Abstract
AimThe extension of spinal anesthesia by extradural injection has been identified as a modification of the combined spinal-epidural anesthesia. Epidural volume extension (EVE) is a rescue strategy that can raise the level of insufficient post-spinal sensory block.MethodsAfter approval of Adnan Menderes University Ethics Committee (Decision 2016/834/37), the data of 455 patients who had undergone insufficient simultaneous combined spinal epidural without catheter between 2010 and 2016 were retrospectively analyzed in terms of ASA scores; demographic and hemodynamic data; surgery type; preoperative and postoperative sensory and motor block levels; operation onset times after anesthesia; need for peroperative additional anesthesia, vasopressor (ephedrine) and atropine; and postoperative pain onset times.ResultsOf the 455 patients, there were two groups. In the first group, there were 238 patients who had undergone cesarean section and in the second group there were 217 patients who had undergone surgery for inguinal hernia. There was no mortality and morbidity in any group. There was a statistically significant decrease in heart rate, systolic, diastolic, and mean arterial pressures during the peroperative period in both groups (p<0.05).ConclusionThe simultaneous combined spinal-epidural technique (sCSEA) without catheter may be considered as an alternative to conventional methods for appropriate surgeries. It can be safely used with local anesthetic combinations instead of saline for EVE. The advantages and disadvantages of EVE compared to the conventional method should be demonstrated with clinical randomized studies.
Keywords
Introduction
Combined spinal-epidural anesthesia (CSEA) was first described by Brownridge 36 years ago.1 In 1982, the needle-through-needle technique, which has become the standard nowadays for CSEA, was introduced into clinical practice by Coates.2 CSEA has become a suitable neuroaxial technique for urological, gynecological, and lower extremity surgeries and caesarean sections. CSEA offers the advantage of a rapid onset of anesthesia provided via the spinal route and can also provide postoperative analgesia via an epidural catheter.3 Later, extension of spinal anesthesia by extradural injection was identified as a modification of CSEA by Blumgart et al.4 and became known as epidural volume extension (EVE). EVE means injecting normal saline into the epidural space after the subarachnoid block, which aims to rapidly increase the sensory block level resulting from intrathecal local anesthetic injection.4-5 EVE is a rescue strategy that can raise the level of insufficient post-spinal sensory block. In this study, we conducted a retrospective evaluation of cases that had been performed with local anesthesia at low dose with spinal and epidurals simultaneously, which we defined as sequential CSEA without catheter aspiration by EVE mechanism.
Materials and Methods
After approval of the Adnan Menderes University Ethics Committee (Decision 2016/834/37), the data of 455 patients who had undergone insufficient simultaneous combined spinal epidural without catheter between 2010 and 2016, was analyzed retrospectively in terms of ASA scores; demographic and hemodynamic data; surgery type; preoperative and postoperative sensory and motor block levels; operation onset times after anesthesia; need for peroperative additional anesthesia, vasopressor (ephedrine) and atropine; and postoperative pain onset times.Simultaneous Combined Spinal Epidural Technique Without Catheter(sCSEA)In this method, a simultaneous combined spinal-epidural kit without catheter, with 18G epidural and 27G spinal needles (suitable needles for the needle-through-needle technique), may be preferred. In the application of sCSEA, the appropriate interval is marked by examination. After skin sterilization and covering, a local anesthetic substance is applied by a 18G epidural needle, finding the epidural space with pressure loss or with the hanging drop technique. Subsequently, 2 ml of 40 mg lidocaine and 1:200.000 adrenaline are applied from the epidural needle as a test dose. If the test is negative, the 27G pencil point spinal needle is pushed forward into the intrathecal space following dural puncture by the needle-through-needle technique. After CSF is seen, bupivacaine is administered intrathecally at calculated dose according to patient length and the operation to be performed. Then the spinal needle is removed. If there is no liquid resembling CSF coming from the epidural needle, the combination of bupivacaine, lidocaine, and morphine, the dose and volume calculated according to the patient’s length and operation, is applied into the epidural space. Then the pinprick test and Bromage are checked and surgery is started. The spinal and epidural
doses and volumes that can be applied according to the surgery type and patient length are shown in Table 1.Statistical AnalysisDemographic data, ASA, surgery, peroperative supplemental anesthesia requirement, and vasopressor (ephedrine) requirement were compared using x2 and Fisher exact tests. One-way variance analysis (ANOVA) for multiple comparisons and post-hoc Bonferroni tests for nominal values were used and Kruskal-Wallis analysis was performed for ordinal data. A p value smaller than 0.05 was considered as statistically significant.
Results
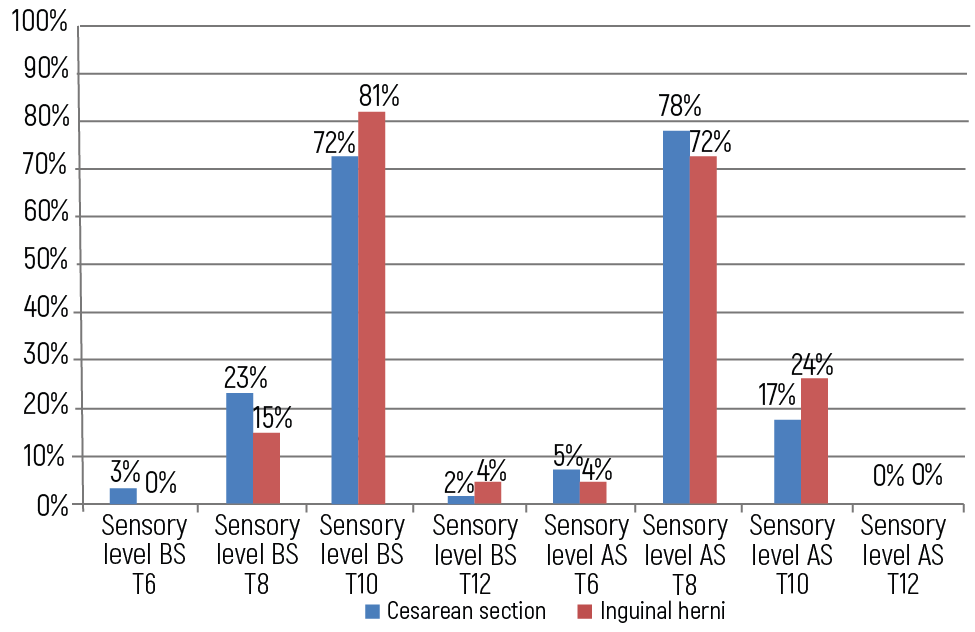
Of the 455 patients, there were two groups. In the first group, there were 238 patients who underwent cesarean section, and in the second group there were 217 patients who underwent surgery for inguinal hernia. There was no mortality and morbidity in either group. There was a statistically significant decrease in heart rate, systolic, diastolic, and mean arterial pressures during the peroperative period in both groups (p<0.05). The need for peroperative anesthesia, vasopressor (ephedrine), and atropine in cesarean and inguinal hernia operations are shown in Table 2; sensory levels before and after surgery are shown in Table 3; pre- and post-surgery Bromage levels are shown in Table 4. Postoperative pain initiation times were 14±4 hours in cesarean patients and 16±2 hours in inguinal hernia operations. The mean operation onset times after anesthesia were 300 ± 83 s in the cesarean section group and 240 ± 75 s in the inguinal hernia group.
Discussion
Opinions regarding the impact of EVE vary. Studies advocating the effect of EVE have compared saline volumes with analgesia durations affecting motor and sensory levels.5-6-7-8-9
Lew et al.10 achieved satisfactory anesthesia in only 55% of patients using the EVE method when performing cesarean sections. They attributed this finding to the fast ending of the motor block. In our cases, we found the rate of satisfactory anesthesia was 77% in cesarean patients. We believe this difference was due to the use of spinal low-dose isobaric bupivacaine as a local anesthetic instead of epidural saline.
Loubert et al.11 reported that they did not find any benefit to using EVE with 5 ml saline in caesarean section patients. Lin et al.’s letter.12 criticized Loubert et al.’s study because of the inadequacy of the epidural volume. Lin et al. suggest at least 10 ml of epidural saline. Takiguchi et al.7 and Dogancı et al.13 suggest 10-15 and 20 ml of epidural saline for EVE.
In EVE, there are studies suggesting the block level is time-dependent and it has been determined that the average block resistance time is 12 minutes.14 In our cases, this period was shorter. We believe that the combination of epidural local anesthetic and opioid is beneficial in reducing both spinal and epidural doses, and that this therefore reduces the likelihood of complications associated with spinal and epidural anesthesia.
Stienstra et al.15 attribute the epidural top-up effect of the increased spinal block level to the effect of epidural volume. It is obvious that epidural bupivacaine, morphine, and saline increase the spinal anesthesia level due to epidural volume effect in sCSEA.
In conclusion, the sCSEA technique may be considered as an alternative to conventional methods for appropriate surgeries. It also can be safely used with local anesthetic combinations instead of saline for EVE. Advantages and disadvantages of EVE compared to the conventional method should be demonstrated with clinical randomized studies.AcknowledgmentWe thank Serpil Demirag for her contributions and comments and Sylvia M. Bozdogan for her contributions to editing the English.
Declarations
Informed Consent
Due to the retrospective nature of the study, informed consent was waived by the ethics committee.
Conflict of Interest
The author declares no conflicts of interest.
Funding
None.
References
- Brownridge P. Epidural and subarachnoid analgesia for elective caesarean section. Anaesthesia. 1981;36:70. doi:10.1111/j.1365-2044.1981.tb08614.x
- Coates MB. Combined subarachnoid and epidural techniques. Anaesthesia. 1982;37:89-90. doi:10.1111/j.1365-2044.1982.tb01016.x
- Heesen M, Weibel S, Klimek M, et al. Effects of epidural volume extension by saline injection on the efficacy and safety of intrathecal local anaesthetics: systematic review with meta-analysis, meta-regression and trial sequential analysis. Anaesthesia. 2017;72(11):1398-1411. doi:10.1111/anae.14033
- Blumgart CH, Ryall D, Dennison B, Thomson-Hill LM. Mechanism of extension of spinal anesthesia by extradural injection of local anaesthetic. Br J Anaesth. 1992;69:457-460. doi:10.1093/bja/69.5.457
- Stienstra R, Dilrosun-Alhadi BZ, Dahan A, van Kleef JW, Veering BT, Burm AG. The epidural “top-up” in combined spinal-epidural anesthesia: the effect of volume versus dose. Anesth Analg. 1999;88:810-814. doi:10.1097/00000539-199904000-00024
- Choi DH, Park NK, Cho HS, Hahm TS, Chung IS. Effects of epidural injection on spinal block during combined spinal and epidural anaesthesia for cesarean delivery. Reg Anesth Pain Med. 2000;25:591-595. doi:10.1053/rapm.2000.8934
- Takiguchi T, Okano T, Egawa H, et al. The effect of epidural saline injection on analgesic level during combined spinal and epidural anaesthesia assessed clinically and myelographically. Anesth Analg. 1997;85:1097-1100. doi:10.1097/00000539-199711000-00024
- Trautman WJ, Liu SS, Kopacz DJ. Comparison of lidocaine and saline for epidural top-up during combined spinal-epidural anaesthesia in volunteers. Anesth Analg. 1997;84:574-577. doi:10.1097/00000539-199703000-00020
- Yamazaki Y, Mimura M, Hazama K, Namiki A. Reinforcement of spinal anaesthesia by epidural injection of saline: a comparison of hyperbaric and isobaric tetracaine. J Anesth. 2000;14:73-76. doi:10.1007/s005400050070
- Lew E, Yeo SW, Thomas E. Combined spinal-epidural anaesthesia using epidural volume extension leads to faster motor recovery after elective cesarean delivery: a prospective, randomized, double-blind study. Anesth Analg. 2004;98:810-814. doi:10.1213/01.ane.0000101987.79454.bc
- Loubert C, O’Brien PJ, Fernando R, et al. Epidural volume extension in combined spinal epidural anaesthesia for elective caesarean section: a randomized controlled trial. Anaesthesia. 2011;66:341-347. doi:10.1111/j.1365-2044.2011.06662.x
- Lin X, Wu L, Zhou J. Epidural volume extension in combined spinal-epidural anaesthesia. Anaesthesia. 2012;67:927-928. doi:10.1111/j.1365-2044.2012.07244.x
- Doganci N, Apan A, Tekin O, Kaymak C. Epidural volume expansion: is there a ceiling effect? Minerva Anestesiol. 2010;76:334-339.
- Mardirosoff C, Dumont L, Lemédioni P, Pauwels P, Massaut J. Sensory block extension during combined spinal and epidural anesthesia. Reg Anesth Pain Med. 1998;23:92-95. doi:10.1016/s1098-7339(98)90117-1
- Stienstra R, Dahan A, Alhadi BZ, van Kleef JW, Burm AG. Mechanism of action of an epidural top-up in combined spinal epidural anesthesia. Anesth Analg. 1996;83:382-386. doi:10.1097/00000539-199608000-00031
Tables
Table 1. Spinal and epidural doses and volumes were evaluated for the simultaneous combined spinal epidural anesthesia technique without catheter (sCSEA).
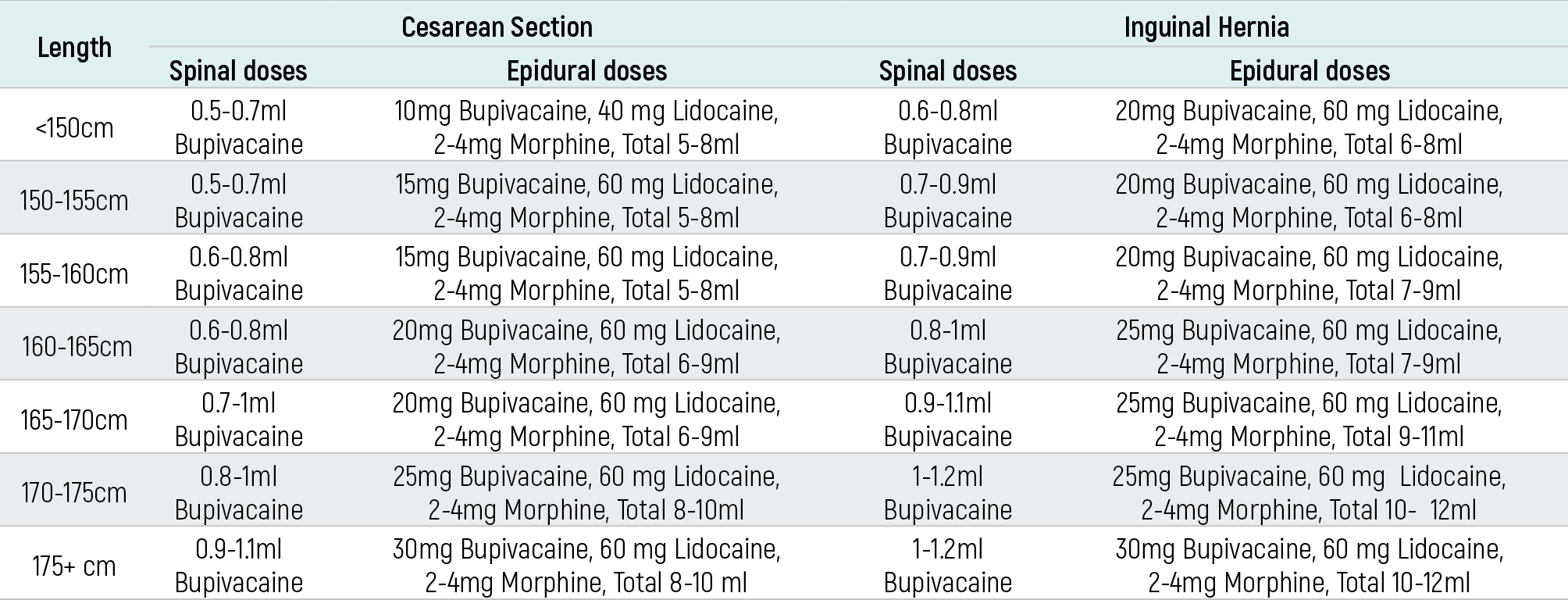
Table 2. Need for additional anesthesia, ephedrine, and atropine in peroperative period

Table 3. Bromage levels

Table 4. Sensory levels
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Kamil Varlık Erel. Simultaneous combined spinal epidural anesthesia technique without catheter. Eu Clin Anal Med 2026;6(2):22-24. doi:10.4328/ECAM.128
- Received:
- 13.03.2018
- Accepted:
- 28.03.2018
- Published Online:
- 04.02.2018
- Printed:
- 01.05.2018