Abstract
IntroductionForeign body injuries are common injuries and foreign body penetrations may occur in almost any part of the body. Case PresentationIn the literature there are many reports including different kinds of piercing or penetrating injuries of the extremities. In this paper we report the case of a 19-year-old man who presented with a knife retained in the forearm and our treatment strategy for removing the knife. ConclusionWe informed our patient and took the consent form before the submission for publication.
Keywords
Introduction
Foreign body penetrations are common injuries and may occur in almost any part of the body.1-2 Nearly half of the penetrating traumas are penetrating injuries to the extremities. Penetrating injuries of extremities are commonly seen in the accident and emergency departments and they are excessively associated with peripheral nerve and arterial injuries.3-4 They are less common injuries in West European countries. In these countries the low incidence makes it difficult to gain experience for the trauma surgeons.2 So as not to miss such
common injuries as it can lead to drastic consequences, physicians should be more careful at the examination and treatments of such wounds. We report the case of a 19-year-old man who was assaulted and stabbed in his right forearm.
Discussion
Foreign body penetrations are common injuries and may occur in almost any part of the body.1-2 Penetrating trauma of upper extremities are considered as difficult injuries to manage because vascular and nerve injuries are serious and may lead to catastrophic damages impairing the patient outcome.4-5 In common practice for the treatment of this deeper penetrating injuries routine emergent exploration was performed causing a large number of iatrogenic injuries and unnecessary extremity explorations.6 Some authors support the idea of elective non-operative management favorable for the management of penetrating injuries of the upper extremities.2 In this case, we didn’t attempt to remove the knife at the emergency department so as not to cause neurovascular damage and to avoid unnecessary morbidity we performed slight dissection into the knife tract. To ensure the best outcome the phsycians must perform an accurate, rapid and detailed examination for all injured extremities exploring vascular, nerve, and muscular injury. In the literature for the penetrating injury of upper extremities, eurovascular deficit and osseos penetration were reported.7-8 Our case was not complicated with neurovascular deficits or fructure of the forearm. We advocated the treatment strategy of remove foreign body, irrigate its tract, provide systemic antibiotics keeping with the guidelines used for any retained foreign body.9-10 Postoperatively we checked the neurological examination and no deficit was detected. At the follow up period we didn’t encounter any complications like late neurologic deficit or wound infection. After 2 weeks the patient returned his previous activity levels. In this paper we wanted to emphasize the importance of rapid and controlled intervention for the penetrating injuries of the upper extremities.
Conclusion
In penetrating injuries of extremities such as stabbing not to miss neurovascular injuries the physians must perform an accurate, rapid and detailed examination. We think foreign body removal should be performed not at the emergeny rooms but at the operation theatres with anestesia and detailed dissection is critical to prevent iatrogenic injuries.
Declarations
Informed Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
References
- Van Waes OJ, Cheriex KC, Navsaria PH, van Riet PA, Nicol AJ, Vermeulen J. Management of penetrating neck injuries. Br J Surg. 2012;99:149-154.
- Van Waes OJ, Navsaria PH, Verschuren RC, Vroon LC, Van Lieshout EM, Halm JA, Nicol AJ, Vermeulen J. Management of penetrating injuries of the upper extremities. Ulus Travma Acil Cerrahi Derg. 2013;19(5):405-410. doi:10.5505/tjtes.2013.08684
- Dragas M, Davidovic L, Kostic D, Markovic M, Pejkic S, Ille T, Ilic N, Koncar I. Upper extremity arterial injuries: factors influencing treatment outcome. Injury. 2009;40(8):815-819. doi:10.1016/j.injury.2008.08.012
- Manthey DE, Nicks BA. Penetrating trauma to the extremity. J Emerg Med. 2008;34:187-193. doi:10.1016/j.jemermed.2007.03.038
- Zellweger R, Hess F, Nicol A, Omoshoro-Jones J, Kahn D, Navsaria P. An analysis of 124 surgically managed brachial artery injuries. Am J Surg. 2004;188:240-245. doi:10.1016/j.amjsurg.2004.02.005
- Doody O, Given MF, Lyon SM. Extremities: indications and techniques for treatment of extremity vascular injuries. Injury. 2008;39:1295-1303. doi:10.1016/j.injury.2008.02.043
- Abboud JA, Wiesel B, Tomlinson D, Ramsey M. Intraosseous stab wound to the arm. Am J Orthop. 2008;37(3):52-54.
- Sunderamoorthy D, Chaudhury M. An uncommon peripheral nerve injury after penetrating injury of the forearm: the importance of clinical examination. Emerg Med J. 2003;20(6):565-566. doi:10.1136/emj.20.6.565
- Grobbelaar A, Knottenbelt JD. Retained knife blades in stab wounds of the face: is simple withdrawal safe? Injury. 1991;22(1):29-31. doi:10.1016/0020-1383(91)90156-9
- Greene MW, Hackney FL, Nishioka GJ, Triplitt RG. Fractured knife blade—an incidental finding. Oral Surg Oral Med Oral Pathol. 1991;72(6):758-759. doi:10.1016/0030-4220(91)90024-7
Figures
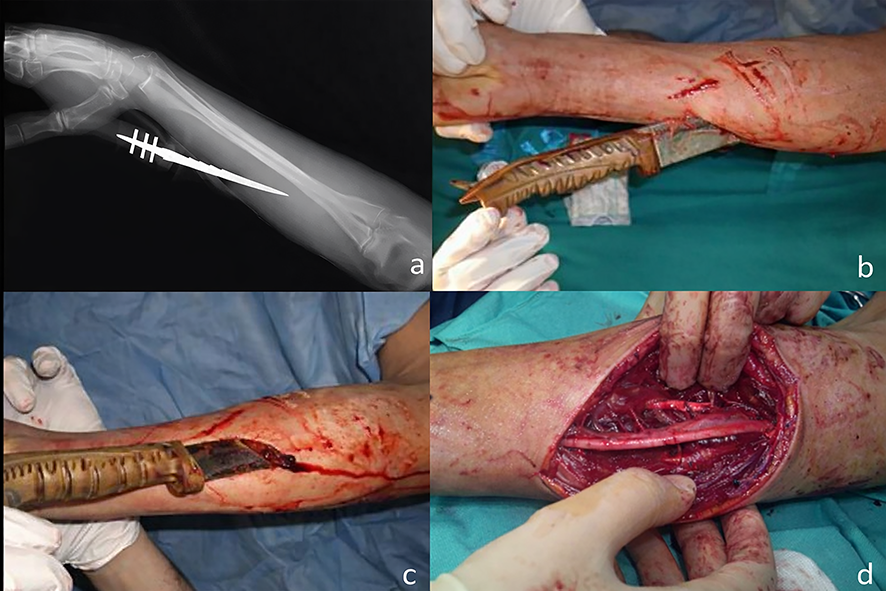
Figure 1. The knife was spanned in a posterolateral direction(a), it penetrated approximately 6 cm into the forearm(b), and didn’t exit the body without any osseos penetration(c), The knife had entered the forearm through the fleksor muscles near to the median nerve and away from the radial and ulnar neurovascular bundle(d).
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Kaan Gürbüz, Erdal Uzun, Alper Çıraklı, Fırat Ozan, Fuat Duygulu. Stabbing injury of the forearm: A Case Report. Eu Clin Anal Med 2026;4(2):62-64. doi:10.4328/ECAM.83
- Received:
- 10.03.2016
- Accepted:
- 19.03.2016
- Published Online:
- 01.05.2016
- Printed:
- 01.05.2016