Abstract
AimThe breast tissue in women shows continuous change from birth with the hormonal effect, and various symptoms occur accordingly. Breast diseases are among the most common diseases seen in women and their incidence is continuously increasing.MethodsThe records of patients aged 18 to 75 who were consulted to Ahi Evran University Training and Research Hospital General Surgery Clinic between October 2014-January 2016 and who were pathologically diagnosed with primary breast disease were retrospectively examined. Clinical information was analyzed with SPSS 19.ResultsThe most common patient complaint was breast pain (43 patients). The most commonly encountered benign pathology was fibroadenoma (24 patients). Inflammatory diseases were encountered in 12 patients. 26 patients were diagnosed with malignant breast lesions.ConclusionIn our study, similar to the literature, benign breast diseases formed the most commonly observed group, with a rate of 59.5%. Malign breast diseases formed the second most commonly diagnosed group, with a rate of 27.6%. Inflammatory breast diseases formed the third most commonly diagnosed group, with a rate of 12.7%.
Keywords
Introduction
The breast tissue in women shows continuous change with the hormonal effect beginning at birth, and various symptoms occur accordingly. Breast diseases are among the most common diseases seen in women and their incidence is continuously increasing. More than 200,000 women are diagnosed with breast diseases annually.1 Most of the lesions that occur in the breast are benign. Benign breast diseases generally occur during the reproductive period and are encountered approximately four times more often than breast cancer.2-3 In this study, the frequency of breast diseases identified and the scanning programs used were explored.
Materials and Methods
The records of patients aged 18 to 75 who were consulted to Ahi Evran University Training and Research Hospital General Surgery Clinic between October 2014 and January 2016 with breast-related complaints or under the breast cancer scanning program and who were pathologically diagnosed with primary breast disease (patients on whom needle biopsy, excisional biopsy, segmental mastectomy, or mastectomy were performed) were retrospectively examined. Patients previously diagnosed with breast cancer or a secondary breast disease were excluded from the study.
Complaints of the patients during the consultation, clinical examinations performed, pathological diagnosis, and demographic features were recorded by reviewing the patient files. The post-diagnostic follow-up period of the patients was at least 6 months.After the clinical information for the patients were compiled, it was analyzed with SPSS 19.
Results
Within the 15-month period when the retrospective examination was carried out, 94 patients were pathologically diagnosed with primary breast disease. The mean age of patients was 28.1 years (18-75). The most common complaint of the patients was breast pain (43 patients). The number of patients consulting due to breast lumps was 20, whereas 10 patients consulted with complaints of erythema, ulcer, or lesions. Five patients complained of serohemorrhagic nipple discharge. 16 patients had category 4 or 5 BI-RADS (Breast Imaging Reporting and Data Systems) under the scanning program for patients aged 40 and over (Table 1 Complaints of Patients upon Consultation).With regard to the pathological diagnosis of the breast, the patients were examined in 3 groups: benign lesions, malign lesions, and inflammatory lesions. (As idiopathic granulomatous mastitis and breast cancer were concurrent in only 1 patient, inflammatory lesions are evaluated in a separate group.) These pathological diagnoses and numbers of patients are given in Table 2 (Table 2 Numbers of Patients based on the Pathological Results).
The most commonly encountered benign pathology was fibroadenoma (24 patients). The mean age of patients with fibroadenoma was 23.2 years (18-29 years). As there was size growth and radiological findings with suspicion of malignancy in the lesions of 3 premenopausal patients followed up with a fibroadenoma pre-diagnosis, excisional biopsy was performed and pathological diagnosis was reported as benign phyllodes tumor.Inflammatory diseases were encountered in 12 patients. Among these, 9 patients were diagnosed with granulomatous mastitis and 3 patients were diagnosed with periductal mastitis. Of these, 1 patient had concurrent granulomatous mastitis and invasive ductal carcinoma in the same pathological sampling; modified radical mastectomy was subsequently performed on the patient. 5 patients consulting with serohemorrhagic nipple discharge complaints were diagnosed with intraductal papilloma. 3 patients consulting due to lumps in the axillary area and aesthetic concerns were diagnosed with accessory breast tissue.26 patients were diagnosed with malign breast lesions. Of these, the most commonly diagnosed type was invasive ductal carcinoma.
Discussion
Most of the lesions that occur in the breast are benign. Benign breast diseases are a non-homogenous group that consists of developmental anomalies, epithelial and stromal growth, inflammatory lesions, and neoplasms. They generally occur during the reproductive period. Approximately 55% of females are diagnosed with benign breast disease in their lives.2-3-4-5 The mean age of patients in our study was 28.1 years (18-75) and 76.2% of the patients were under age 40. This rate is similar to the rates in previous studies in the literature related to patients diagnosed with benign breast disease.6-7
Benign breast diseases were the most commonly encountered pathological diagnosis in our study group, with a rate of 59.5%. Of the benign breast diseases, fibroadenoma ranked first with a rate of 42.8%. As they tend to be dependent upon hormonal effects, diagnosis is more commonly made at young ages. Nevertheless, they can be encountered as calcified lesions in scanning mammographies until about age 50. In our study, the mean age of patients with fibroadenoma was 23.2 years (1829). Fibroadenomas made up 25.5% of the patients in the study group.
This rate was found to be lower compared to the previous studies.8-9 The reason for this could be interpreted as performing diagnostic procedures on fibroadenomas with a large size or that bear malignancy risk as assessed by radiological and clinical evaluations. Three of our patients with a fibroadenoma pre-diagnosis were followed up. As there was size growth and radiological findings with suspicion of malignancy in the lesions of these patients, excisional biopsies were performed and pathological diagnoses were reported as benign phyllodes tumors. During the observation of fibroadenomas, biopsy should be considered for growing lumps or lumps with a BI-RADS category 4 suspicion of malignancy.10 While the number of patients diagnosed with fibrocystic disease was 8, it was the second most common benign breast disease. Similar to fibroadenomas, the number of patients in this group was also smaller than in the previously reported studies.11-12 Patients with a fibrocystic disease may have lumps that could not be differentiated from malignancy with clinical findings.13 Simple, complicated, or complex cysts could be encountered in the ultrasonographies of these patients. While the rate of malignancy is below 2% in complicated cysts, this rate is reported to be between 23-31% in complex cysts.13-14 Our patients also were found to have complicated and complex cyst (BRADS 4) pre-diagnoses during breast ultrasonographies performed during the preoperative period. Benign papillary neoplasia form 1-5% of all lesions for which a biopsy is performed on the breast, and represent less than 10% of all benign breast lesions.15 In our study, this rate was less than 1%. Bloody-pathological nipple discharge occurred in almost half of the cases diagnosed with papilloma.16 5 of our patients diagnosed with intraductal papilloma had serohemorrhagic nipple discharge.
Inflammatory diseases of the breast were the third most common disease in our study. Of these, 9 patients were diagnosed with idiopathic granulomatous mastitis, a benign chronic breast disease that may relapse in time. Clinically, it could be focal or diffused, and it sometimes displays inflammatory findings (hyperaemia, pain) that present as lumps such as tumors, and also induration and galactorrhea. It can clinically and radiologically mimic cancer.17-18 Granulomatous mastitis and invasive ductal carcinoma were concurrent in the same pathological sample of one of our patients who was diagnosed with idiopathic granulomatous mastitis. Modified radical mastectomy was performed on our patient following the diagnosis. Only 3 cases in which idiopathic granulomatous mastitis and breast cancer were present concurrently have been presented in the literature.19-20 The important aspect of this case is that ours is the fourth reported case where idiopathic granulomatous mastitis and breast cancer were present concurrently.In our study, malign breast diseases were the second most commonly diagnosed group of diseases, with a rate of 27.6%. This rate is higher compared to the previous studies.21 We are of the opinion that such a high rate of malign breast lesions is due to the early diagnosis in patients thanks to the scanning programs for people over 40 years of age. While the prevalence of breast cancer has increased in years, the mortality rate has dropped thanks to early diagnosis and developments in treatment modalities. As a result of the mammography and scanning activities performed in developed countries, a decrease of up to 35% has been observed in breast cancer mortality in women older than 50 years of age. The decrease in mortality as a result of the scanning is due to finding tumors of a smaller size and the increase in the rate of patients diagnosed during the in situ period (25%).22 In our study, we discussed the pathological diagnosis of patients on whom breast surgery was performed within the 15-month period, in line with the literature. Similar to the literature, benign breast diseases formed the most commonly observed group, with a rate of 59.5%. Among these, fibroadenomas rank the first. Malign breast diseases formed the second most commonly diagnosed group, with a rate of 27.6%. We are of the opinion that such a high rate of malign breast lesions is due to the early diagnosis in patients thanks to the scanning programs for people over 40 years of age. Inflammatory breast diseases formed the third most commonly diagnosed group, with a rate of 12.7%. Within this group, idiopathic granulomatous mastitis was the most common diagnosis, and it is an important fact that one of our patients had concurrent granulomatous mastitis and invasive ductal carcinoma in the same pathological sample, being only the fourth case in the literature reporting this co-occurrence.
All procedures performed in studies involving human participants were in accordance with the ethical standards of Ahi Evran University Ethical Research Committee and the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Declarations
Informed Consent
Informed consent was obtained from all participants included in the study.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
None.
References
- Malik M, Selahuddin O, Azhar M, Dilawar O, Irshad H, Sadia SA. Breast disease spectrum in Wah Cantt: POF Hospital experience. Prof Med J. 2010;17(3):366-372.
- Pearlman MD, Mark D. Benign breast disease. Am J Obstet Gynecol. 2010;116(3):747-758. doi:10.1097/aog.0b013e3181ee9fc7
- Hughes LE. World progress in surgery: benign breast disorders. Introduction—fibrocystic disease? Non disease? or ANDI? World J Surg. 1989;13(6):667-668. doi:10.1007/bf01658411
- Santen RJ, Mansel R. Benign breast disorders. N Engl J Med. 2005;353(3):275-285. doi:10.1056/nejmra035692
- Dupont WD, Parl FF, Hartmann WH, Brinton LA, Winfield AC, Worrell JA, et al. Breast cancer risk associated with proliferative breast disease and atypical hyperplasia. Cancer. 1993;71(4):1258-1265.
- Ihekwaba FN. Benign breast disease in Nigerian women: a study of 657 patients. J R Coll Surg Edinb. 1994;39(5):280-283.
- Chaudhary IA, Qureshi SK, Rasul S, Bano A. Pattern of benign breast diseases. J Surg Pak. 2003;8(3):5-7.
- Adesunkanmi AR, Agbakwuru EA. Benign breast lesions in Wesley Guild Hospital, Ilesha, Nigeria. West Afr J Med. 2001;20(2):146-151.
- Kathcy KC, Datubo-Brown DD, Gogo-Abite M, Iweha UU. Benign breast lesions in Nigerian women in Rivers State. East Afr Med J. 1990;67(3):201-204.
- D’Orsi CJ. Breast imaging reporting and data system (BI-RADS). 4th ed. American College of Radiology; 2003:147.
- Anyikam A, Nzegwu MA, Ozumba BC, Okoye I, Olusina DB. Benign breast lesions in Eastern Nigeria. Saudi Med J. 2008;29(2):241-244. doi:10.15537/1658-3175.4227
- Ali K, Abbas MH, Aslam S, Aslam M, Abid KJ, Khan AZ. Frequency of benign breast diseases in female patients with breast lumps: a study at Sir Ganga Ram Hospital. Ann King Edward Med Coll. 2005;11(4):526-528.
- Berg WA, Campassi CI, Ioffe OB. Cystic lesions of the breast: sonographic-pathologic correlation. Radiology. 2003;227(1):183-191. doi:10.1148/radiol.2272020660
- Doshi DJ, March DE, Crisi GM, Coughlin BF. Complex cystic breast masses: diagnostic approach and imaging-pathologic correlation. Radiographics. 2007;27(suppl 1):S53-S64. doi:10.1148/rg.27si075508
- Mulligan AM, O’Malley FP. Papillary lesions of the breast. Adv Anat Pathol. 2007;14(2):108-119. doi:10.1097/pap.0b013e318032508d
- Al-Sarakbi W, Worku D, Escobar PF, Mokbel K. Breast papillomas: current management with a focus on a new diagnostic and therapeutic modality. Int Semin Surg Oncol. 2006;3(1):1-8.
- Kuba S, Yamaguchi J, Ohtani H, Shimokawa I, Maeda S, Kanematsu T. Vacuum-assisted biopsy and steroid therapy for granulomatous lobular mastitis: report of three cases. Surg Today. 2009;39(8):695-699. doi:10.1007/s00595-008-3891-7
- Azlina AF, Ariza Z, Arni T, Hisham AN. Chronic granulomatous mastitis: diagnostic and therapeutic considerations. World J Surg. 2003;27(5):515-518. doi:10.1007/s00268-003-6806-1
- Limaiem F, Khadhar A, Hassan F, et al. Coexistence of lobular granulomatous mastitis and ductal carcinoma: a fortuitous association? Pathologica. 2013;105(6):357-360.
- Luqman M, Niza ASS, Jaszle JS, et al. Breast carcinoma occurring from chronic granulomatous mastitis. Malays J Med Sci. 2012;19(2):82-85.
- Aslam HMA, Saleem S, Shaikh HA, Shahid N, Mughal A, Umah R. Clinico-pathological profile of patients with breast disease. Diagn Pathol. 2013;8(1):77. doi:10.1186/1746-1596-8-77
- Anderson TJ, Lamb J, Donnan P, Alexander FE, Huggins A, Muir BB, et al. Comparative pathology of breast cancer in a randomized trial of screening. Br J Cancer. 1991;64(1):108-113. doi:10.1038/bjc.1991.251
Tables
Table 1. Complaints of the patients on consultation
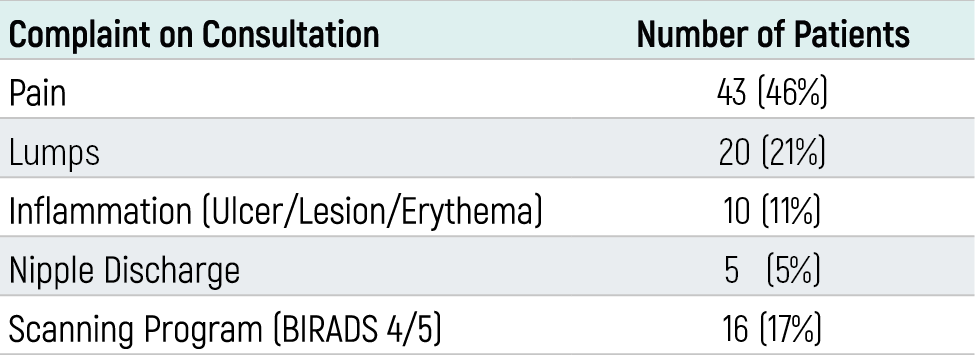
Table 2. Numbers of Patients based on the Pathological Results

Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Hasan Calis, Nuraydin Ozlem. Clinicopathologic features of breast diseases in a clinic. Eu Clin Anal Med 2026;5(2):28-31. doi:10.4328/ECAM.110
- Received:
- 29.03.2017
- Accepted:
- 24.04.2017
- Published Online:
- 01.05.2017
- Printed:
- 01.05.2017