Abstract
AimKnee Osteoarthritis (OA) is a major cause of pain and disability in older adults. Of the cytokines identified in osteoarthritic joints, interleukin-1 (IL-1) appears to be of particular importance. The present study is a random ized, prospective, single-institution study to determine the effect of interleukin 1 ß receptor antagonist (IL-1ß Ra) in OA; we made this analysis by injecting symmetrically involved knees.MethodsThe present study comprised 33 patients (19 female, 14 male) with 66 knees with a mean age 57.6 (range 41-70 years). Patients were included in the study if they had radiologically-verified bilateral grade 2-3 OA of the knee according to Kellgren-Lawrence classification. The patients were analyzed with Visual Ana logue Scale (VAS) for pain, Knee Injury and Osteoarthritis Score (KOOS), and Knee Society Score (KSS) before the first injection was administered (pre-treatment) and again one year after the last injection (post-treatment).ResultsTreatment with ACS consistently showed significant decrease in VAS score (p<0.01). The patients report ed a significant improvement in KOOS (subscores and total) one year after ACS treatment (p<0.01). The increase in KSS score from baseline to post-treatment one year also was significant (p<0.01).ConclusionIntra-articular injection of ACS (Orthokine) in patients with painful knee OA has an excellent safety profile and results in a strong clinical response. The data show that ACS (Orthokine) represents an effective and well-tolerated alternative to currently predominant treatments of OA.
Keywords
Introduction
Osteoarthritis (OA) is the single most important cause of locomotor disability in western societies and a major burden on their healthcare systems.1-2 It is a progressive, chronic condition leading to pain and loss of function that dramatically reduces patients’ quality of life and ability to work. Knee Osteoarthritis (OA) is a major cause of pain and disability in older adults.3 It is the most common type and encountered in 6% of adults, with a prevalence reaching 40% in advanced age (>70 years).4 Pain control is one of the main goals in the treatment of knee OA.5 The management of knee OA begins with conservative treatments such as physical therapy, exercise, weight loss, and medications. Pharmacologic treatment options for OA used to be restricted to the symptomatic use of analgesics, non-steroidal anti-inflammatory drugs (NSAIDs), and the intra-articular injection of steroids or hyaluronan (HA).6-7-8-9-10-11 Intra-articular HA is commonly used as a safe, off-the-shelf treatment for OA of the knee, but its efficacy is controversial. There is a pressing need for novel, improved, mechanism-based agents for treating OA. Surgical intervention can be indicated for patients with advanced OA.12
In OA, the destruction of hyaline cartilage constitutes the central pathological mechanism causing various mechanical and biological dysfunctions within the joint. Of the cytokines identified in osteoarthritic joints, interleukin-1 (IL-1) appears to be of particular importance. Accordingly, the IL-1 receptor antagonist protein (IRAP), a naturally occurring inhibitor of IL-1, has been reported to limit the intra-articular damage associated with IL-1.11-12 In animal models,many researchers have succeeded in positively modifying the osteoarthritic disease process by effectively antagonising IL-1.11-12-13 Autologous conditioned serum (ACS) is an example of a presumably disease-modifying treatment for OA based on antagonising the intra-articular effects of IL-1.13 The resulting conditioned serum contains elevated levels of various anti-inflammatory cytokines, such as IRAP, IL-4, and IL-10.11,14-15 Several investigators have reported effectiveness of IL-1Ra when delivered by intra-articular injection in a canine model of OA and in a pilot human study.16 After initial scepticism and the positive outcome of an animal model, recent prospective randomized controlled double-blind trials have provided the first evidence in human samples demonstrating that Orthokin® (Orthogen, Düsseldorf, Germany) is more effective than placebo and/or HA for the treatment of knee OA.11,17-18-19 The present study is a randomized, prospective, single-institution study to determine the effect of interleukin 1 ß receptor antagonist (IL-1ß Ra) in OA; we made this analysis by injecting symmetrically involved knees.
Materials and Methods
After approval by the institutional review board and with written informed patient consent, 33 patients (19 female, 14 male) not older than 70 years with 66 knees were included in the study. Data collection and treatment took place at a single institution. This study was based on a one-year prospective, randomized, controlled clinical trial.PatientsAll patients presented to the orthopedic outpatient clinic with a bilateral knee pain score equal to or more than 4 points of 0-10 Visual Analogue Scale (VAS) on the day of the examination. To evaluate pain severity, analgesic and anti-inflammatory medications were discontinued before the start of treatment. The wash-out period was 3 weeks starting from the day of inclusion until the first injection. Patients were included in the study if they had radiologically-verified bilateral grade 2-3 OA of the knee according to Kellgren-Lawrence classification.20 All patients in this study were dissatisfied with previous attempts at conservative
treatment, including non-steroidal anti-inflammatory drugs. No patient dropped out or underwent surgery while enrolled in the study. Secondary arthritis, grade IV OA, systemic or inflammatory joint diseases, a history of a crystalline arthropathy, clinically relevant hematologic or abnormal clinical chemistry values, bone cancer, and metastatis or tumor-like lesions in immediate proximity to the treated joint, joint instability, intra-articular corticosteroid injection within the previous 6 months, history of diabetes mellitus, recent history of trauma to the knee, and BMI greater than 30 were exclusion criteria. Patients were also excluded if they had contraindication to injection, such as infection, anticoagulation therapy, allergy, or hypersensitivity to any of the study medications. Patients who use systemic corticosteroids were also excluded. Patients who had VAS difference more than 2 points between their knees were excluded from the study.Outcome MeasurementsAll patients were analyzed with Visual Analogue Scale (VAS) for pain, which ranges from 0 (no pain) to 10 (most severe pain), Knee Injury and Osteoarthritis Score (KOOS), and Knee Society Score (KSS) before the first injection was administered (pre-treatment) and again one year after the last injection (post-treatment).21ACS PreparationTo produce ACS, 50 mL of whole blood were taken from each patient using a special syringe with increased internal surface area (Orthogen, Düsseldorf, Germany); glass beads in the syringes increase the non-pyrogenic surface area and induce the dose-dependent production of IRAP (among others) by white blood cells in whole blood incubated at 37°C. After incubation, the blood-filled syringes were centrifuged, and the serum supernatant was filtered (0.22 mm; Millipore, Carrigtwohill, Co. Cork, Ireland) and aliquoted into 6-8.2 mL portions. The aliquots were stored at -20°C until use. A randomization procedure was followed to assign each compound to the right or the left knee.Administration of InjectionOne orthopedic surgeon in one center applied all of the injections. Patients were placed in the sitting position with 90 degrees of knee flexion. A lateral approach to the knee was selected. The skin of the injection site was cleaned with povidone-iodine solution. No anesthetic was administered before injection. ACS was injected in a sterile condition into the affected joint in a series of six intra-articular injections given twice a week for three weeks. The patient was sent home after injection. Limited movement was allowed for 24 hours and resting was recommended in case of pain. The patient was recommended not to receive non-steroidal inflammatory drugs (NSAIDs) and not to locally apply ice for a week after injection in order not to reduce efficacy of ACS. In addition, an exercise program was given to the patients and performing normal daily activities was recommended when tolerable.Another surgeon who was not aware of the study design performed the clinical evaluation. Patients underwent clinical evaluation before the injection and at the first-year control. The possible complications and side effects were also evaluated in each visit.Statistical AnalysisStatistical analysis was performed using NCSS (Number Cruncher Statistical System) 2007 (Kaysville, Utah, USA). Descriptive statistics were expressed as number and percentage for categorical variables and as mean, standard deviation, median, minimum, and maximum for numerical variables. Paired Samples t Test was used to test whether variables were distributed normally. Wilcoxon Signed Ranks Test was used to test whether variables were distributed non-normally. p<0.01 were considered statistically significant.
Results
The present study comprised 33 patients (19 female, 14 male) with 66 knees with a mean age 57.6 (range 41-70 years); the general characteristics of the patents are shown in Table 1. These patients were highly symptomatic. At the first admission, the mean VAS score was 7.3 ± 0.9 on the right side and 7.7 ± 1.2 on the left side. The change in VAS score before and after treatment was statistically significant. Treatment with ACS consistently showed a significant decrease in VAS score (p<0.01) (Table 2, 3).
No intra-articular injection-related major complications such as infection, deep venous thrombosis, or muscular atrophy were detected in any of the patients over the course of treatments.
ACS (Orthokine) resulted in significantly greater improvement over a one-year period bilaterally. When asked retrospectively to rate their health, the patients reported a significant improvement in KOOS (subscores and total) one year after ACS treatment (p<0.01). It is interesting that retrospectively, they rated their initial health (all outcomes of KOSS) as being lower than the ratings they gave before the actual ACS treatment (Table 2, 3).
By the end of the study, there was a significant improvement in the KSS score over time. Increase in KSS score from baseline to post-treatment 1 year was significant (p<0.01) (Table 2, 3).
Discussion
OA is accompanied by a number of mechanical and biologic dysfunctions within the joint, the central pathologic feature being the destruction of hyaline cartilage. Of the catabolic cytokines identified in osteoarthritic joints, IL-1, the most potent known mediator of artilage loss22-23-24-25-26-27-28-29-30-31, appears pivotal. The naturally occurring inhibitor of IL-1, the IL-1 receptor antagonist (IL-1Ra) could potentially limit the intra-articular actions of IL-1 and thereby control the disease process.32-33-34 NSAIDs give only modest control over the signs and ymptoms of OA. Scholes et al. have reported that only 15% of patients with OA of the knee for whom a NSAID was prescribed were still taking the same drug 12 months later.35 Certain cyclooxygenase-2 (COX-2) inhibitors have recently been withdrawn as a result of cardiovascular complications.10 The future of this class of drugs is now unclear. Their claimed qualification as OA medication may possibly be due to what has been until now a lack of effective treatment alternatives. Interleukin (IL)-1b is a pivotal mediator of many inflammatory and regenerative diseases, including osteoarthritis (OA), rheumatoid arthritis (RA), and spinal disorders. Strategies for inhibiting the biological activities of IL-1b include use of the recombinant IL-1 receptor agonist, soluble forms of IL-1 receptors, and anti-inflammatory cytokines such as IL-4, IL-10, and IL-13, which inhibit the synthesis of IL-1, increase the synthesis of IL-1Ra, or both. A biologic therapeutic preparation known as ACS or Orthokine (Orthokine, Dusseldorf, Germany) has been developed and used clinically in orthopedic patients suffering from OA, RA, and spinal disorders. ACS is prepared from peripheral whole blood. Briefly, blood is drawn into a syringe containing treated glass beads with CrSO4 to initiate monocyte activation.36 ACS was developed in the mid-1990s in an attempt to generate an injectable material enriched in endogenous IL-1Ra as a novel therapeutic for OA. Meijer et al. noted that exposure of blood to glass beads elicits a vigorous, rapid increase in the synthesis of several anti-inflammatory cytokines, including IL-1Ra.37 This observation is the basis for producing ACS, which is injected into the affected joint in a series of six intra-articular injections given twice a week for 3 weeks. This therapy is currently available for humans in several countries and its use is even more widespread for equine OA, where ACS considerably improves clinical lameness in horses and may protect cartilage from degradation.10 Our data show that ACS (Orthokine) is safe and has a therapeutic effect on the major clinical parameters of painful knee OA. ACS resulted in significantly greater improvement over one year. Furthermore, patients treated with ACS consistently showed significantly greater improvements compared to the pre-treatment parameters. Remarkably, the therapeutic effect persists for at least one year. The ACS production process has been shown to reproducibly elevate IL-1Ra and other factors, although the mechanisms by which the effects are mediated are not fully understood.35-36,38 The multitude of synergistic, active therapeutic molecules may explain the observed clinical effect, but its long-term persistence is more difficult to explain. One possibility may be that the therapeutic molecules help to re-establish a healthy joint homeostasis.19
In summary, intra-articular ACS (Orthokine) reduces pain and increases function and mobility for up to 1 year, based on our clinical trial results. It can be considered as clinically very safe because of its autologous origin. No clinically serious side effects were observed in the ACS group during the observation period. We conclude that ACS is effective for treatment of patients with low- to medium-grade, painful knee OA. We treated only patients with grade 2-3 OA of the knee according to Kellgren-Lawrence classification, so the results can not necessarily be generalized to all OA patients. Although this study supports the use of ACS in mid-stage painful OA of the knee, we are aware of its limitations.
Conclusion
Intra-articular injection of ACS (Orthokine) in patients with painful knee OA has an excellent safety profile and results in a strong clinical response. The data show that ACS (Orthokine) represents an effective and well-tolerated alternative to currently predominant treatments of OA.
Declarations
Informed Consent
Informed consent was obtained from all participants.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
None.
References
- Gupta S, Hawker GA, Laporte A, Croxford R, Coyte PC. The economic burden of disabling hip and knee osteoarthritis (OA) from the perspective of individuals living with this condition. Rheumatology (Oxford). 2005;44(12):1531-1537. doi:10.1093/rheumatology/kei049
- Peat G, McCarney R, Croft P. Knee pain and osteoarthritis in older adults: a review of community burden and current use of primary health care. Ann Rheum Dis. 2001;60(2):91-97. doi:10.1136/ard.60.2.91
- Hadler NM. Osteoarthritis as a public health problem. Clin Rheum Dis. 1985;11:175-185. doi:10.1016/s0307-742x(21)00538-5
- Michael JW, Schlüter-Brust KU, Eysel P. The epidemiology, etiology, diagnosis, and treatment of osteoarthritis of the knee. Dtsch Arztebl Int. 2010;107(9):152-162. doi:10.3238/arztebl.2010.0152
- Raynauld JP, Buckland-Wright C, Ward R, et al. Safety and efficacy of long-term intra-articular steroid injections in osteoarthritis of the knee: a randomized, double-blind, placebo-controlled trial. Arthritis Rheum. 2003;48:370-377. doi:10.1002/art.10777
- Juni P, Nartey L, Reichenbach S, Sterchi R, Dieppe PA, Egger M. Risk of cardiovascular events and rofecoxib: cumulative meta-analysis. Lancet. 2004;364:2021-2029.
- Zhang W, Moskowitz RW, Nuki G, et al. OARSI recommendations for the management of hip and knee osteoarthritis, part I: critical appraisal of existing treatment guidelines and systematic review of current research evidence. Osteoarthritis Cartilage. 2007;15(9):981-1000. doi:10.1016/j.joca.2007.06.014
- Jordan KM, Arden NK, Doherty M, et al. EULAR recommendations 2003: an evidence-based approach to the management of knee osteoarthritis: report of a task force of the ESCISIT. Ann Rheum Dis. 2003;62(12):1145-1155. doi:10.1136/ard.2003.011742
- Schnitzer TJ. Update of ACR guidelines for osteoarthritis: role of the coxibs. J Pain Symptom Manage. 2002;23:24-30. doi:10.1016/s0885-3924(02)00372-x
- Hernandez-Diaz S, Varas-Lorenzo C, Garcia Rodriguez LA. Nonsteroidal antiinflammatory drugs and the risk of acute myocardial infarction. Basic Clin Pharmacol Toxicol. 2006;98(3):266-274.
- Baltzer A, Moser C, Jansen S, Krauspe R. Autologous conditioned serum (Orthokine) is an effective treatment for knee osteoarthritis. Osteoarthritis Cartilage. 2009;17:152-160. doi:10.1016/j.joca.2008.06.014
- Frisbie DD, Ghivizzani SC, Robbins PD, Evans CH, McIlwraith CW. Treatment of experimental equine osteoarthritis by in vivo delivery of the equine interleukin-1 receptor antagonist gene. Gene Ther. 2002;9:12-20. doi:10.1038/sj.gt.3301608
- Fernandes JC, Tardif G, Martel-Pelletier J, et al. In vivo transfer of interleukin-1 receptor antagonist gene in osteoarthritic rabbit knee joints: prevention of osteoarthritis progression. Am J Pathol. 1999;154:1159-1169. doi:10.1016/s0002-9440(10)65368-0
- Rutgers M, Saris DB, Dhert WJ, Creemers LB. Cytokine profile of autologous conditioned serum for treatment of osteoarthritis: in vitro effects on cartilage metabolism and intra-articular levels after injection. Arthritis Res Ther. 2010;12:R114. doi:10.1186/ar3050
- Wehling P, Reinecke J, Baltzer A, et al. Clinical responses to gene therapy in joints of two subjects with rheumatoid arthritis. Hum Gene Ther. 2009;20:97-101. doi:10.1089/hum.2008.075
- Chevalier X, Giraudeau B, Conrozier T, et al. Safety study of intra-articular injection of interleukin 1 receptor antagonist in patients with painful knee osteoarthritis: a multicenter study. J Rheumatol. 2005;32(7):1317-1323.
- Burmester GR, Grifka J. Revision of the recommendations of the Commission on the Pharmacotherapy of the German Society for Rheumatology. Z Rheumatol. 2007;66:83-84.
- Frisbie DD, Kawcak CE, Werpy NM, et al. Clinical, biochemical, and histologic effects of intra-articular administration of autologous conditioned serum in horses with experimentally induced osteoarthritis. Am J Vet Res. 2007;68:290-296. doi:10.2460/ajvr.68.3.290
- Yang KG, Raijmakers NJ, van Arkel ER, et al. Autologous interleukin-1 receptor antagonist improves function and symptoms in osteoarthritis when compared to placebo in a prospective randomized controlled trial. Osteoarthritis Cartilage. 2008;16:498-505. doi:10.1016/j.joca.2007.07.008
- Kellgren JH, Lawrence JS. Radiological assessment of osteoarthrosis. Ann Rheum Dis. 1957;16:494-501. doi:10.1136/ard.16.4.494
- Freyd M. The graphic rating scale. J Educ Psychol. 1923;14:83-102. doi:10.1037/h0074329
- Goldring MB. Osteoarthritis and cartilage: the role of cytokines. Curr Rheumatol Rep. 2000;2:459-465. doi:10.1007/s11926-000-0021-y
- Goldring SR, Goldring MB. The role of cytokines in cartilage matrix degeneration in osteoarthritis. Clin Orthop Relat Res. 2004;(427):27-36. doi:10.1097/01.blo.0000144854.66565.8f
- Fernandes JC, Martel-Pelletier J, Pelletier JP. The role of cytokines in osteoarthritis pathophysiology. Biorheology. 2002;39:237-246. doi:10.1177/0006355x2002039001002025
- Karsenty G. An aggrecanase and osteoarthritis. N Engl J Med. 2005;353(5):522-523. doi:10.1056/nejmcibr051399
- Myers SL, Brandt KD, Ehlich JW, et al. Synovial inflammation in patients with early osteoarthritis of the knee. J Rheumatol. 1990;17(12):1662-1669.
- Fukui N, Purple CR, Sandell LJ. Cell biology of osteoarthritis: the chondrocyte’s response to injury. Curr Rheumatol Rep. 2001;3(6):496-505. doi:10.1007/s11926-001-0064-8
- Smith MD, Triantafillou S, Parker A, et al. Synovial membrane inflammation and cytokine production in patients with early osteoarthritis. J Rheumatol. 1997;24(2):365-371.
- Silvestri T, Pulsatelli L, Dolzani P, et al. In vivo expression of inflammatory cytokine receptors in the joint compartments of patients with arthritis. Rheumatol Int. 2006;26(4):360-368. doi:10.1007/s00296-005-0586-x
- Pettipher ER, Higgs GA, Henderson B. Interleukin 1 induces leukocyte infiltration and cartilage proteoglycan degradation in the synovial joint. Proc Natl Acad Sci U S A. 1986;83(22):8749-8753. doi:10.1073/pnas.83.22.8749
- Pelletier JP, Faure MP, DiBattista JA, et al. Coordinate synthesis of stromelysin, interleukin-1, and oncogene proteins in experimental osteoarthritis: an immunohistochemical study. Am J Pathol. 1993;142(1):95-105.
- Arend WP, Malyak M, Guthridge CJ, Gabay C. Interleukin-1 receptor antagonist: role in biology. Annu Rev Immunol. 1998;16:27-55. doi:10.1146/annurev.immunol.16.1.27
- Dinarello CA. Interleukin-1 and interleukin-1 antagonism. Blood. 1991;77(8):1627-1652. doi:10.1182/blood.v77.8.1627.bloodjournal7781627
- Dinarello CA. The role of the interleukin-1 receptor antagonist in blocking inflammation mediated by interleukin-1. N Engl J Med. 2000;343(10):732-734. doi:10.1056/nejm200009073431011
- Scholes D, Stergachis A, Penna PM, Normand EH, Hansten PD. Nonsteroidal antiinflammatory drug discontinuation in patients with osteoarthritis. J Rheumatol. 1995;22(4):708-712.
- Arend WP, Leung DY. IgG induction of IL-1 receptor antagonist production by human monocytes. Immunol Rev. 1994;139:71-78. doi:10.1111/j.1600-065x.1994.tb00857.x
- Tüzün EH, Eker L, Aytar A, Daşkapan A, Bayramoğlu M. Acceptability, reliability, validity, and responsiveness of the Turkish version of WOMAC osteoarthritis index. Osteoarthritis Cartilage. 2005;13:28-33. doi:10.1016/j.joca.2004.10.010
- Meijer H, Reinecke J, Becker C, Tholen G, Wehling P. The production of anti-inflammatory cytokines in whole blood by physico-chemical induction. Inflamm Res. 2003;52(10):404-407. doi:10.1007/s00011-003-1197-1
Tables
Table 1. Age and gender

Table 2. Before and after 1 year treatment for left knee
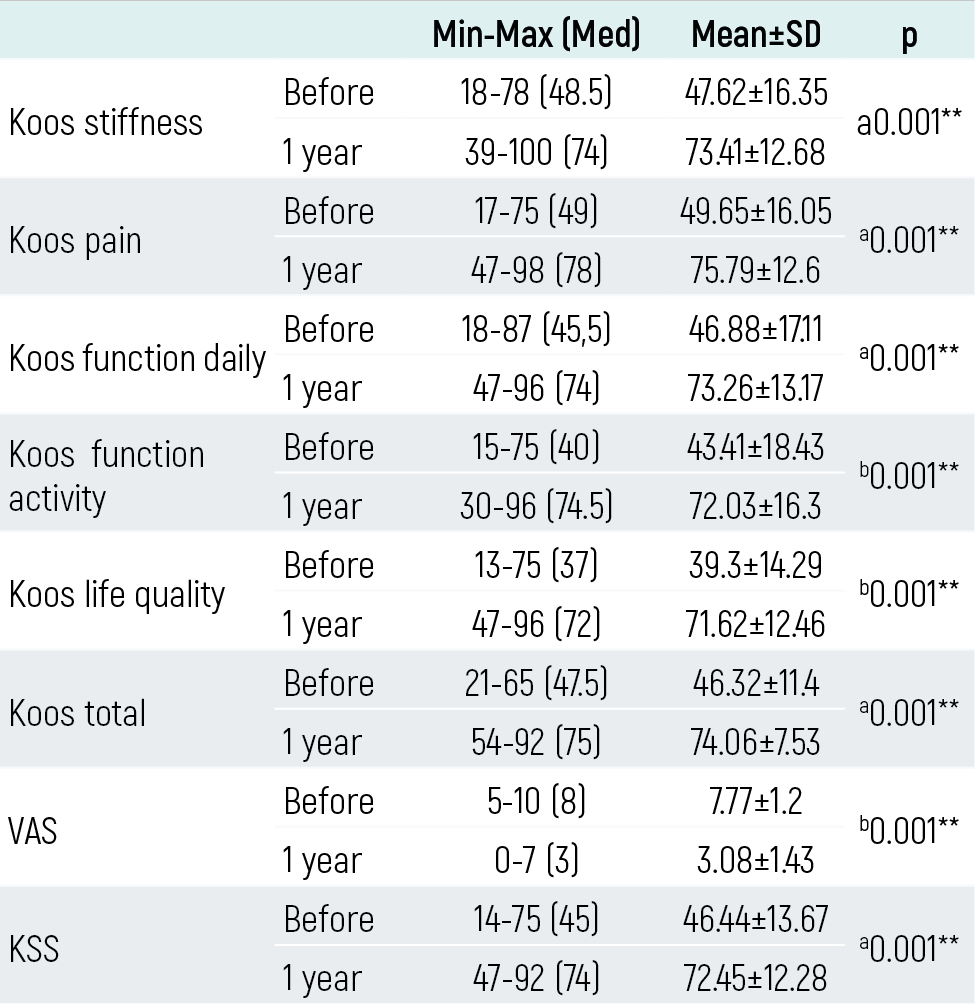
Table 3. Before and after 1 year treatment for right knee

Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Yunus Öç, Bekir Eray Kilinc, Yigit Atalay, Hasan Basri Sezer, Osman Tugrul Eren. Autologous conditioned serum treatment in the knee osteoarthritis. Eu Clin Anal Med 2026;5(1):6-10. doi:10.4328/ECAM.105
- Received:
- 02.02.2017
- Accepted:
- 12.02.2017
- Published Online:
- 01.01.2017
- Printed:
- 01.01.2017