Abstract
AimThere are studies indicating an increase in cytokine levels at the cellular level during the progression of adrenocortical masses and their development into cancer. Additionally, it is known that neutrophil migration and platelet activity play fundamental roles in the immune response, which has anti-tumor effects in all organs. Therefore, this study aims to investigate whether peripheral blood parameters such as the Neutrophil-to-Lymphocyte Ratio (NLR), Platelet-to-Lymphocyte Ratio (PLR), and Lymphocyte-to-Monocyte Ratio (LMR) serve as decisive factors related to the pathological outcomes of adrenocortical lesions.MethodsThis study was conducted retrospectively by reviewing the records of 37 patients who underwent open or laparoscopic adrenalectomy for adrenal masses at a tertiary center between 2015 and 2020. Patients were categorized based on pathology results into adenoma, non-adenomatous benign lesions, metastatic lesions, pheochromocytoma, and primary malignant tumors (malignant (n=11), benign (n=26)). The relationship between lesion size and neutrophil, NLR, LMR, and PLR values among these five groups was examined.ResultsA statistically significant positive correlation was observed between lesion size and NLR and neutrophil values (r=0.396, p=0.017 and r=0.361, p=0.030, respectively). Additionally, it was found that NLR values were elevated at non-statistically significant levels in adrenocortical cancers (p=0.460).ConclusionIn our study, a positive correlation was established between lesion size and NLR and neutrophil values. We anticipate that during the perioperative period, insights into the nature of the lesion can be gained by considering hematological parameters.
Keywords
Introduction
Adrenocortical masses are rare lesions among the spectrum of endocrine tumors.1 Adrenocortical malignant lesions, on the other hand, account for approximately 0.02% to 0.2% of cancer-related deaths and are reported to have a poor prognosis.2 Some scoring systems and genetic panels are used as prognostic indicators alongside the evaluation of surgical specimens.3 Hematological parameters reflecting alterations in leukocyte, neutrophil, and platelet levels serve as indicators of systemic inflammation.4 They also serve as indicators of the immune system and chronic inflammation. Various studies have shown that cytokine levels increase at the cellular level during the progression of adrenal masses and their development into cancer.5 Additionally, it is known that neutrophil migration plays fundamental roles in the immune response with anti-tumor activity in all organs.6 However, the presence and relationship of inflammation and the immune system in the process of adrenal neoplasia have not yet been clearly defined. While there are many markers that reflect the complex nature of inflammation and the immune system in various aspects, hematological parameters are easily accessible and among the fundamental markers.7
Neutrophil-to-Lymphocyte Ratio (NLR), Platelet-to-Lymphocyte Ratio (PLR), and Lymphocyte-to-Monocyte Ratio (LMR) obtained from peripheral blood samples have been shown to be potentially associated with prognosis in various cardiovascular diseases, inflammatory diseases, and malignancies.8-9-10 For example, NLR has been identified as a positive predictive value for breast, prostate, and colorectal cancers and can be obtained at a low cost.11,12 While NLR and PLR ratios are frequently used in a prognostic context for many diseases, there is currently a lack of sufficient research investigating these values in adrenal masses and different adrenal lesion groups, both with and without adrenal masses.
Based on these considerations, our study aimed to investigate whether peripheral blood parameters such as NLR, PLR, and LMR (lymphocyte-to-monocyte ratio) serve as decisive factors for the pathological examination results of adrenocortical lesions.
Materials and Methods
Ethical approval was obtained before the commencement of the study. In this study, records of patients who underwent open or laparoscopic adrenalectomy for adrenal masses at a tertiary center’s general surgery clinic between 2015 and 2020 were retrospectively reviewed. Patients’ clinical characteristics, findings, sociodemographic features, and operation notes were accessed from file records and the electronic database.
Parameters assessed and included in the analysis for all patients in this research were as follows: medical history, medication use, smoking status, personal background, other physical examination findings, and previous laboratory results (routine complete blood count evaluation, laboratory tests associated with possible diseases). When evaluating hemogram parameters, the values obtained within the latest 2 weeks before adrenalectomy were considered. Patients were categorized into five groups based on pathology results: adenoma, non-adenomatous benign lesions, metastatic lesions, pheochromocytoma, and primary malignant tumors. The results of the study patients were evaluated, and groups were compared in terms of lesion size, neutrophil, lymphocyte and platelet counts and; NLR, PLR, and LMR values.
Exclusion Criteria
Patients with immunosuppression, active infections, recent blood transfusions, or ongoing chemotherapy were excluded from the study.Ethical ApprovalThe study was approved by the Ethics Committee of Pamukkale University (Date: 16.02.2021, Decision No: 04).Statistical AnalysisDescriptive values of quantitative continuous variables (such as age) were examined using standard descriptive statistical methods (arithmetic mean, standard deviation, median). Categorical variables (frequency of occurrence) were presented with frequencies and percentages of the total. The evaluation of quantitative measurements was performed using Student’s t-test or the Wilcoxon signed-rank test according to the distribution characteristics of the data. Comparisons of categorical variables were made using Chi-square or Fisher’s Exact test depending on the distribution of case distributions. Correlations between analysis variables were evaluated using linear regression models.Reporting GuidelinesThe study was reported in accordance with STROBE guidelines.
Results
It was determined that 48.6% of the patients (n=18) were female, and 51.4% (n=39) were male. Furthermore, 48.6% of the patients (n=18) had adenomas, 16.2% (n=6) had metastatic lesions, 10.8% (n=4) had non-adenomatous benign lesions, 10.8% (n=4) had pheochromocytoma, and 13.5% (n=5) were diagnosed with primary malignant tumors. Additionally, it was found that 70.3% of the patients (n=26) had benign tumors, while 29.7% (n=11) had malignant tumors. The average age of the patients was 53.65±11.82. Sociodemographic data of the patients are summarized in Table 1.
The patients had an average neutrophil count of 5.28±2.33, platelet count of 282.13±128.54, NLR value of 3.00±1.80, PLR value of 151.13±73.34, LMR value of 4.75±6.89, and lesion diameter of 38.94±18.77. The clinical and hematological parameters of the patients are presented in Table 2.
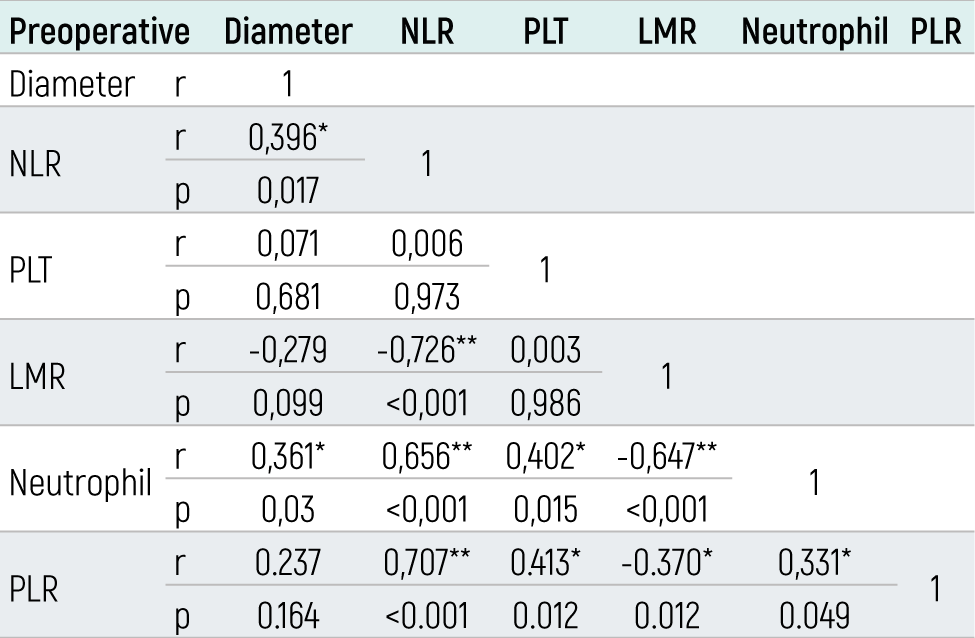
The correlation between lesion diameter, neutrophil and platelet counts, NLR, PLR, LMR is shown in Table 3. A statistically significant positive correlation was found between lesion diameter and NLR values (r=0.396, p=0.017). However, there was no statistically significant relationship between lesion diameter and platelet values (r=0.071, p=0.681), PLR (r=0.237, p=0.164), and LMR (r=-0.279, p=0.099) values. A positive statistically significant difference was found between lesion diameter and neutrophil values (r=0.361, p=0.030).
When comparing the mean values of neutrophil counts (p=0.400) and platelet counts (p=0.430), NLR (p=0.292), LMR (p=424), and PLR (p=0.305) between the groups, no statistically significant difference was observed. Similarly, there was no statistically significant difference in neutrophil counts (p=0.668), platelet counts (p=0.164), NLR (p=.460), LMR (p=0.204), and PLR (p=0.440) values among all groups.
Discussion
The existing findings in the literature strongly indicate a notable correlation between neutrophils, specifically NLR and PLR, with adverse outcomes observed across a spectrum of cancer types.13 This intriguing relationship raises a debate about the intricate interplay between inflammation and cancer pathogenesis. It has been hypothesized that cancer frequently emerges within environments marked by persistent inflammation, characterized by the presence of immune cells releasing various factors that not only sustain the inflammatory milieu but also fuel the proliferation of tumor cells.4,5 This hypothesis underpins the theory that inflammation plays a pivotal role in the initiation and progression of cancer.
Nevertheless, the functional dynamics and mechanisms governing the interconnection between inflammation and cancer have remained a focal point of scientific inquiry for a considerable period. Researchers and clinicians have sought to elucidate the intricate web of interactions between the immune system and tumorigenesis, yet definitive results remain elusive. The complexity of this relationship, coupled with the heterogeneity of cancer subtypes and individual patient responses, underscores the need for further rigorous investigation and a multifaceted approach to uncover the precise mechanisms driving the association between inflammation and cancer. Future research endeavors hold promise for shedding light on inflammation and cancer.
Measuring hematologic parameters like NLR and PLR values during the perioperative period is a straightforward and cost-effective practice. As a result, they serve as valuable markers for predicting the long-term outcomes of various malignancies. Meta-analyses have consistently shown that elevated NLR ratios in the preoperative phase can serve as unfavorable prognostic indicators in solid tumors undergoing curative resection.14 He and his colleagues have also demonstrated that increased NLR levels are a prognostic factor in metastatic colorectal cancers. Furthermore, it has been established that high NLR and PLR values hold predictive value for prognosis in adrenocortical cancers.15 In our study, we also found elevated NLR values in malignant adrenal tumors compared to other groups, although the difference was not statistically significant (benign: 2.84 ± 1.68, malignant: 3.35 ± 2.09, p: 0.460).
Bagante et al.15 conducted an investigation using a multi-center database and analyzed 84 patients diagnosed with adrenocortical carcinoma. Despite the inclusion of data from 13 major centers across the United States, the low number of patients reflects the rarity of this disease. Their study revealed associations between elevated NLR and PLR with larger tumors and the necessity for resecting other organs. Notably, an elevated NLR and PLR were both linked to five-year recurrence-free survival (both P < 0.05). In multivariate survival analyses, PLR remained a predictor of recurrence-free survival (HR 1.72), while NLR was associated with both disease-specific survival (HR 2.21) and recurrence-free survival (HR 1.99) (both P < 0.05).
Mochizuki et al.16 conducted a retrospective analysis of 59 patients diagnosed with adrenal tumors over an 11-year period, including 13 cases of malignant disease and 46 with benign disease. They found that the NLR in malignant adrenal tumor specimens was significantly higher than in non-malignant specimens (p = 0.028), with adrenocortical carcinoma exhibiting the highest NLR among all adrenal tumors. Importantly, in carcinoma cases, the higher NLR group demonstrated significantly poorer overall survival than the lower NLR group (p = 0.032). The authors concluded that a higher NLR indicates a greater likelihood of malignancy and suggested that the NLR could serve as a novel biomarker for predicting the prognosis of patients with adrenal tumors. It is worth noting that, as a limitation of our study, we did not investigate the prognosis and survival outcomes of our patient cohort.
In a more recent study, De Jong and colleagues examined 57 patients, 26 of whom had hormonally active adrenal cortical masses. There were no differences between the two groups in terms of age, gender, and tumor characteristics. In this study, both a high NLR [HR = 2.24 (95% CI: 1.07–4.70); p = 0.03] and a high PLR [HR = 4.02 (95% CI: 1.80–8.98); p = 0.001] were strongly associated with shorter overall survival in unadjusted analyses. The authors concluded that in patients with adrenocortical cancer during the preoperative period, elevated NLR and PLR ratios shortened overall survival, and high PLR ratios were also associated with earlier recurrence.17 Balkwill and colleagues suggested that inflammatory cells and cytokines present in tumors are more likely to contribute to tumor growth, progression, and immunosuppression in the host, rather than eliciting an anti-tumor response.18 Studies have shown that as tumor size increases, the likelihood of the lesion being malignant also rises.19 In our study, a positive correlation was found between lesion size and NLR and neutrophil count [ (r=0.396, p=0.017) - (r=0.361, p=0.030) retrospectively ].
Limitations
Our study has several limitations that should be taken into account. Firstly, it had a retrospective design, and the relatively small sample size was primarily due to the rarity of adrenocortical carcinoma (ACC). This limitation restricted our ability to conduct specific statistical analyses and increased the risk of type II statistical errors. Additionally, we did not include survival data in the analysis, which is crucial for assessing prognosis.
Conclusion
Immune markers such as Neutrophil-to-Lymphocyte Ratio (NLR), Lymphocyte-to-Monocyte Ratio (LMR), and Platelet-to-Lymphocyte Ratio (PLR) may prove valuable for stratifying patients based on the types of adrenocortical lesions they have. These markers could potentially aid in categorizing patients into different risk groups and influencing treatment and follow-up protocols. Given their cost-effectiveness and ready availability, they could easily complement existing prognostic markers. Thus, further prospective studies, as conducted in other malignancies, are needed to explore their utility.
Declarations
Informed Consent
Informed consent was waived due to the retrospective study design.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare no conflict of interest.
Funding
None.
Abbreviations
LMR: Lymphocyte-to-monocyte ratio
NLR: Neutrophil-to-lymphocyte ratio
PLR: Platelet-to-lymphocyte ratio
References
- Lam AK. Update on adrenal tumours in 2017 World Health Organization (WHO) of endocrine tumours. Endocr Pathol. 2017;28(3):213-227. doi:10.1007/s12022-017-9484-5
- Mansmann G, Lau J, Balk E, Rothberg M, Miyachi Y, Bornstein SR. The clinically inapparent adrenal mass: update in diagnosis and management. Endocr Rev. 2004;25(2):309-340. doi:10.1210/er.2002-0031
- Pennanen M, Tynninen O, Kytölä S, et al. IDH1 expression via the R132H mutation-specific antibody in adrenocortical neoplasias: prognostic impact in carcinomas. J Endocr Soc. 2020;4(4). doi:10.1210/jendso/bvaa018
- Herrero-Cervera A, Soehnlein O, Kenne E. Neutrophils in chronic inflammatory diseases. Cell Mol Immunol. 2022;19(2):177-191. doi:10.1038/s41423-021-00832-3
- Lippitz BE. Cytokine patterns in patients with cancer: a systematic review. Lancet Oncol. 2013;14(6). doi:10.1016/s1470-2045(12)70582-x
- Xiong S, Dong L, Cheng L. Neutrophils in cancer carcinogenesis and metastasis. J Hematol Oncol. 2021;14(1):173. doi:10.1186/s13045-021-01187-y
- Targońska-Stępniak B, Zwolak R, Piotrowski M, Grzechnik K, Majdan M. The relationship between hematological markers of systemic inflammation (neutrophil-to-lymphocyte, platelet-to-lymphocyte, lymphocyte-to-monocyte ratios) and ultrasound disease activity parameters in patients with rheumatoid arthritis. J Clin Med. 2020;9(9):2760. doi:10.3390/jcm9092760
- Detopoulou P, Panoutsopoulos GI, Mantoglou M, et al. Relation of mean platelet volume (MPV) with cancer: a systematic review with a focus on disease outcome on twelve types of cancer. Curr Oncol. 2023;30(3):3391-3420. doi:10.3390/curroncol30030258
- Cupp MA, Cariolou M, Tzoulaki I, Aune D, Evangelou E, Berlanga-Taylor AJ. Neutrophil to lymphocyte ratio and cancer prognosis: an umbrella review of systematic reviews and meta-analyses of observational studies. BMC Med. 2020;18(1):360. doi:10.1186/s12916-020-01817-1
- Van Berckelaer C, Van Geyt M, Linders S, et al. A high neutrophil-lymphocyte ratio and platelet-lymphocyte ratio are associated with a worse outcome in inflammatory breast cancer. Breast. 2020;53:212-220. doi:10.1016/j.breast.2020.08.006
- Walsh SR, Cook EJ, Goulder F, Justin TA, Keeling NJ. Neutrophil-lymphocyte ratio as a prognostic factor in colorectal cancer. J Surg Oncol. 2005;91(3):181-184. doi:10.1002/jso.20329
- Kawahara T, Yokomizo Y, Ito Y, et al. Pretreatment neutrophil-to-lymphocyte ratio predicts the prognosis in patients with metastatic prostate cancer. BMC Cancer. 2016;16:111. doi:10.1186/s12885-016-2134-3
- Templeton AJ, McNamara MG, Šeruga B, et al. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: a systematic review and meta-analysis. J Natl Cancer Inst. 2014;106(6). doi:10.1093/jnci/dju124
- Paramanathan A, Saxena A, Morris DL. A systematic review and meta-analysis on the impact of preoperative neutrophil lymphocyte ratio on long-term outcomes after curative intent resection of solid tumours. Surg Oncol. 2014;23(1):31-39. doi:10.1016/j.suronc.2013.12.001
- Bagante F, Tran TB, Postlewait LM, et al. Neutrophil-lymphocyte and platelet-lymphocyte ratio as predictors of disease-specific survival after resection of adrenocortical carcinoma. J Surg Oncol. 2015;112(2):164-172. doi:10.1002/jso.23982
- Mochizuki T, Kawahara T, Takamoto D, et al. The neutrophil-to-lymphocyte ratio predicts adrenocortical carcinoma and is correlated with the prognosis. BMC Urol. 2017;17(1):49. doi:10.1186/s12894-017-0240-4
- de Jong MC, Mihai R, Khan S. Neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio as possible prognostic markers for patients undergoing resection of adrenocortical carcinoma. World J Surg. 2021;45(3):754-764. doi:10.1007/s00268-020-05868-6
- Balkwill F, Mantovani A. Inflammation and cancer: back to Virchow? Lancet. 2001;357(9255):539-545. doi:10.1016/s0140-6736(00)04046-0
- Lebastchi AH, Kunstman JW, Carling T. Adrenocortical carcinoma: current therapeutic state-of-the-art. J Oncol. 2012;2012:234726. doi:10.1155/2012/234726
Tables
Table 1. Demographics variables of the patients.
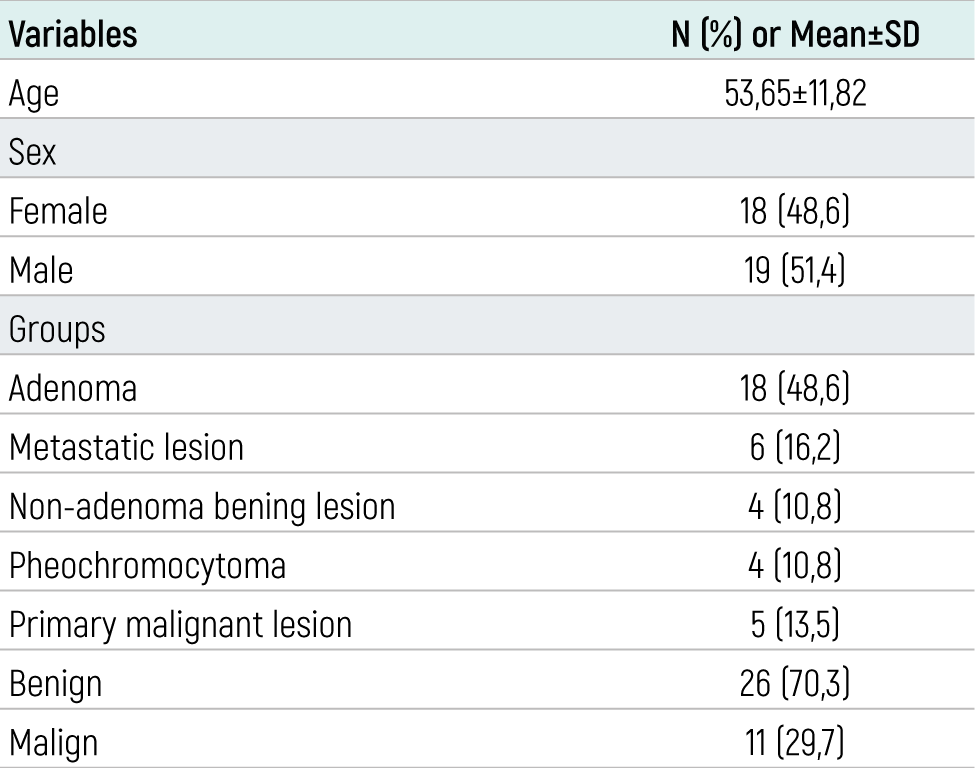
Table 2. Laboratory parameters of the patients.
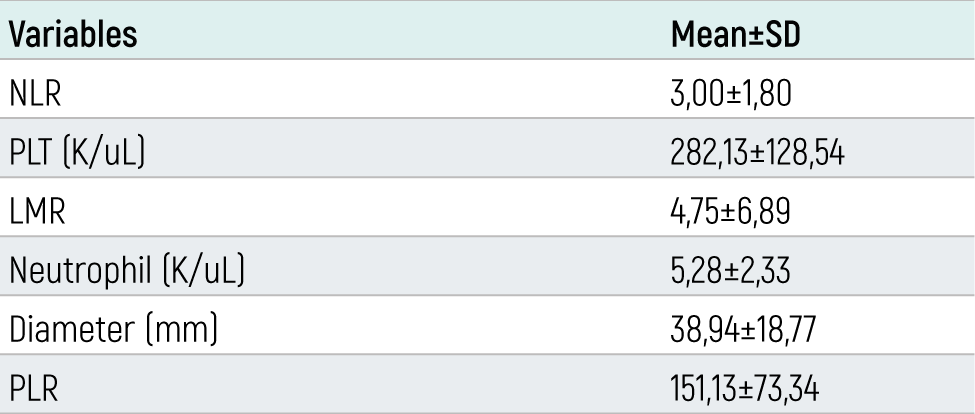
Table 3. Correlation between diameter of the lesion, NLR, PLT, LMR and Neutrophil values.
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Utku Özgen, Sevda Yılmaz, Muhammed Raşid Aykota. Evaluation of neutrophil/lymphocyte ratio and other hematological parameters on types of adrenocortical masses and their predictive value. doi:10.4328/ECAM.10072
- Received:
- 29.09.2023
- Accepted:
- 13.10.2023
- Published Online:
- 14.10.2023
- Printed:
- 15.10.2023