Abstract
AimAlthough bone tumors are rare they are complex in terms of diagnosis, patient monitoring, and treatment plans. We aimed to determine the properties, frequency, and distribution of bone tumors in a group of adults.MethodsThe histopathology reports of all bone samples of the adults that were recorded in a private pathology laboratory in Istanbul between 2009 and 2015 were reviewed.ResultsThere was a total of 78 patients, 44 male (56%) and 34 (44%) female. The average age was 42.46 years. 47 lesions (60.25%) were benign, 31 (39.75%) malignant. The lesions were most common in the lower extremities (44 cases, 56.4%) and secondly in the upper extremities (17 cases, 22%). Osteochondroma (16 cases, 34%), simple bone cysts (7 cases, 16%), and enchondroma (6 cases, 13%) were the most frequent benign lesions. 20 of 31 malignant lesions were metastasis, followed by chondrosarcoma (5 cases, 6.25%) and chondroblastic osteosarcoma (2 cases, 2.5%). 35% of the metastases were from lung cancer and 19% were from renal cell cancer. 67% of the metastatic lesions were in males.ConclusionKnowledge of the properties and diseases related to adult bone tumors is extremely important. Because they are so rare, the diagnosis may be delayed, causing significant morbidity and mortality.
Keywords
Introduction
Bone tumors can be seen at any age and may be located in any region of the musculoskeletal system, in bone, cartilage, fibrous tissue, bone marrow, lymphoid tissue, nerves, or blood vessels. The primary malignant bone tumor incidence is about 9 in 1 million people in a year; they are responsible for 0.2–0.5% of all malignancies in all ages.1 Also, the rate is higher in males than females (10/million/year vs. 8/million/year).2 Europe and the USA have the highest rates, while Asian countries have lower incidence and prevalence.3 Because of significant differences in anatomic location and clinical presentations, the diagnosis and treatment of bone tumors is difficult. Diagnosis is delayed because these neoplasms are uncommon and patients admit without specific signs and symptoms. At the same time, they can damage the normal tissue, can cause severe pain, swelling, and disability with pathological fractures, and can seriously increase morbidity.4,5
The biopsy is extremely important in terms of diagnosis and treatment.6,7 Because limb salvage surgery is most desirable, fine needle aspiration or open biopsies are required and must be performed in experienced centers.8 The maximum diagnostic value of closed biopsy is 80%.9 Sometimes, to get enough tissue samples, open biopsy is more valuable in leading to diagnosis and treatment. This study aimed to determine the bone tumors in adults and their frequency and distribution.
Materials and Methods
In a private pathology laboratory in Istanbul, the histopathology reports belonging to 78 patients between 2009 and 2015 years were studied. Permission of the private laboratory and hospitals ethics committee consent were obtained. The samples were analyzed with SPSS 15 Statistical Software Package.
Results
There was a total of 78 patients in the study group, 44 male (56%) and 34 (44%) female. The average age was 42.46 years. Males had a mean age of 41.79 years (range 16-79). The mean age of women was 43.27 years (range 16-82). 47 lesions (60.25%) were benign and 31 (39.75%) were malignant (Table 1). While benign lesions were found most commonly in men and women in the age range of 16-30 years, malignant lesions were most often seen in men between 60-70 years of age and in women from 30-40 and 50-60 years (Table 2).
When anatomical sites were evaluated, the most common site involved was in lower extremities (44 cases, 56.4%), secondly in upper extremities (17 cases, 22%). Other areas were in the scalp, ribs, scapula, and especially the thoracic vertebrae (Table 3).
Of the benign lesions observed, the most common was osteochondroma (16 cases, 20.5%), second was simple bone cysts (7 cases, 10.55%), and then enchondroma (6 cases, 7.7%) (Table 4). 20 of the 31 malignant cases were metastasis (25% of all cases). Chondrosarcoma came next in frequency after metastasis (5 cases, 6.25%), and third in incidence was chondroblastic osteosarcoma (2 cases, 2.5%) (Table 4).
35% of the metastases were from lung cancer and 19% were from renal cell cancer. 67% of the metastatic lesions were detected in males. The most commonly involved places were the lower extremities (21 cases), especially the femur (10 cases) and the thoracic spine (5 cases).
Discussion
In the present study, there was a total of 78 patients, 56% male and 44% female. The average age was 41.79 years for men and 43.27 years for women. 60.25% of the lesions were benign and 39.75% were malignant. The lesions were most often involved in the lower extremities (44 cases, 56.4%), and then the upper extremities (17 cases, 22%). Nevzat D et al.10 in their study of the Middle Black Sea region of Turkey, found that among 1482 patients (763 male, 719 female), 906 cases were benign as 14.1%. Solakoğlu and Benzer 4 likewise found bone tumors to be more common in men in their second decade, and most often around the knee joint. In the Baena-Ocampo et al.11 study from 566 patients (53.7% male, 46.3% female), 71.6% were benign lesions and 28.4% were malignant, with 39.9% involvement of the femur, 17.7% of the tibia, and 11.8% of the humerus.
Osteochondroma covers 35% of all bone neoplasms and 63.9% of benign bone tumors. In several studies, giant cell tumors are the second most common benign tumor 12 and constitute approximately 5% of all bone tumors.13 In the present study, in benign lesions, osteochondroma was the most common (16 cases, 20.5%), followed by simple bone cysts (7 cases, 10.55%) and enchondroma (6 cases, 7.7%). This result was consistent with the literature.
In the study of Nevzat D et al.10 118 of the benign lesions were osteochondroma and 68 were enchondroma. Solakoğlu and Benzer 4 found the most common benign bone tumor to be enchondroma in children and adolescents, and giant cell tumors the most common benign tumor in adults. In the study by Baena-Ocampo et al., 11 the most common benign lesions was osteochondroma (43.7%), followed by giant cell tumor (14.6%) and enchondroma (10.6%). In the study of Solooki et al.14 with 426 cases (60.1% male, 39.9% female), the most common benign bone tumor was osteochondroma (136; 63.9%), followed by enchondroma (23; 10.8%) and giant cell tumors (21; 9.9%). In benign neoplasms, the femur was the most commonly involved long bone and then the tibia (59, 27.6%) and wrist-hand (27; 12.7%). In the study of Ozkan et al.15 of a total of 57 patients (aged 5 to 18 years), 55 (94.4%) were benign tumors.
Osteochondroma was the most common tumor (31 cases, 54.3%) followed by osteoid osteoma (9 cases, 15.7%). Chondrosarcoma was found in 2 patients and Ewing sarcoma in one patient as malignant tumors, 22.8% in the upper extremities and 77.2% in the lower extremities. In our study, 67.8% of the benign lesions were located in the lower extremities followed by vertebrae and upper extremities. Osteosarcoma, as noted in several studies, is the most common primary malignant bone tumor and represents approximately 35-68% of all primary malignant bone tumors.16,17 Ewing’s sarcoma is the second most common primary bone tumor, responsible for 15.9% of all malignant bone tumors and the third most common is chondrosarcoma (14, 8.0%).18 In developed countries, the second most common is reported as chondrosarcoma.12 It is also known that metastasis to the skeletal system is common. Metastatic tumors are most common in the spine, then can be seen in the pelvis, proximal appendicular (arms and legs, upper section), and ribs. Much of the bone metastases originates from breast and prostate carcinoma, followed in turn by lung, kidney, thyroid, and the gastrointestinal tract.6 20 of our 31 malignant lesions were metastasis (25% of all cases). Chondrosarcoma was the second most common malignant lesion (5 cases, 6.25%) and chondroblastic osteosarcoma (2 cases, 2.5%) the third. The most common metastasis was from the lungs with a 35% ratio and then from renal cell cancer at a rate of 25%. 70% of the metastatic lesions were detected in males. The most common involvement places were the femur (10 cases, 50%) the iliac region (15%), and the thoracic spine (15%). In these results, our study was not consistent with the literature.
In the study of Nevzat D et al.10 58 of 308 malignant cases were osteosarcoma, chondrosarcoma was found in 36 cases, and Ewing’s sarcoma in 33 cases. These 3 tumors were more frequent in men than in women and were most commonly observed in the 51-60 age group; the most frequent localization was at the hip circumference. The most common bone tumor metastases in their study, similar to our patients, were 70 cases from the lung, 36 cases from the breast, followed by kidney and prostate; the primary tumor could not be found in 58 patients. Dorfman et al.7 in his work with bone cancer screened 2627 cases: 35% were osteosarcoma, followed by chondrosarcoma (25.8%), and Ewing sarcoma (16%). In the study of Solooki et al.14 of a total of 176 malignant neoplasms, osteosarcoma was the most common (84; 50.6%), followed by metastasis (30; 17.0%), Ewing’s sarcoma (28; 15.9%), and chondrosarcoma (14; 8.0%).
The results of our study show that some of our data share similarities with the literature but there are also some differences. At this point we can say that the distribution of bone and soft tissue tumors have particular character and also regional differences. Additional samples of bone and soft tissue tumors should be collected in surgery centers for analyses; a larger series is needed to understand the epidemiological characteristics of bone and soft tissue tumors for early diagnosis and the development of treatment strategies.
Declarations
Informed Consent
Informed consent was waived due to the retrospective nature of the study.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
None.
References
- Stiller CA, Bielack SS, Jundt G, Steliarova-Foucher E. Bone tumours in European children and adolescents, 1978-1997: report from the Automated Childhood Cancer Information System project. Eur J Cancer. 2006;42(13):2124-2135. doi:10.1016/j.ejca.2006.05.015
- Parkin DM, Stiller CA, Nectoux J. International variations in the incidence of childhood bone tumours. Int J Cancer. 1993;53(3):371-376. doi:10.1002/ijc.2910530305
- Eyre R, Feltbower RG, Mubwandarikwa E, Eden TO, McNally RJ. Epidemiology of bone tumours in children and young adults. Pediatr Blood Cancer. 2009;53(6):941-952. doi:10.1002/pbc.22194
- Çıraklı A, Dabak N, Çırak S, Sezgin H, Göçer H, Barış H. Distribution of bone tumors according to age, sex and tumor site. Acta Oncol Turc. 2005;38:38-43.
- Arıkan M, Metin E, Gürler D, Güngör Ş, Karakoç Y. Demographic features of childhood benign bone tumors and evaluation of clinical approach. Acta Oncol Turc. 2008;41(1):7-13.
- Sternberg SS, Mills SE, Carter D. Sternberg’s diagnostic surgical pathology. London: Lippincott Williams & Wilkins; 2004.
- Dorfman HD, Czerniak B. Bone cancers. Cancer. 1995;75(1 suppl):203-210.
- Pongkripetch M, Sirikulchayanonta V. Analysis of bone tumors in Ramathibodi Hospital, Thailand during 1977-1986: study of 652 cases. J Med Assoc Thai. 1989;72(11):621-628.
- Schajowicz F. Current trends in the diagnosis and treatment of malignant bone tumors. Clin Orthop Relat Res. 1983;(180):220-252. doi:10.1097/00003086-198311000-00028
- Dabak N, Çıraklı A, Gülman B, Selçuk MB, Barış S. Distribution and evaluation of bone and soft tissue tumors in the middle Black Sea Region. Acta Orthop Traumatol Turc. 2014;48(1):17-24.
- Baena-Ocampo Ldel C, Ramirez-Perez E, Linares-Gonzalez LM, Delgado-Chavez R. Epidemiology of bone tumors in Mexico City: retrospective clinicopathologic study of 566 patients at a referral institution. Ann Diagn Pathol. 2009;13(1):16-21. doi:10.1016/j.anndiagpath.2008.07.005
- Odetayo O. Pattern of bone tumours at the National Orthopaedic Hospital, Lagos, Nigeria. West Afr J Med. 2001;20(2):161-164.
- Turcotte RE. Giant cell tumor of bone. Orthop Clin North Am. 2006;37(1):35-51. doi:10.1016/j.ocl.2005.08.005
- Solooki S, Vosoughi AR, Masoomi V. Epidemiology of musculoskeletal tumors in Shiraz, south of Iran. Indian J Med Paediatr Oncol. 2011;32(4):187-191. doi:10.4103/0971-5851.95138
- Özkan EA, Göret CC, Özdemir ZT, et al. Pattern of primary tumors and tumor-like lesions of bone in children: retrospective survey of biopsy results. Int J Clin Exp Pathol. 2015;8(9):11543-11548.
- Settakorn J, Lekawanvijit S, Arpornchayanon O, et al. Spectrum of bone tumors in Chiang Mai University Hospital, Thailand according to WHO classification 2002: a study of 1,001 cases. J Med Assoc Thai. 2006;89(6):780-787.
- Günaldı M, Duman BB, Erçolak V, et al. Retrospective analysis of 119 osteosarcomas in a single centre experience. J Clin Anal Med. 2015;6(suppl 2):117-120. doi:10.4328/jcam.2689
- Günal N, Kaplan T, Zorlu E, Özpolat B, Dural K. A rarely seen scapular tumor: chondrosarcoma. J Clin Anal Med. 2015;6(suppl 1):104-107. doi:10.4328/jcam.3528
Tables
Table 1. The distribution of benign and malign lesions
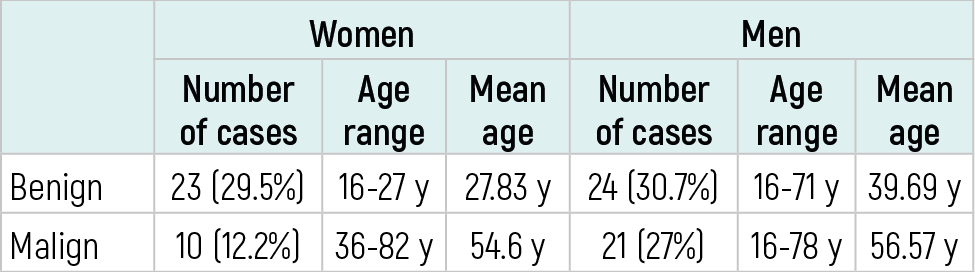
Table 2. The distribution of benign and malign lesions according to age discrimination

Table 3. The discrimination of benign and malign lesions based on anatomic location

Table 4. The number and percentage of cases and average age of bone tumors

Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
Acknowledgements
We would like to thank the Istanbul Private Ekin Pathology Laboratory for their assistance in data collection.
About This Article
How to Cite This Article
Zeynep Tugba Ozdemir, Ceren Canbey Goret. Evaluation of adult bone tumors. Eu Clin Anal Med 2026;4(3):71-73. doi:10.4328/ECAM.89
- Received:
- 22.04.2016
- Accepted:
- 29.05.2026
- Published Online:
- 01.09.2016
- Printed:
- 01.09.2016