Abstract
AimThis study aimed to investigate the impact of bariatric surgery (BS) on individuals with hypertension (HT) by assessing changes in clinical and metabolic parameters following BS.MethodsA total of 34 obese individuals undergoing BS were included in the study. Demographic characteristics, including age and gender, were recorded, along with clinical parameters such as body mass index (BMI), glucose levels, blood urea nitrogen (BUN), uric acid, C-reactive protein (CRP), albumin, CRP-to-albumin ratio (CAR), and glycated hemoglobin (HbA1c). Hypertensive patients were further divided into groups based on the use of HT medication. Changes in these parameters were assessed three months post-surgery and compared between groups.ResultsNo significant differences were observed in age, gender, and most metabolic parameters between groups with and without HT (p>0.05). Although, preoperative BMI was higher in the HT group (p=0.014), the difference was decreased following BS (p=0.059). 29.2% of HT patients stopped or reduced doses of antihypertensive medicines. There were no significant differences in glucose, BUN, CRP, CAR, and HbA1c levels between groups. Notably, uric acid levels exhibited a greater reduction in the HT group (mean change of -0.3 vs. -0.1, p=0.026). AKI rates were higher among HT patients with obesity (20% vs 12.5%, p=0.975) but the difference was not significant.ConclusionThis study has once again demonstrated that a reduction in blood pressure can be achieved in obese patients with HT following BS. Additionally, it is noteworthy that additional benefits, such as improvements in high uric acid levels in HT patients, can also be observed. These findings reflect the beneficial metabolic consequences of BS.
Keywords
Introduction
A body mass index (BMI) of ≥30 kg/m2 denotes obesity, a chronic condition on the rise globally.1,2 The World Health Organization estimates around 650 million adults worldwide suffer from obesity (availiable at: https://www.who.int/en/news-room/fact-sheets/detail/obesity-and-overweight), with approximately 35% of U.S. adults (about 100 million people) affected.3 Procedures addressing obesity are collectively known as metabolic or “bariatric” surgery (from the Greek “baros,” meaning “weight,” and “iatrikos,” meaning “medicine”). Obesity has long been associated with increased morbidity and mortality, particularly reducing life expectancy for those under 40 years old.4
Higher BMI generally correlates with elevated all-cause and cardiovascular mortality risk, with a 21-108% increased risk in all-cause mortality among those with BMI ≥30 according to a National Health Interview Survey analysis.5 The risk escalates with higher BMI and is more pronounced in severe obesity. Bariatric surgery (BS), or metabolic surgery, is increasingly employed worldwide, particularly for advanced obesity. It ‘is preferred for patients who meet these criteria: 1) BMI ≥ 40 kg/m2, 2) BMI ≥ 35 with obesity-related comorbidities (e.g., type 2 diabetes, hypertension), and 3) unsuccessful weight loss despite medical efforts.6
Obese individuals frequently exhibit elevated blood pressure, especially with upper body and abdominal obesity. Weight loss in obesity is linked to lower blood pressure. Bariatric surgery not only improves metabolism, including diabetes and fatty liver disease, but also reduces blood pressure.7,8 This study aims to reveal the differences between outcomes of hypertensive and nonhypertensive individuals following sleeve gastrectomy.
Materials and Methods
In this retrospective two-center case- control study, 34 individuals with obesity who underwent sleeve gastrectomy between January 27 and February 28, 2022, were evaluated. The operations were conducted at Medicana International Ankara hospital by experienced bariatric surgery teams who currently operates monthly approximately 20-25 cases.
Inclusion criteria: Individuals with bariatrric surgery indications and who could be completely monitored in regardfor of clinical and laboratory features following sleeve gastrectomy were enrolled in the study.
Exclusion criteria: Prolonged hospitalization, post-surgery infection, and patients with missing data.
BS indications: The indications were followed according to the criteria of the American Society for Metabolic and Bariatric Surgery 2018.6
Drug cessation and categorizing: Individuals who were under an antihypertensive regimen longer than 3 months were labelled as hypertensive “HT + Group” and who had no history of HT were labelled as “HT – Group”. Then, after BS surgery, a group of patients who did not require antihypertensive following 3 months were labelled as “hypertensive medication -“ and the patients who remained on anti-hypertensive medication were labelled as “hypertensive medication +” groups. Furthermore, patients who required a lower dose of antihypertensive medication postoperatively compared to their preoperative dose were categorized into the ‘HT -’ and ‘hypertensive medication -’ groups.
Measurements: The demographic variables (age, gender, BMI) and laboratory features (glucose, creatinine, uric acid, C-reactive protein [CRP], albumin, CRP-to-albumin ratio [CAR], glycated hemoglobin A1c [HbA1c]) of patients were recorded preoperatively and at 3 months after post-bariatric surgery (BS).Ethical ApprovalThe study was approved by the Ethics Committee of Medipol University Faculty of Medicine (Decision No: E-10840098-772.02-6203).Statistical AnalysisResearch data were analyzsed using IBM SPSS 22 (IBM Statistical Package for Social Sciences). Descriptive statistics of categorical variables are presented as numbers and percentages. The normality distribution of numerical variables was assessed with the Shapiro-Wilk test because the number of cases per group was less than 30. Cross-tabulations were used to compare categorical variables, and the Pearson chi-square test, Yates continuity correction, and Fisher exact test were applied. Numeric variables, which were normally distributed (parametric) were presented as mean ± standardt deviation, and numeric variables, which were not normally distributed (nonparametric) were variables are presented as median (minimum-maximum). The independent -samples t- test was used in the comparison for parametric variables, whereas the Mann-Whitney U test was used in the comparison of non- parametric variables. The accepted statistical significance level was p<0.05.Reporting GuidelinesThe study was reported in accordance with STROBE guidelines.
Results
The study included a total of 34 obese individuals. 70.5% of obese patients in this study had HT. Table 1 presents the demographic and laboratory characteristics of the groups based on the presence of hypertension (HT) among the participants. Regarding age and gender, no differences were observed between the groups with and without HT. While there were no disparities between the groups concerning the patients’ preoperative BMI, a significant difference in mean BMI was detected after three months, with the HT group showing a higher mean BMI (31.6 kg/m² vs. 44.7 kg/m², p = 0.014).
During the preoperative assessment, no statistically significant differences were found between the groups in terms of glucose, BUN, uric acid, CRP, albumin, CAR, and HbA1c levels. Similarly, at the three-month follow-up after surgery, no statistically significant differences were identified between the groups in relation to glucose, BUN, uric acid, CRP, albumin, CAR, and HbA1c levels. Additionally, no statistically significant differences were observed between the groups in terms of the development of acute kidney injury (AKI).
BMI, Body mass index BUN, Bloodd urea nitrogen, CRP, C-reactive protein CAR, CRP to albumin ratio.
According to the presence of hypertension, differences in patients’ BMI, glucose, BUN, uric acid, CRP, albumin, CAR, and HbA1c values were assessed at the three-month mark post-bariatric surgery in comparison to their respective preoperative values (see Table 2). No statistically significant differences were observed between the groups in terms of BMI, glucose, BUN, uric acid, CRP, albumin, and CAR. However, there was a higher change in HbA1c levels in the HT group when compared to the group without HT (median change of -0.3 vs. -0.1, p=0.038).
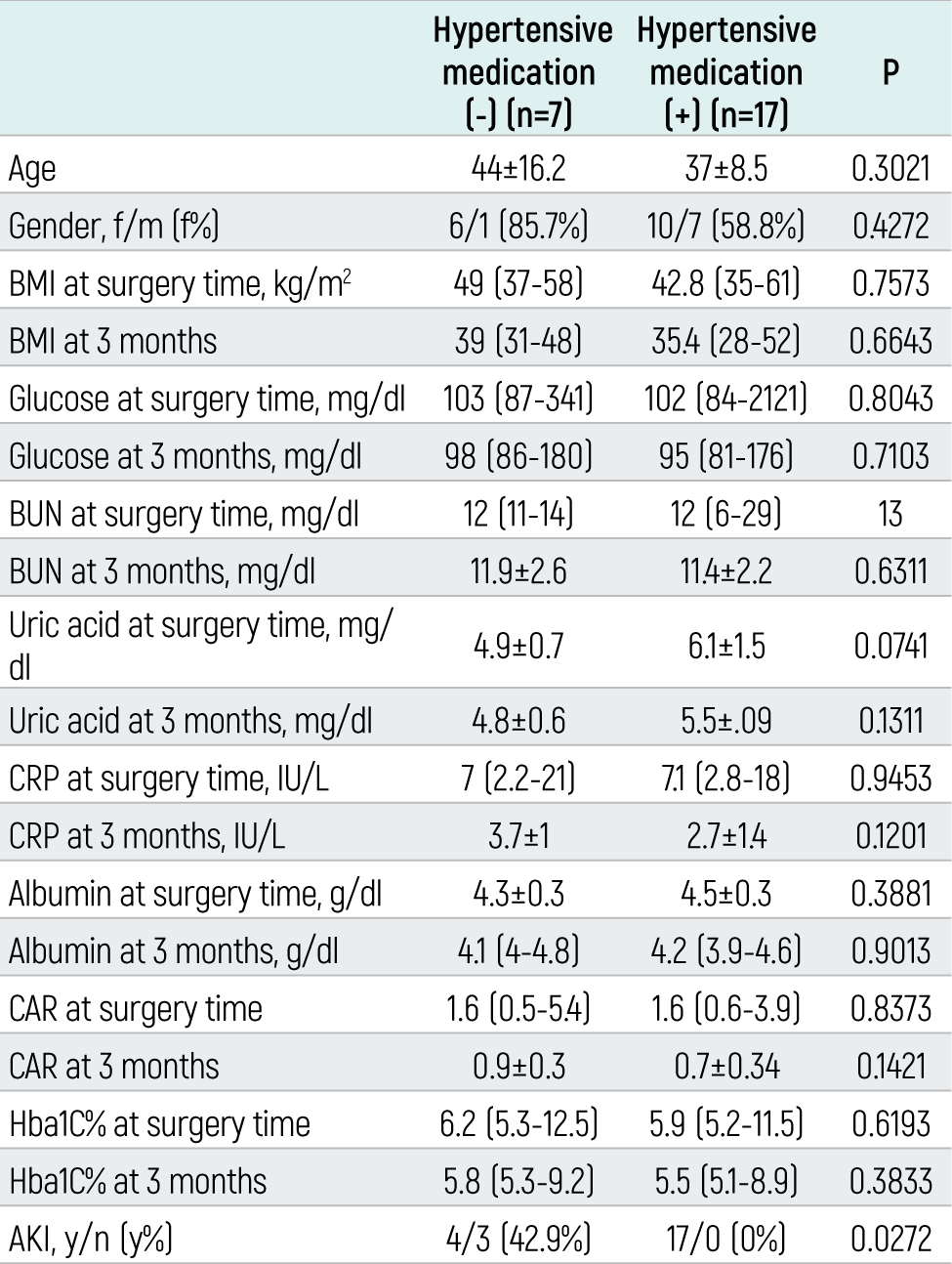
A subset of patients with hypertension (n=7, 29.2%) no longer required hypertension medication following bariatric surgery. In Table 3, we present the characteristics of patients who ceased hypertension medication and those who continued their treatment. Notably, no statistically significant differences were observed between the groups concerning age, gender, preoperative and postoperative BMI, glucose, BUN, uric acid, CRP, albumin, CAR, and HbA1C. Four patients who developed acute kidney injury (AKI) belonged to the group that discontinued hypertension treatment (p=0.027). This is probably due to postoperative hypotension episodes which did were mandatory to stop the medication.
In the context of the HT medication (-)/(+) groups, variations in patients’ BMI, glucose, BUN, uric acid, CRP, albumin, CAR, and HbA1c values were assessed at the three-month mark post-bariatric surgery in comparison to their respective preoperative values, and the groups were subjected to comparative analysis. No statistically significant differences were observed between the groups concerning BMI, glucose, BUN, CRP, CAR, and HbA1c (respectively, p=0.173, p=0.852, p=0.534, p=0.407, p=0.266, p=0.447, p=0.534). However, a significant discrepancy emerged in the reduction of uric acid levels between the group receiving hypertension treatment after bariatric surgery and the group not receiving any medication (mean change of -0.3 vs. -0.1, p=0.026).
Discussion
The present study investigated the impact of bariatric surgery on individuals with hypertension. The findings revealed significant changes in various clinical parameters post-surgery. Notably, a subgroup of patients with HT demonstrated a notable decrease in the need for HT medication following bariatric intervention, underscoring the potential therapeutic benefits of surgical intervention in managing HT.
Hypertension and obesity are the main risk factors for mortality and cardiovascular diseases.9,10 The relationship between excess adiposity and elevated blood pressure is well-established, with obesity estimated to account for 65-78% of cases of primary hypertension.11 Consistent with previous studies, this research found a hypertension prevalence rate as high as 70.5% among obese patients. Furthermore, this study focused on a relatively young population with a higher prevalence of hypertension. However, it is evident that this population represents a group of patients with at least Class II obesity or Class I obesity accompanied by comorbidities.
Bariatric surgery is the preferred treatment option for obesity in a group of patients whose criteria are outlined in the guidelines.6 Additionally, since many metabolic parameters reverse following bariatric surgery, a reduction in blood pressure can also occur.12,13 Patients diagnosed with hypertension before undergoing bariatric surgery had higher BMI values. However, after sleeve gastrectomy, the BMI values of patients with and without a diagnosis of hypertension were found to be similar. Remarkably, 29.2% of patients diagnosed with hypertension before the surgery achieved normotension within the first three months postoperatively, leading to the discontinuation of their antihypertensive medications. Indeed, a group of patients, likely because they did not discontinue antihypertensive medications in the preoperative period, experienced acute kidney injury related to hypotension. As a result, antihypertensive medications had to be discontinued early in these patients. Uric acid levels exhibited a more pronounced decrease in the HT group following BS. The reduction in uric acid levels in the HT group may signify a favorable metabolic response to BS, which could have implications for the management of both hypertension and hyperuricemia in obese individuals. The findings of from this study align with the research conducted by Liu et al., which reported the effectiveness of bariatric surgery in reducing serum uric acid levels in obese patients with type 2 diabetes mellitus.14 Analysis of metabolic and inflammatory markers provided valuable insights into the physiological shifts accompanying BS. Notably, no statistically significant variances were detected in glucose, blood urea nitrogen, C-reactive protein, albumin, CAR, and HbA1c levels between HT groups. This suggests that, within the scope of this study, HT did not exert a discernible influence on these parametres post-BS.
Limitations
Limitations of the Study
1. Short-Term Follow-Up: The study’s follow-up period was limited to three months post-bariatric surgery. Longer-term follow-up would provide a more comprehensive understanding of the sustained effects of surgery on hypertension and other metabolic parameters.
2. Selection Bias: The study may be susceptible to selection bias, as the sample consisted of individuals who had already opted for BS. This may not represent the entire population of individuals with obesity and hypertension, potentially skewing the results.
3. Lack of Control Group: The absence of a control group, comprising obese individuals who did not undergo bariatric surgery, makes it challenging to attribute observed changes solely to the surgical intervention.
4. Data on Medication Use: While the study mentions the discontinuation of hypertension medication in some patients, detailed information on medication types, dosages, and adherence would provide a more nuanced understanding of the impact of surgery on medication management.
5. Heterogeneity: The study does not address potential variations in surgical techniques or the presence of other comorbidities among the participants, which could influence outcomes.
6. Data on Dietary and Lifestyle Changes: Information regarding dietary and lifestyle modifications following surgery, which can significantly affect metabolic parameters, was not included in the analysis.
7. Single-Center Study: The study’s single-center nature of the study may limit the generalizability of the findings to other healthcare settings with different patient demographics and practices.
8. Data Collection Methods: The study relies on retrospective data, which may introduce recall bias and limit the accuracy of certain clinical measurements.
9. Duration of Hypertension: The duration of hypertension and its management prior to surgery were not explicitly considered in the analysis, which could impact the observed changes in HT status post-surgery.
10. Statistical Power: Given the small sample size, the study may have limited statistical power to detect subtle differences in some parameters, potentially leading to type II errors.ot exert a discernible influence on these parameters post-BS.
11. Sample Size: The study included a relatively small sample size of 34 obese individuals, which may limit the generalizability of the findings to broader populations.
Conclusion
This study provides valuable insights into the effects of bariatric surgery on individuals with hypertension. While no significant differences were observed in several clinical parameters, a notable reduction in uric acid levels was noted in patients receiving HT medication post-surgery. Additionally, close monitoring of renal function is crucial, especially in individuals receiving HT treatment. Further research, encompassing larger sample sizes and longer follow-up periods, is warranted to corroborate these findings and illuminate the intricate interplay between HT, bariatric surgery, and associated metabolic changes. These insights hold the potential for refining therapeutic approaches and optimizing outcomes for individuals with both obesity and hypertension.
Declarations
Informed Consent
Not required.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare no conflict of interest.
Funding
None.
Abbreviations
BMI: Body mass index
BS: Bariatric surgery
BUN: Blood urea nitrogen
CAR: C-reactive protein-to-albumin ratio
CRP: C-reactive protein
HbA1c: Glycated hemoglobin A1c
HT: Hypertension
IRB: Institutional review board
References
- Semlitsch T, Stigler FL, Jeitler K, Horvath K, Siebenhofer A. Management of overweight and obesity in primary care: a systematic overview of international evidence-based guidelines. Obes Rev. 2019;20(9):1218-1230. doi:10.1111/obr.12889
- Kushner RF, Ryan DH. Assessment and lifestyle management of patients with obesity: clinical recommendations from systematic reviews. JAMA. 2014;312(9):943-952. doi:10.1001/jama.2014.10432
- Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of childhood and adult obesity in the United States, 2011-2012. JAMA. 2014;311(8):806-814. doi:10.1001/jama.2014.732
- Grover SA, Kaouache M, Rempel P, et al. Years of life lost and healthy life-years lost from diabetes and cardiovascular disease in overweight and obese people: a modelling study. Lancet Diabetes Endocrinol. 2015;3(2):114. doi:10.1016/s2213-8587(14)70229-3
- Visaria A, Setoguchi S. Body mass index and all-cause mortality in a 21st century US population: a National Health Interview Survey analysis. PLoS One. 2023;18(7). doi:10.1371/journal.pone.0287218
- English WJ, DeMaria EJ, Hutter MM, et al. American Society for Metabolic and Bariatric Surgery 2018 estimate of metabolic and bariatric procedures performed in the United States. Surg Obes Relat Dis. 2020;16(4):457-463. doi:10.1016/j.soard.2019.12.022
- Schlottmann F, Galvarini MM, Dreifuss NH, Laxague F, Buxhoeveden R, Gorodner V. Metabolic effects of bariatric surgery. J Laparoendosc Adv Surg Tech A. 2018;28(8):944-948. doi:10.1089/lap.2018.0394
- Dixon JB. Surgical management of obesity in patients with morbid obesity and nonalcoholic fatty liver disease. Clin Liver Dis. 2014;18(1):129-146. doi:10.1016/j.cld.2013.09.011
- Redon J, Tellez-Plaza M, Orozco-Beltran D, et al. Impact of hypertension on mortality and cardiovascular disease burden in patients with cardiovascular risk factors from a general practice setting: the ESCARVAL-risk study. J Hypertens. 2016;34(6):1075-1083. doi:10.1097/hjh.0000000000000930
- Abdelaal M, le Roux CW, Docherty NG. Morbidity and mortality associated with obesity. Ann Transl Med. 2017;5(7):161. doi:10.21037/atm.2017.03.107
- Shariq OA, McKenzie TJ. Obesity-related hypertension: a review of pathophysiology, management, and the role of metabolic surgery. Gland Surg. 2020;9(1):80-93. doi:10.21037/gs.2019.12.03
- Iqbal Z, Adam S, Ho JH, et al. Metabolic and cardiovascular outcomes of bariatric surgery. Curr Opin Lipidol. 2020;31(4):246-256. doi:10.1097/mol.0000000000000696
- Boido A, Ceriani V, Cetta F, Lombardi F, Pontiroli AE. Bariatric surgery and prevention of cardiovascular events and mortality in morbid obesity: mechanisms of action and choice of surgery. Nutr Metab Cardiovasc Dis. 2015;25(5):437-443. doi:10.1016/j.numecd.2015.01.011
- Liu W, Zhang H, Han X, Zhang P, Mao Z. Uric acid level changes after bariatric surgery in obese subjects with type 2 diabetes mellitus. Ann Transl Med. 2019;7(14):332. doi:10.21037/atm.2019.06.66
Tables
Table 1. Comparison of demographic and clinical-laboratory results betweenamong groups based on hypertension the presence of hypertension.
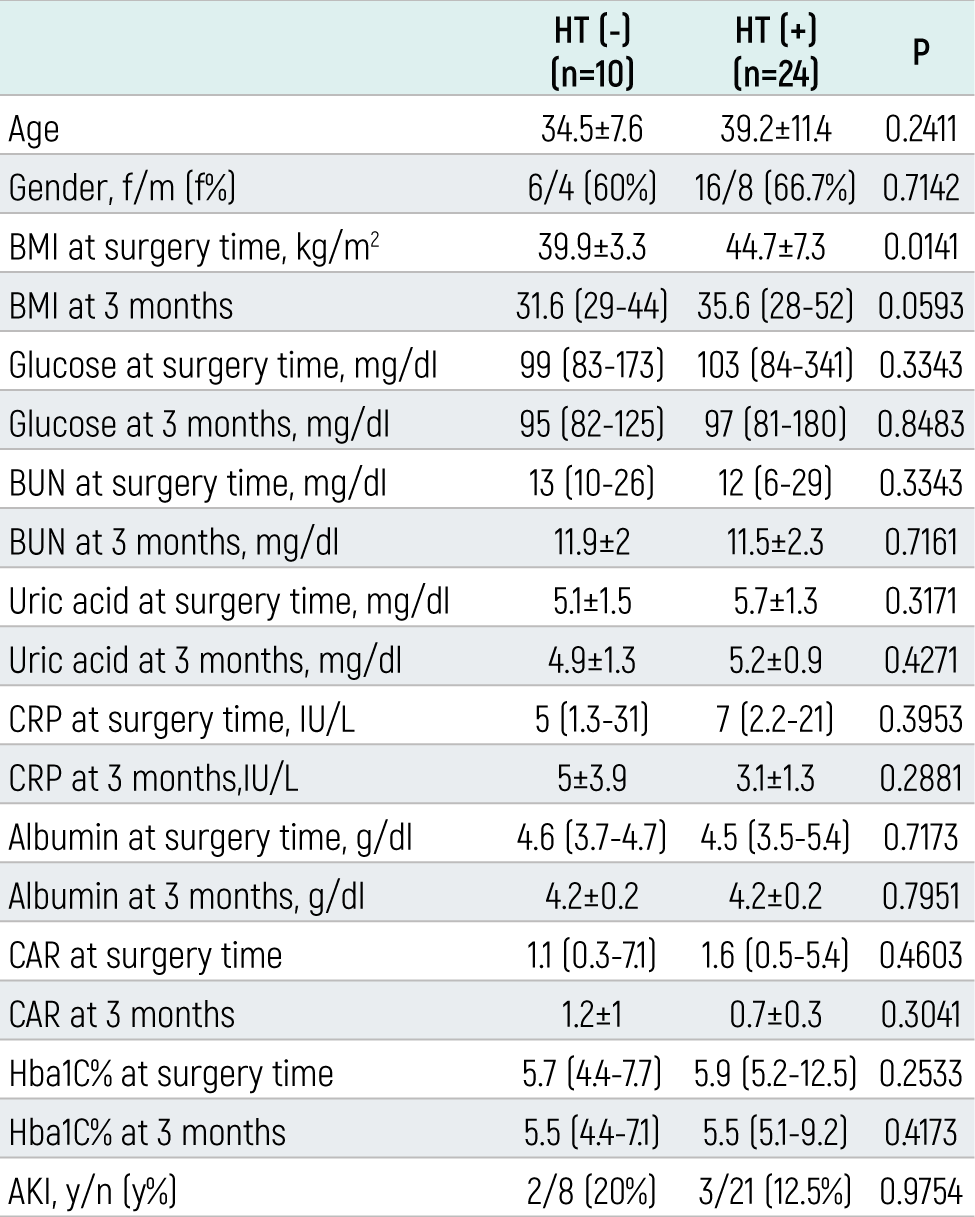
Table 2. Differences in of patient’s clinical and laboaraotary characteristics between preoperative and postoperative -3 -months.
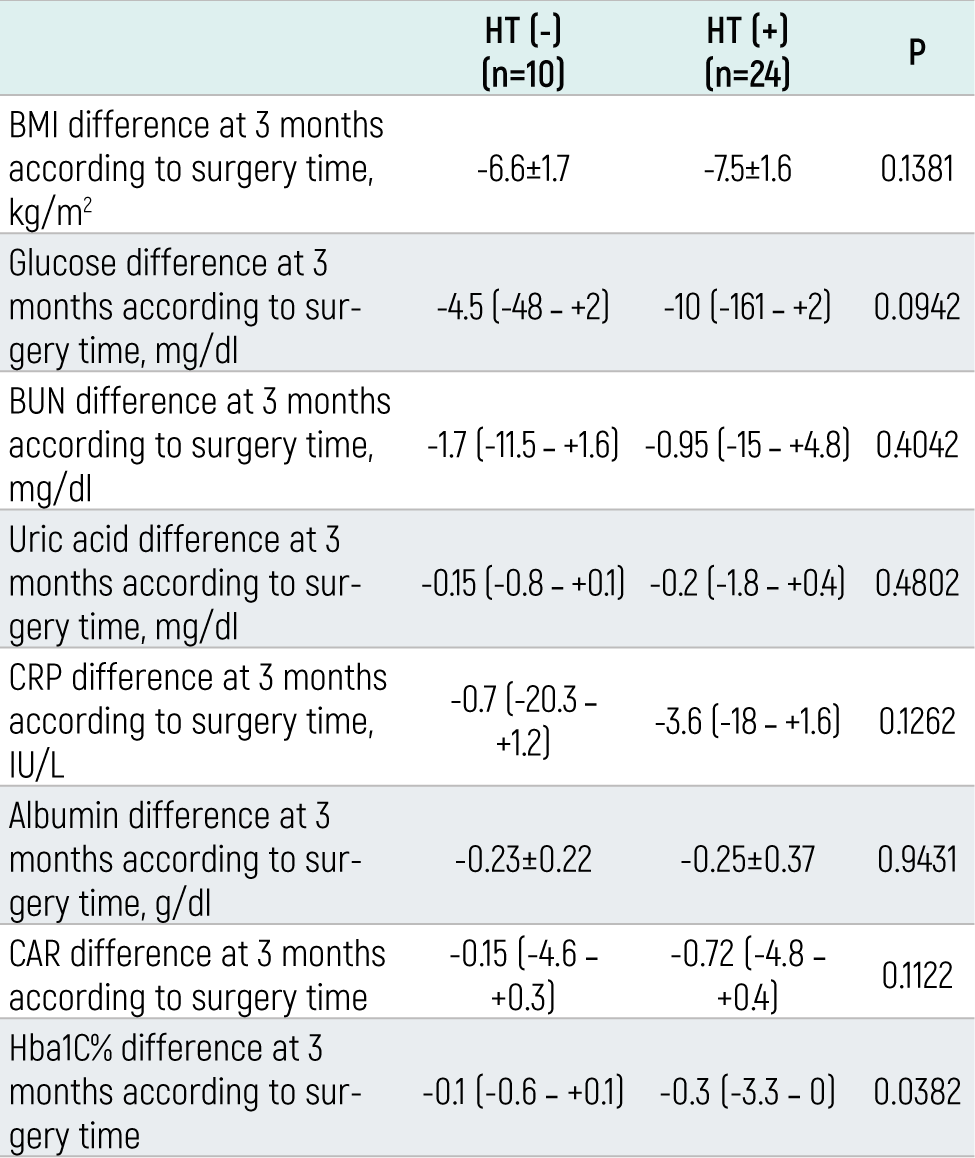
Table 3. Demographic characteristics and the characteristics of the patients who did not require hypertension medication and whose continued hypertension treatment.
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Tuba Mert, Gülçin Türkmen Sarıyıldız. Clinical outcomes in hypertensive patients undergoing bariartic surgery. doi:10.4328/ECAM.10071
- Received:
- 28.09.2023
- Accepted:
- 13.10.2023
- Published Online:
- 14.10.2023
- Printed:
- 15.10.2023