Abstract
IntroductionCongenital diaphragmatic hernia is a progression into chest of abdominal organs depends on diaphragmatic defect during fetal development. Prevalence is 1/2500-3000 of live births. Case PresentationThe most common seen hernia is Bochdalek (90%). In this presentation, late congenital diaphragmatic hernia is described in a patient treatment and follow-up process. Congenital diaphragmatic hernia is a congenital malformation manifested by diaphragmatic hernia, pulmonary hypoplasia and abdominal organ changes. The most common accepted theory of etiology is a problem in the closure of pleuroperitoneal canal. Left-sided hernias which are seen after puberty is rare. Our case is one of them. ConclusionIn conclusion, although the frequency of late congenital diaphragmatic hernia is 0.17–12%, it is a clinical situation that may be encountered in intensive care practice. It must therefore be kept in mind.
Keywords
Introduction
Congenital diaphragmatic hernia is a progression of abdominal organs into chest depends on diaphramatic defect during fetal development. It was described firstly by Victor Alexander Bochdalek in 1867.1 It is a rare malformation of lung and incidence is 1 / 2500-3000 in live births. It is mostly characterized by cardiac and respiratory symptoms in neonatal period. However, some of them may remain asymptomatic until adulthood. Prevalence of diaphragmatic hernia identified in adult is 0.17-12% as approximately.2 Bochdalek hernia is the most frequent form which 90% of them is located posterolateral. However, Morgagni hernia (1-5%) and esophageal hernia (1-5%) can be seen. Late period Bochdalek hernias are usually right-sided, left sided ones are rare.3-4 In this study, surgical treatment and postoperative intensive care process are shared in a rare case of late congenital diaphragmatic hernia.
Discussion
Congenital diaphragmatic hernia is a congenital malformation manifested with trio of diaphragmatic hernia, pulmonary hypoplasia and displacement of abdominal organs. Although there are several theories on the etiology, the most widely accepted theory is problem of the closure of pleuroperitoneal channel.5 It is usually in the form of Bochdalek hernia and lef sided display. However the delayed emergence of Bochdalek hernia occurs with defect from right side generally due to the effect of closing the liver. The existence of liver at right side allows the partial closure of defect. Left sided hernias after puberty are rare.4 Our case is one of these rare group.14% of congenital diaphragmatic hernia was asymptomatic, in symptomatic patients chest pain (69%), intestinal obstruction (39%) and pulmonary symptoms (wheezing, recurrent pneumonia, dyspnea, cough) (37%) are most common symptoms observed. Some factors such as chronic constipation, strong straining, severe cough, physical exertion, strenuous exercise, trauma and pregnancy could cause to become symptomatic or asymptomatic cases.6 On physical examination, respiratory distress, absence of breath sounds in herniation zone, bowel sounds in lung fieds and displacement of heart sounds are guiding. In our case, there were all physical findings indicated. To diagnosis, respectively, chest and abdominal x-ray, barium enema, thoracic computer tomography (most common) magnetic resonance, ultrasound, laparoscopy/laparotomy (used in advanced stage) are used.7 In our case, diagnosis was made by physical examination, chest x-ray and thoracic computer tomography.In bochdalek hernia, left hernia sac has mostly omentum and retroperitoneal structures. intestine, spleen, liveri pancreas nd kidneys can be found. Colon containing hernias are rare.4 In our case, most of abdominal organs including most of small intestine, ascending colon, cecum and appendix is located on left hemithorax. Surgery should be planned without delay especially when large hernias accompained abdominal organs are seen due to high risk of complications.8 The main aims of surgery are to place herniated organs to abdomen, to open hernia sac, and to close defect of diaphragm. For this purpose, thoracotomy, thoracoscopy, laparotomy, laparoscopy and if necessary a combination of these methods can be applied.9-10 In our case, operation began with thoracotomy but laparotomy was included in operation with general surgery team due to large amount of abdominal organs and they could not be placed in the abdomen. Intra-abdominal hypertension, can be seen in patients with intra-abdominal pressure rises above 12 mmHg.11 Our patient intra-abdominal pressure is measured as 14 mmHg, entering Grade 1 Group according to the 2013 Consensus Statement of the Abdominal Compartment Society (WSACS),11 Postoperative follow-up is required to be done carefully to avoid this situation included renal, cardiac, pulmonary and inflammtory complications. In our case management, especially we cared about the lungs of peak inspiratory pressure monitoring during mechanical ventilation to the expansion, the provision of adequate analgesia, bowel sounds and gas - if necessary by following the stool out made the gastric decompression, urine output monitoring and abdominal pressure measuring. In these cases, the postoperative intensive care unit stay varies depending on factors such as patient age, comorbidities, postoperative complications, the presence of pulmonary hypoplasia. In the postoperative period, patient should be intubated while monitored to facilitate lung expansion. However, there is no study on how much it should be the optimum time. This period shall be determined in accordance with clinical follow-up of intensive care physicians considering the factors mentioned above. Time should be kept as short as possible in terms of ventilator-associated pneumonia.12 In our case, due to young patient, lack of co-morbid condition and the development of postoperative complications, sufficient to ensure early detection of lung expansion, after 24 hours postoperatively extubation was deemed appropriate. There is no clear information about the selection of mechanical ventilation in the postoperative follow-up which mechanical ventilation mode or used in non-invasive post-extubation. In these cases, keeping in the forefront of lung protective strategy, respiratory mechanics should remain within physiological limits.12 Consequently; Late congenital diaphragmatic hernia is a featured clinical condition due to the possibility of intra-abdominal hypertension in the postoperative period. In these cases, early diagnosis is important for prevention of the development of lung hypoplasia. As it was in our case, we believe that avoidance of positive fluid overlod at surgery the only option for treatment and intensive care follow up and prevention of intra-abdominal hypertension benefiting from treatment guidelines of WSAC are quite significant for morbidity and mortality.
Declarations
Informed Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
None.
References
- Bochdalek VA. Ueber den Peritonealueberzug der Milz und das Ligamentum pleurocolicum: Beitrag zur Anatomie des Bauchfells. Arch Anat Physiol Wiss Med. 1867:565-614.
- Mullins ME, Stein J, Saini SS, Mueller PR. Prevalence of incidental Bochdalek’s hernia in a large adult population. AJR Am J Roentgenol. 2001;177:363-366. doi:10.2214/ajr.177.2.1770363
- Demirkaya A, Kaynak K. Bochdalek hernisinde tanı ve cerrahi tedavi. J Thorac Surg Spec Top. 2010;3(1):18-22.
- Yetim TD, Yetim I, Karcıoğlu M, Davran R, Canbolant E. Congenital diaphragmatic hernia late period: a rare case report. Tıp Araştırmaları Derg. 2013;11(1):28-31.
- Allan DW, Greer JJ. Pathogenesis of nitrofen-induced congenital diaphragmatic hernia in fetal rats. J Appl Physiol. 1997;83:338-347. doi:10.1152/jappl.1997.83.2.338
- Brown SR, Horton JD, Trivette E, Hofmann LJ, Johnson JM. Bochdalek hernia in the adult: demographics, presentation, and surgical management. Hernia. 2011;15:23-30. doi:10.1007/s10029-010-0699-3
- Eren S, Ciriş F. Diaphragmatic hernia: diagnostic approaches with review of the literature. Eur J Radiol. 2005;54:448-459. doi:10.1016/j.ejrad.2004.09.008
- Kholdebarin R, Iwasiow BM, Keijzer R. Pulmonary development considerations in the surgical management of congenital diaphragmatic hernia. Early Hum Dev. 2011;87:755-758. doi:10.1016/j.earlhumdev.2011.08.017
- Döngel İ, Duman L, Yazkan R, Camaş HE, Bülbül M. Geç bulgu veren Bochdalek hernisinde cerrahi tedavi ve sonrası: olgu sunumu. Respir Case Rep. 2013;2(3):121-125.
- John PH, Thanakumar J, Krishnan A. Reduced port laparoscopic repair of Bochdalek hernia in an adult: a first report. J Minim Access Surg. 2012;8(4):158-160. doi:10.4103/0972-9941.103131
- Kirkpatrick AW, Roberts DJ, De Waele J, et al. Intra-abdominal hypertension and the abdominal compartment syndrome: updated consensus definitions and clinical practice guidelines from the World Society of the Abdominal Compartment Syndrome. Intensive Care Med. 2014;39:1190-1206.
- Bacakoğlu F. Mekanik ventilasyona bağlı akciğer hasarı. Toraks Derg. 2002;3(2):207-212.
Figures
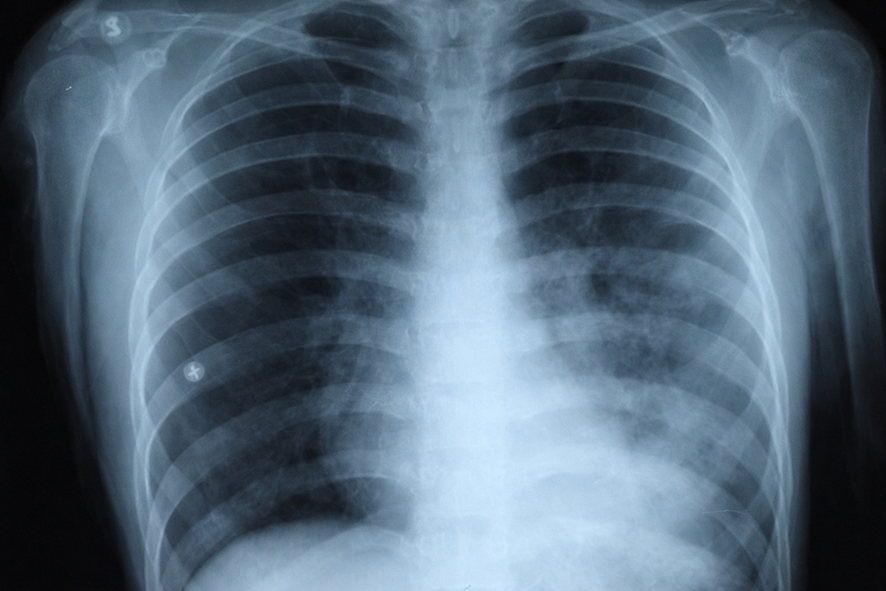
Figure 1. Preoperative patient’s chest x-ray. On the left side of the chest the abdominal contents are observed.

Figure 2. Preoperative computed tomography scan of case

Figure 3. Postoperative chest radiograph on the first day
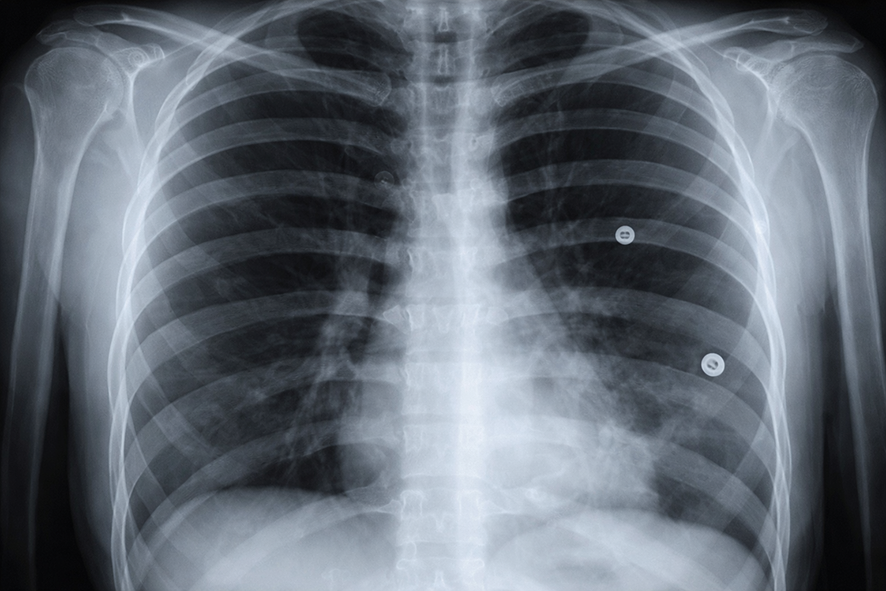
Figure 4. The pre-discharge control chest x-ray of case
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Deniz Erdem, Pakize Özçiftci Yılmaz, Belgin Akan, Özgür Karakurt, Işıl Özkoçak Turan. Late congenital diaphragmatic hernia: A Case Report. Eu Clin Anal Med 2026;4(2):43-46. doi:10.4328/ECAM.65
- Received:
- 03.11.2015
- Accepted:
- 07.11.2015
- Published Online:
- 01.05.2016
- Printed:
- 01.05.2016