groups (groups 3 and 4) administered tramadol (p=0.0194) (Figure 1I and 2). TNF-α immunoreactivity did not differ in all groups (Figure 1J and 2) and intensities were moderate (++).
Discussion
IBD is an autoimmune bowel disease characterized by chronic inflammation.4,11 Opioids are recommended in the analgesic treatment protocols of patients exposed to IBD.11 In a cohort study of IBD patients, lower rates of infection, intestinal obstruction or ileus, and mortality were reported with the use of tramadol.11 Application of TNF-α+IFN-ɣ proinflammatory cytokines to the IEC-6 cell line triggers inflammation.7,8 In our study, the in vitro inflammation model IEC-6 cells created with TNF-α+IFN-ɣ maintained their epithelioid properties but had cytoplasmic deposits.
Cytokine storm is regulated by numerous cytokines and inflammatory mediators.6 It occurs when the imbalance between pro-inflammatory and anti-inflammatory factors becomes apparent.6 Proinflammatory cytokines synthesis, such as IL-6 and TNF-α alters epithelial homeostasis after infection.12 The potency state for inhibition of cytokine release is considerably higher in tramadol than in other opioids.12 In our study, the prophylactic and therapeutic effects of tramadol were evaluated in the inflammation model created in enterocytes by cytokines.
Cytokine storms can also trigger inflammatory cell death pathways like necroptosis. Caspase-1 is an enzyme that plays a crucial role in various cellular processes, including apoptosis and inflammation and its excessive secretion triggers inflammation and inflammation-mediated diseases.13,14 Our results suggested that the administration of tramadol after inflammation may have reduced cell death in in vitro condition by controlling the release of caspase-1 in enterocytes. The decrease in group 3 suggested a protective effect of tramadol on the intestines supporting our hypothesis concerning the impact of tramadol in our study.
A multifaceted role of IL-6 has been reported in IBD.15 IL-6’s function can shift based on the composition of the gut microbiota. When microbiome balance is disrupted, IL-6 increases. Conversely, in the presence of a healthy intestinal flora IL-6 appears to aid in maintaining intestinal equilibrium and mitigating pathological inflammation.15
In summary, IL-6 can serve as both an initiator of inflammation and a promoter of intestinal harmony and stability. Consequently, when pro-inflammatory factors like TNF-α+IF-ɣ are applied, IL-6 levels may decrease due to disruptions in the IEC-6 cell lines. However, the administration of tramadol to restore homeostasis in these cell lines can lead to a rise in IL-6 levels. Therefore, according to our study, IL-6 immunoreactivity remained consistent and similar between group 1 and 2, with changes occurring after tramadol administration, suggesting that IEC-6 cells responded to tramadol.
Additionally, it is worth noting that IL-8 is a pro-inflammatory cytokine.16 Since the pro-inflammatory function of IL-8 is neutrophil and macrophage dependent, it is likely that the IL-8 levels remained unchanged in our in vitro study.
In addition, the level of TNF-α is also a key regulator of inflammation control.17,18 In our study, TNF-α level was evaluated both immunocytochemically and by ELISA. While TNF-α immunoreactivities in IEC-6 cells were similar in all groups, group 2 had a higher TNF-α level compared to group 1. However, the level of TNF-α in the culture medium was decreased after tramadol treatment in group 4 compared to group 2, which was statistically significant, suggesting a protective effect on IEC-6 cells post-cytokine storm. Throughout this process, the analysis of the culture medium proved to be more insightful than cell immunoreactivity since TNF-α is a cytokine released in the early stages of inflammation. Therefore, tramadol may control the secretion of TNF-α from enterocytes to trigger the inflammatory process in microenvironment of enterocytes. In our study, IL-8 and TNF-α immunoreactivities in IEC-6 cells were similar in all groups, however, the level of IL-8 and TNF-α in culture medium was decreased after tramadol treatment. Therefore, tramadol may control the secretion of IL-8 and TNF-α from enterocytes, triggering the inflammatory process in microenvironment of enterocytes.
During necroptosis, phosphorylation of MLKL occurs downstream of activation of RIPK-1 and RIPK-3.12 It has been demonstrated that the deterioration and subsequent cell death in IEC-6 cells resulting from the application of TNFα+IFN-ɣ are not attributable to RIPK-1/3 or caspases.19 In our inflammation model, even though we observed a non-significant decrease in caspase-3 levels within the prophylactic group, the protective effect of tramadol application has been supported. In addition, the decrease in the distribution of RIPK-1 that induces apoptosis and necroptosis in group 3 (p<0.01), indicates that cell death can be controlled through induction of necroptosis.
After inflammatory model that occurred with TNF-α+IFN-ɣ administration, mimicked the inflammatory microenvironment in enterocytes. It induced necroptosis rather than apoptosis with an increase in MLKL and RIPK-1. Application of tramadol decreased the RIPK-1 and caspase 1 in group 3. Therefore, the anti-inflammatory effects of tramadol can be protective for enterocytes after inflammation in intestinal diseases like IBD. The in vivo effect of tramadol should be investigated in IBD animal model to evaluate its role.
Conclusion
In conclusion, our findings provide valuable insights into the potential therapeutic benefits of tramadol in mitigating inflammation and cell death in enterocytes. The absence of other immune system cells in the in vitro environment may have influenced the cellular response compared to the in vivo setting. Therefore, the initial results obtained in our study involving tramadol-triggered intestinal epithelial cells are significant preliminary data for in vivo studies.
Declarations
Informed Consent
Not applicable.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare no conflict of interest.
Funding
None.
Abbreviations
CD: Crohn’s disease
DMSO: Dimethyl sulfoxide
ELISA: Enzyme-linked immunosorbent assay
FBS: Fetal bovine serum
IBD: Inflammatory bowel disease
IEC: Intestinal epithelial cell
IFN-γ: Interferon gamma
IL: Interleukin
MLKL: Mixed lineage kinase domain-like protein
MOR: Mu opioid receptor
MTT: 2,5-Diphenyl-2H-tetrazolium bromide
PBS: Phosphate-buffered saline
PCD: Programmed cell death
RIPK: Receptor-interacting protein kinase
TNF-α: Tumor necrosis factor alpha
UC: Ulcerative colitis
References
- Ruera CN, Miculán E, Pérez F, Ducca G, Carasi P, Chirdo FG. Sterile inflammation drives multiple programmed cell death pathways in the gut. J Leukoc Biol. 2021;109(1):211-221. doi:10.1002/jlb.3ma0820-660r
- Golusda L, Kühl AA, Siegmund B, Paclik D. Reducing pain in experimental models of intestinal inflammation affects the immune response. Inflamm Bowel Dis. 2022;28(5):801-807. doi:10.1093/ibd/izab290
- Buccellati C, Sala A, Ballerio R, Bianchi M. Tramadol anti-inflammatory activity is not related to a direct inhibitory action on prostaglandin endoperoxide synthases. Eur J Pain. 2000;4(4):413-415. doi:10.1053/eujp.2000.0208
- Wybran J, Appelboom T, Famaey JP, Govaerts A. Suggestive evidence for receptors for morphine and methionine-enkephalin on normal human blood T lymphocytes. J Immunol. 1979;123(3):1068-1070. doi:10.4049/jimmunol.123.3.1068
- Herbert MK, Weis R, Holzer P. The enantiomers of tramadol and its major metabolite inhibit peristalsis in the guinea pig small intestine via differential mechanisms. BMC Pharmacol. 2007;7:5. doi:10.1186/1471-2210-7-5
- Cron RQ, Goyal G, Chatham WW. Cytokine storm syndrome. Annu Rev Med. 2023;74(1):321-337. doi:10.1146/annurev-med-042921-112837
- Karki R, Sharma BR, Tuladhar S, et al. Synergism of TNF-α and IFN-γ triggers inflammatory cell death, tissue damage, and mortality in SARS-CoV-2 infection and cytokine shock syndromes. Cell. 2021;184(1):149-168.e17. doi:10.1016/j.cell.2020.11.025
- Kolinska J, Lisa V, Clark JA, et al. Constitutive expression of IL-18 and IL-18R in differentiated IEC-6 cells: effect of TNF-α and IFN-γ treatment. J Interferon Cytokine Res. 2008;28(5):287-296. doi:10.1089/jir.2006.0130
- Keskinbora K, Aydınlı I. An atypical opioid analgesic: tramadol. Agri. 2006;18(1):5-19.
- Scott LJ, Perry CM. Tramadol: a review of its use in perioperative pain. Drugs. 2000;60(1):139-176. doi:10.2165/00003495-200060010-00008
- Dalal RS, Lund K, Zegers FD, Friedman S, Allegretti JR, Nørgård BM. Use of tramadol vs traditional opioids and adverse outcomes in patients with inflammatory bowel disease: a Danish nationwide cohort study. Inflamm Bowel Dis. 2023.
- Subedi M, Bajaj S, Kumar MS, Yc M. An overview of tramadol and its usage in pain management and future perspective. Biomed Pharmacother. 2019;111:443-451. doi:10.1016/j.biopha.2018.12.085
- McIlwain DR, Berger T, Mak TW. Caspase functions in cell death and disease. Cold Spring Harb Perspect Biol. 2013;5(4).
- Molla MD, Akalu Y, Geto Z, Dagnew B, Ayelign B, Shibabaw T. Role of caspase-1 in the pathogenesis of inflammatory-associated chronic noncommunicable diseases. J Inflamm Res. 2020;13:749-764. doi:10.2147/jir.s277457
- Shahini A, Shahini A. Role of interleukin-6-mediated inflammation in the pathogenesis of inflammatory bowel disease: focus on the available therapeutic approaches and gut microbiome. J Cell Commun Signal. 2023;17(1):55-74. doi:10.1007/s12079-022-00695-x
- Anton K, Glod J. Tumor-secreted factors that induce mesenchymal stromal cell chemotaxis. In: Mesenchymal Stromal Cells as Tumor Stromal Modulators. 2016:193-214.
- Pan L, Xie W, Fu X, et al. Inflammation and sarcopenia: a focus on circulating inflammatory cytokines. Exp Gerontol. 2021;154:111544. doi:10.1016/j.exger.2021.111544
- van Loo G, Bertrand MJM. Death by TNF: a road to inflammation. Nat Rev Immunol. 2023;23(5):289-303. doi:10.1038/s41577-022-00792-3
- Woznicki JA, Saini N, Flood P, et al. TNF-α synergises with IFN-γ to induce caspase-8-JAK1/2-STAT1-dependent death of intestinal epithelial cells. Cell Death Dis. 2021;12(10):864. doi:10.1038/s41419-021-04151-3
Figures
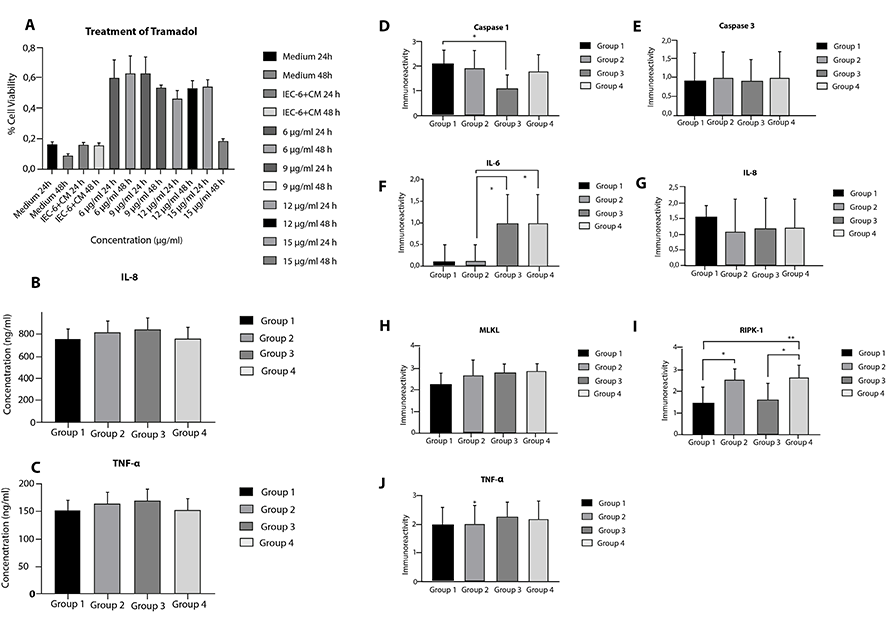
Figure 1. (A) Percent viability changes of IEC-6 cells after 24 h and 48 h of tramadol treatment. ELISA results of IL-8 (B) and TNF-α (C) levels in culture mediums of all groups. Caspase-1 (D), caspase-3 (E), IL-6 (F), IL-8 (G), MLKL (H), RIPK-1 (I) and TNF-α (J) immunoreactivity measurements and statistical analysis in all experimental groups. The results were presented as mean ± SD and the significance of the difference was indicated with asterisk (*) as p-value smaller than 0.05 (p
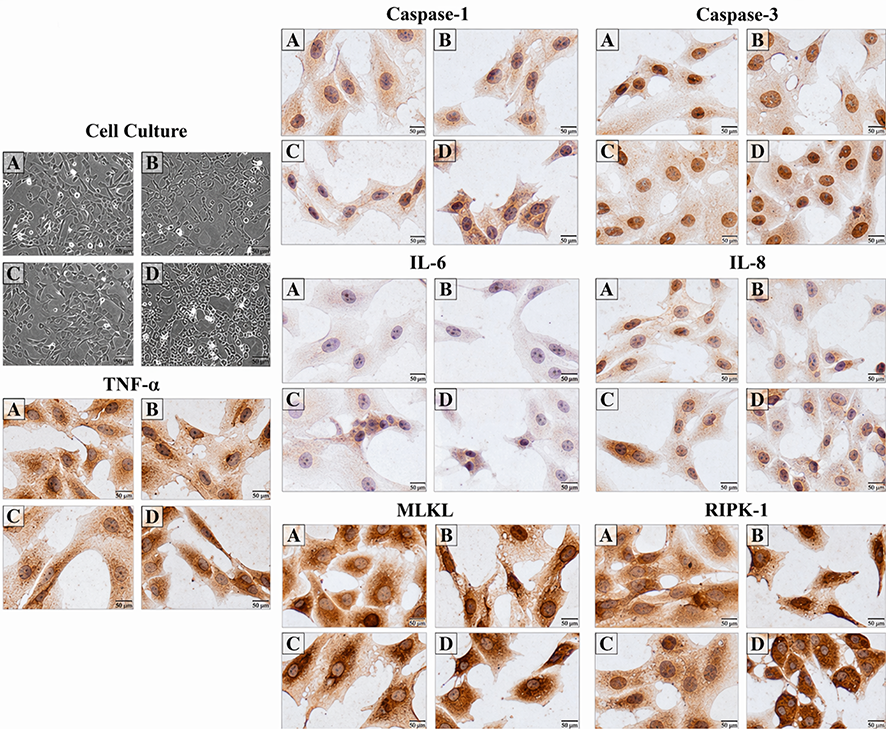
Figure 2. Cell culture of group 1 (A), group 2 (B), group 3 (C) group 4 (D) IEC-6 cells and caspase-1, caspase-3, IL-6, IL-8, MLKL, RIPK-1, TNF-α immunocytochemical staining images. Scale Bars: 100 µm (cell culture) and 10 µm (immunocytochemistry).
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Ugur Ozgurbuz, Damla Akogullari Celik, Hilal Kabadayi Ensarioglu, Hafize Seda Vatansever. Tramadol protects enterocytes after cytokine storm. doi:10.4328/ECAM.10070
- Received:
- 26.09.2023
- Accepted:
- 13.10.2023
- Published Online:
- 14.10.2023
- Printed:
- 15.10.2023