Abstract
AimThe aim of the study was to investigate serum anti-Müllerian hormone (AMH) and various biochemical parameter levels in healthy females before and after puberta, adults with polycystic ovary syndrome and pregnant women.MethodsThe present study was performed on 100 female volunteers in four groups who applied to the polyclinic in Dr. Faruk Sukan maternal and children hospital and who had no metabolic syndrome. The groups were classified as: group 1: 7-12 years of age, prepubertal period (n=25); group 2: 18-25 years of age, pregnant females in the first trimester (n=25); group 3: 18-24 years of age, suffering from ovarian cysts (n=25); group 4: 18-24 years of age postpubertal as a control group (n=25).ResultsThe levels of AMH were found in prepubertal females (age 7-12) and the control group (age 18-24) as 3.62 pg/dl and 3.60 pg/dl, respectively (p=0.7636). The levels of AMH were 4.11 pg/dl (p=0.8690) in the women suffering
from polycystic ovary syndrome.ConclusionThe use of AMH in the measurement of ovarian reserve in clinical trials provides an advantage in early diagnosis of infertility and polycystic ovary syndrome (PCOS).
Keywords
Introduction
Anti-Müllerian hormone (AMH), also named Müllerian inhibiting substance (MIS), is produced in the ovary by ranulose cells.1 It is known as a member of the transforming growth factor-beta (TGF-β) superfamily. AMH is a homodimeric disulfide-linked glycoprotein with a molecular weight of 140 kDa.2-3 AMH is encoded by the AMH gene in humans. The gene is located on the short arm of chromosome 19 in humans, band 19 p 13.3 .4 The research implies that AMH is associated with various growth factors in the development and growth of ovarian follicles. It also exhibits the features of other TGF-β family members5-6-7, especially growth factors such as AMH and inhibin-B which are produced locally by the granulose cells and are closely associated with follicular growth.8 In the periods of fetal, prepubertal and pubertal development, determining underlying disorder mechanisms is difficult.9 Determining the level of AMH is very important in assessing ovarian reserves and in detecting, or predicting course of granulose cell tumors in clinical evaluation. Previous studies have shown the role of AMH on follicular hormone production. Studies on animals imply that AMH shows aromatase activity in granulose cells. In this way, FSH is stimulated and the number of LH receptors declines. Notwithstanding its regulatory effects on ovarian activities, AMH decreases the production of testosterone in teka cells. Levels of AMH are correlated with the number of antral follicles.10
AMH induces degeneration of the müllerian derivatives, suppressing the formation of the anlagen of the oviducts, the uterus, and the upper part of the vagina during male fetal sex differentiation.11
There is a limited population of primordial follicles in the follicle pool formed during fetal life. The germ cells are divided up to 10-15 times to reach the maximum number of oocytes, totaling up to seven million by the 20th week of pregnancy. The number of oocytes decreases in a logarithmic fashion at birth, about one million oocytes remain. A subsequent reduction in the number of oocytes occurs during childhood. Finally, by the time of the menarche period the number of oocytes is 300,000-500,000.12 The follicle reserve is limited after the loss of primordial follicles. Furthermore, during the growth phase of primordial follicles or atresia, about 1,000 follicles are lost monthly. This monthly loss rate increases after 35 years of age.13
In the period of menopause, the size of the follicle pool is about 100- 1,000 oocytes. This number of follicles is unable to maintain the hormonal concentrations necessary for normal menstrual cycles.14 After menopause, due to the loss of exposure to protective female sex steroid hormones, women have an increased risk for a number of health problems, such as osteoporosis and changes in cognitive function. Furthermore, it has been suggested that the risk for cardiovascular diseases increases after menopause.15-16 The research on ovarian cysts indicates that it is beneficial to analyse AMH levels as part of the evaluation of ovary dysfunctions such as PCOS and premature ovarian failure.17 Recent studies show that AMH has critical during the reproductive age of women. AMH has an important role in reducing the primordial follicle pool and regulating the rate of transition from the primordial into the growth stage. In addition, AMH has a protective role in decreasing the rate of exhaustion in the primordial follicle pool. AMH inhibits FSH-stimulated follicle growth, thus regulating the rate of growth and inhibiting the growing follicles in the early antral period.18-19
Chronic and irregular AMH secretion which is activated by unknown factors in granulose cells, leads to PCOS. Measurement of serum AMH levels in anovulatuar or oligoovulatuar women will assist in identifiying PCOS patients.20
No definite standarts have yet been developed for determining the ovarian reserve. The studies on whether AMH is a reliable parameter are still continuing. Recent findings reveal the importance of AMH in determining ovary function and emphasize the importance of AMH rather than FSH. For this reason, AMH levels were measured in pre- and post-pubertal healthy girls, pregnant women, and those suffering from ovarian cysts.
Materials and Methods
The present study was performed on 100 volunteers in four groups who applied to the polyclinic in the Dr. Faruk Sukan maternal and children hospital and who had no metabolic syndrome. The age, height and weight of the volunteers in groups were recorded. Tanner criteria were used to decide the term of pre-and post-puberta. The groups were divided as follows;
1. group: 7-12 years-old girls, who were in the prepubertal period (n=25)
2. group: 18-25 years-old pregnant women, who were in the first trimester (n=25)
3. group: 18-24 years-old women who were suffering from ovarian cysts, detected by ultrasound measurement (n=25)
4. group: (control group) 18-24 years-old post-pubertal girls without any health problems (n=25)
BMI (Body Mass Index) measurement, calculated as kg/m2 was performed for all four groups. Those who were obese had been excluded from the study. The blood samples (5-6 ml) were taken from individual 8 hour after
fasting. Fasting blood glucose (FBG), Follicle stimulating hormone (FSH), Testosterone (T), Estradiol 2 (E2), Luteinizing hormone (LH), High-density lipoprotein (HDL), Low-density lipoprotein (LDL), total cholesterol and triglyceride levels were analysed immediately. The rest of the samples were kept at -85°C to analyse AMH levels. AMH levels were analysed with ELISA test kits (ACTİVE Müllerian inhibiting Substance/anti-Müllerian Hormone (MIS/AMH) -Diagnostic Systems Laboratories Inc, Germany, DSL cat no: 10-14400). Analytical sensitivity of the kit was 0.006 ng/ml. Coefficients of variation were studied in eight samples and were 4.6% (0.144 ng/ ml), 2.4% (0.843 ng/ml) and 3.3% (4.408 ng/ml), respectively.Statistical AnalysisStatistical analysis was carried out with the Statistical Package for the Social Sciences (SPSS, Version 17.0). Kruskal Wallis and Mann-Whitney U tests were performed in the study due to the nonparametric distribution. The data were evaluated by aligning the levels of correlation. The relationships between the findings were examined with the Spearman correlation test. The data were expressed as median (min-max) values. The results were considered to be statistically significant (P<0.01, P<0.05).
Results
The results obtained from the study presented in Tables 1-4. The levels of AMH were found in prepubertal girls (age 7-12) and the control group (age 18-24) as 3.62 pg/dl and 3.60 pg/dl, respectively. Although the AMH levels were higher in the prepubertal group than in the control group, this difference was not statistically significant (p=0.736). The present study found the levels of AMH as 4.11 pg/dl and 3.60 pg/ dl in the women suffering from ovarian cysts and in the control group, respectively. Although, the AMH levels were higher in the group with ovarian cysts than in the control group; this differences was not statistically significant (p=0.8690). The levels of AMH were found in the first trimester of pregnancy (age 18-25) and in the control group as 3.65 pg/dl and 3.60 pg/dl, respectively. The differences between the groups were not statistically significant (p=0.1253). AMH levels increased with declining age, compared to the levels of the prepubertal and postpubertal groups. Also, higher AMH levels were found in women suffering from ovarian cysts. Minimal increases in AMH levels were found in the first three months of pregnancy.
Discussion
Clinical signs of PCOS may emerge during the peripubertal period, and premature puberta may constitute an early manifestation in some girls21-22-23 The clinical features used to diagnose PCOS in adult women are difficult to apply during adolescence. Increased androgen and insulin secretion (typical of PCOS) may be observed in normal adolescents24-25-26-27 In this context, a biochemical marker that might distinguish between normal and PCOS pubertal girls is not yet available.
AMH levels changes very little during the menstrual cycle. This feature enables the use of AMH in clinics.28 AMH may be used as a marker to follow the granulose cell tumors, recognize puberta peroxy and delayed puberta and to evaluate female gonadal function in prepubertal and pubertal girls. In the present study, AMH levels were determined as 3.62 pg/dl in girls in the prepubertal period and 3.60 pg/dl in the control group (Table 2).
Lee et al.29 determined AMH levels as 2.66 ng/ml in the prepubertal period and 1.9 ng/ml in the post-pubertal period. In the same study, the researchers also found that during infancy, the girls had the lowest levels of AMH. Furthermore, minimal decreases during the prepubertal period were determined. In the present study, statistically insignificant decreases were determined between the pre- and post-pubertal periods, declining with age (Table 2). These results are compatible with the previous studies.30-31 Thus, AMH may be a sensitive marker for ovarian aging.32-33 AMH levels were determined respectively as 3.65 pg/dl and 3.60 pg/dl in the first trimester of pregnancy (age 18-25) and in the control groups (Table 3).
A study34 conducted on pregnant women, the levels of FSH were found as 4-5 IU / L in the control group and throughout all the periods of pregnancy and the early puerperium were found as 0-1 IU / L, the lowest levels of E2 were determined in the control group and, E2 levels were found 0-5000 pg/ml in the first trimester of pregnancy. AMH levels were found as 1.9 ± 0.5 ng/ml in the follicular phase of the menstrual cycle, whereas the levels were 2.1 ± 0.56 ng/ml in the first trimester of the pregnancy. Furthermore, AMH levels were similar in the first trimester of pregnant women to those of the control group.35 There is a similarity between our study and the above-mentioned two studies.
In our study, minimal increases in AMH levels that occurred during the first trimester of pregnancy were statistically insignificant (p=0.1253). In a study carried out on pregnant women, testosterone levels were found as 2.56 ± 1.17 nmol/ml compared to 1.12 ± 0.3 nmol/ml in the control group; Estradiol 2 (E2) levels were 20,000–30,000 pg/ml in the pregnant group.36
In our study, testosterone and E2 levels were significantly higher and LH and FSH levels were significantly lower in the pregnant group than in the control group (Table 3). These results are similar to those of La Marca et al.34, Lutterodt et al.35 and Dzaja et al.36 Total cholesterol, triglyceride, HDL-cholesterol and LDL-cholesterol levels were measured in the first trimester of pregnancy and in control groups. Table 3 shows that all the parameters were insignificantly higher in the first trimester. Findings of the other studies37-38 are similar to our findings. In pregnancy, serum total cholesterol and HDL-cholesterol levels show increases parallel with the months of pregnancy, especially during late
pregnancy. Most of the pregnant women develop maternal hypertriglyceridemia. VLDL-cholesterol and LDL-cholesterol levels increase in normal pregnancy and at the end of the period reach the highest values.39-40 In this regard, our results (Table 3) are similar to those in the literature. The transition of gluconeogenetic amino acids such as alanin and glucose to the fetus, and the increases of maternal blood volume together with the increases in the volume of glucose distribution, lead to a reduction to the level of 40-50 mg/dl in maternal fasting glucose tests.41
In our study, fasting glucose levels were slightly lower in pregnant women than in the control group. In the present study, AMH levels were measured in the ovarian cyst group (age 18-24) and the control group as 4.11 pg/dL and 3.60 ± 1.83 pg/dl, respectively. The difference was statistically insignificant (p=0.8690). Chronic and irregular AMH secretion which is activated by unknown factors in granulose cells leads to polycystic ovarian syndrome. The study conducted on infants (months 2-3) who were born to PCOS mothers have showed that serum concentrations of AMH were 20.40 ± 15.60 pmol/L. In a prepubertal group who had PCOS mothers, the levels were 14.80 ± 7.70 pmol/L whereas in prepubertal girls who had mothers in the control group the levels were 9.61 ± 4.40 pmol/L.42 The levels of FSH, LH, testosterone and E2 were investigated in the same study and FSH levels were found lower in the study group than in the control group. It has been observed that AMH level is high and FSH level is low in mothers with PCOS and in their daughters in all periods. This is similar to the results of our study (Table 4).
The elevated androgen levels in women with PCOS are the cause of high levels of AMH.43 Another study notes that the AMH levels of the prepubertal daughters of women with PCOS were higher than those in in the prepubertal daughters of women without PCOS.44 This indicates that these children have a high risk of becoming PCOS in the future. So in this sense, the measurement of AMH may be an early diagnosis criterion. The data in our study is consistent with the existing literature. The ovarian cysts are benign in the present study, so that; early symptoms prediction is not completely clear. For this reason, AMH levels of patients with ovarian cysts were higher than in the other groups. Çimen et al.45 conducted a study to measure the levels of LH, FSH, LH / FSH ratio, and free, and total testosterone in the control group and in women with PCOS. They found that all of the studied parameters except for FSH were higher in the group with ovarian cysts than in the control group. It was seen that only a reduction in the level of FSH occurred. As a result of the Freaman et al.46 study on obese and nonobese women, the levels of AMH were 0.016 ng/ml and 0.046 ng/ml, respectively. The AMH levels of the women who were obese were 65% lower than the other group; this condition may be one of the causes for infertility. In our study, BMI measurements were performed for each group. The median values for each group were found as follows: group1: M=17.85, group2: M=21.48 group3: M=22.40, and group4: M=21.45. Even with a minimal increase in body mass index, a negative correlation between AMH levels within the study groups was obtained. These results are similar to those of the study by Freaman et al.46 Bayramoğlu47 found that the success rate of IVF treatment was 96% in infertile women with > 0.25 pg/ml AMH level and that the success rate remained at 23% in infertile women with <0.25 pg/ml AMH level. Prior to IVF (in vitro fertilization) treatment, AMH and Antral Follicle Count (AFC) were used to measure ovarian reserve. The success rate of IVF treatment was lower in infertile women with low serum AMH levels than in women with high levels.48 Measurement of serum AMH is also useful in the evaluation of infertility. Assessment of ovarian reserve in women with AMH is a guide on this subject. Looking at the AMH levels of women whose ovarian reserve has decreased may provide a chance to make changes in family plans before possible future infertility. These women can decide in advance to freeze eggs or to have children as soon as possible in light of the levels of this hormone. In the prepubertal and pubertal periods, high AMH levels in the daughters of mothers with PCOS indicate that these children have an increased risk of being PCOS in the future. AMH may be useful as a therapeutic hormone in several diseases including endometriosis, adenomyosis, and uterine cancer. Based on these findings, further investigations are needed.
Declarations
Informed Consent
Informed consent was obtained from all participants.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
This research was supported by Selcuk University, Scientific Research Projects Department (SÜBAP), (Project number: 09202037).
References
- Picon P. Action of the fetal testis on the development in vitro of the müllerian duct in the rat. Arch Anat Microsc Morphol Exp. 1983;58(1):19.
- Picard JY, Josso N. Purification of testicular anti-Müllerian hormone, allowing direct visualization of pure glycoprotein and determination of yield and purification factor. Mol Cell Endocrinol. 1984;34(1):23-29. doi:10.1016/0303-7207(84)90155-2
- di Clemente N, Ghaffari S, Pepinsky RB, Pieau C, Josso N, Cate RL, et al. A quantitative and interspecific test for biological activity of anti-Müllerian hormone: the fetal ovary aromatase assay. Development. 1992;114:721-727. doi:10.1242/dev.114.3.721
- Cate RL, Mattaliano RJ, Hession C, Tizard R, Farber NM, Cheung A, et al. Isolation of the bovine and human genes for müllerian inhibiting substance and expression of the human gene in animal cells. Cell. 1986;45:685-698. doi:10.1016/0092-8674(86)90783-x
- Behringer RR, Finegold MJ, Cate RL. Müllerian inhibiting substance function during mammalian sexual development. Cell. 1994;79:415-425. doi:10.1016/0092-8674(94)90251-8
- Teixeira J, Maheswaran S, Donahoe PK. Müllerian inhibiting substance, an instructive developmental hormone with diagnostic and possible therapeutic applications. Endocr Rev. 2001;22(5):657-674. doi:10.1210/edrv.22.5.0445
- Matzuk MM, Burns KH, Viveiros MM, Eppig JJ. Intercellular communication in the mammalian ovary: oocytes carry the conversation. Science. 2002;296:55-56. doi:10.1126/science.1071965
- Knight PG, Glister C. TGF-β superfamily members and ovarian follicle development. Reproduction. 2006;132:191-206. doi:10.1530/rep.1.01074
- Akdağ T, Tiftik AM, Sarıyıldız L. A comparative investigation of anti-müllerian hormone (AMH) and various biochemical parameters in patients with cryptorchidism, oligospermia or varicocele. Turk J Med Sci. 2012;42(3):411-415.
- van Rooij IA, Broekmans FJ, te Velde ER, Fauser BCJM, Bancsi LF, de Jong FH, et al. Serum anti-müllerian hormone levels: a novel measure of ovarian reserve. Hum Reprod. 2002;17:3065-3071. doi:10.1093/humrep/17.12.3065
- Weenen C, Laven JS, von Bergh AR, Cranfield M, Groome NP, Visser JA, et al. Anti-müllerian hormone expression pattern in the human ovary: potential implications for initial and cyclic follicle recruitment. Mol Hum Reprod. 2004;10(2):77-83. doi:10.1093/molehr/gah015
- Faddy MJ, Gosden RG, Gougeon A, Richardson SJ, Nelson JF. Accelerated disappearance of ovarian follicles in mid-life: implications for forecasting menopause. Hum Reprod. 1992;7(10):1342-1346. doi:10.1093/oxfordjournals.humrep.a137570
- Gougeon A. Regulation of ovarian follicular development in primates: facts and hypotheses. Endocr Rev. 1996;17:121-155. doi:10.1210/edrv-17-2-121
- te Velde ER, van Leusden HA. Hormonal treatment for the climacteric: alleviation of symptoms and prevention of postmenopausal disease. Lancet. 1994;343:654-658. doi:10.1016/s0140-6736(94)92642-5
- Gibaldi M. Prevention and treatment of osteoporosis: does the future belong to hormone replacement therapy. J Clin Pharmacol. 1997;37:1087-1099. doi:10.1002/j.1552-4604.1997.tb04292.x
- Kesslak JP. Can estrogen play a significant role in the prevention of Alzheimer’s disease. J Neural Transm. 2002;109:227-239. doi:10.1007/978-3-7091-6139-5_21
- Visser JA, de Jong FH, Laven JS, Themmen AP. Anti-müllerian hormone: a new marker of ovarian function. Reproduction. 2006;131(1):1-9. doi:10.1530/rep.1.00529
- Baarends WM, van Helmond MJ, Post M, van der Schoot PJ, Hoogerbrugge JW, de Winter JP, et al. A novel member of the transmembrane serine/threonine kinase receptor family is specifically expressed in the gonads and in mesenchymal cells adjacent to the müllerian duct. Development. 1994;120:189-197. doi:10.1242/dev.120.1.189
- Durlinger AL, Gruijters MJ, Kramer P, Karels B, Kumar TR, Matzuk MM, et al. Anti-müllerian hormone attenuates the effects of FSH on follicle development in the mouse ovary. Endocrinology. 2001;142(11):4891-4899. doi:10.1210/endo.142.11.8486
- Cook CL, Siow Y, Brenner AG, Fallat ME. Relationship between serum müllerian inhibiting substance and other reproductive hormones in untreated women with PCOS and normal women. Fertil Steril. 2002;77(1):141-146. doi:10.1016/s0015-0282(01)02944-2
- Ibáñez L, Dimartino-Nardi J, Potau N, Saenger P. Premature adrenarche: normal variant or forerunner of adult disease. Endocr Rev. 2000;21:671-696.
- Ibáñez L, Potau N, Virdis R, Zampolli M, Terzi C, Gussinyé M, et al. Postpubertal outcome in girls diagnosed with premature pubarche during childhood: increased frequency of functional ovarian hyperandrogenism. J Clin Endocrinol Metab. 1993;76:1599-1603.
- DiMartino-Nardi J. Pre- and postpubertal findings in premature adrenarche. J Pediatr Endocrinol Metab. 2000;13(5):1265-1269.
- Rosenfield RL. Hyperandrogenism in peripubertal girls. In: Mahoney CP, ed. Current issues in pediatric and adolescent endocrinology. Philadelphia, PA: Saunders; 1990:33-58. doi:10.1016/s0031-3955(16)37014-6
- Franks S. Adult polycystic ovary syndrome begins in childhood. Best Pract Res Clin Endocrinol Metab. 2002;16:263-272. doi:10.1053/beem.2002.0203
- Homburg R, Lambalk C. Polycystic ovary syndrome in adolescence: a therapeutic conundrum. Hum Reprod. 2004;19:1039-1042. doi:10.1093/humrep/deh207
- Witchel SF. Puberty and polycystic ovary syndrome. Mol Cell Endocrinol. 2006;255:146-153. doi:10.1016/j.mce.2006.04.028
- Cook CL, Siow Y, Taylor S, Fallat ME. Serum müllerian inhibiting substance levels during normal menstrual cycles. Fertil Steril. 2000;73:859-861. doi:10.1016/s0015-0282(99)00639-1
- Lee MM, Donahoe PK, Hasegawa T, et al. Müllerian inhibiting substance in humans: normal levels from infancy to adulthood. J Clin Endocrinol Metab. 1996;81:571-576. doi:10.1210/jcem.81.2.8636269
- de Vet A, Laven JS, de Jong FH, Themmen AP, Fauser BC. Anti-müllerian hormone serum levels: a putative marker for ovarian aging. Fertil Steril. 2002;72:357-362. doi:10.1016/s0015-0282(01)02993-4
- Piltonen T, Morin-Papunen L, Koivunen R, Perheentupa A, Ruokonen A, Tapanainen JS. Serum anti-müllerian hormone levels remain high until late reproductive age and decrease during metformin therapy in women with PCOS. Hum Reprod. 2005;20:1820-1826. doi:10.1093/humrep/deh850
- Fanchin R, Schonauer LM, Righini C, Guibourdenche J, Frydman R, Taieb J. Serum anti-müllerian hormone is more strongly related to ovarian follicular status than serum inhibin B, estradiol, FSH, and LH. Hum Reprod. 2003;18:323-327. doi:10.1093/humrep/deg042
- Laven JS, Mulders AG, Visser JA, Themmen AP, de Jong FH, Fauser BC. Anti-müllerian hormone serum concentrations in normoovulatory women of reproductive age. J Clin Endocrinol Metab. 2004;89:318-332. doi:10.1210/jc.2003-030932
- La Marca A, Giulini S, Orvieto R, Volpe A. Anti-müllerian hormone concentrations in maternal serum during pregnancy. Hum Reprod. 2005;20:69-72. doi:10.1093/humrep/deh819
- Lutterodt M, Byskov AG, Skouby SO, Tabor A, Yding Andersen C. Anti-müllerian hormone in pregnant women in relation to other hormones, fetal sex, and circulation of second trimester fetuses. Reprod Biomed Online. 2009;18(5):694-699. doi:10.1016/s1472-6483(10)60016-8
- Dzaja A, Wehrle R, Lancel M, Pollmächer T. Elevated estradiol plasma levels in women with restless legs during pregnancy. Sleep. 2009;32(2):169-174. doi:10.1093/sleep/32.2.169
- Matorras R, Ruiz JI, Perteagudo L, Barbazan MJ. Longitudinal study of fatty acids in plasma and erythrocyte phospholipids during pregnancy. J Perinat Med. 2001;29(4):293-297. doi:10.1515/jpm.2001.042
- Turan F, Sezgin N, Özerol E, et al. Serum lipids, lipoprotein and Lp(a) levels in preeclampsia. İÜ Tıp Fak Derg. 2002;9(3):199-203.
- Knopp RH, Herrera E, Freinkel N. Carbohydrate metabolism in pregnancy. VII. Metabolism of adipose tissue isolated from fed and fasted pregnant rats during late gestation. J Clin Invest. 1971;50:1438.
- Herrera E, Lasunción MA, Palacín M. Intermediary metabolism in pregnancy. Diabetes. 1991;40(suppl 2):83-88. doi:10.2337/diab.40.2.s83
- Brody A, Veland K, Kase N. Endocrine disorders in pregnancy. Appleton & Lange; 1989:247-272.
- Sir-Petermann T, Codner E, Maliqueo M, et al. Increased anti-müllerian hormone serum concentrations in prepubertal daughters of women with PCOS. J Clin Endocrinol Metab. 2006;91:3105-3109. doi:10.1210/jc.2005-2693
- Pellatt L, Hanna L, Brincat M, et al. Granulosa cell production of anti-müllerian hormone is increased in polycystic ovaries. J Clin Endocrinol Metab. 2007;92:240-245. doi:10.1210/jc.2006-1582
- Crisosto N, Codner E, Maliqueo M, et al. Anti-müllerian hormone levels in prepubertal daughters of women with polycystic ovary syndrome. J Clin Endocrinol Metab. 2007;92(7):2739-2743. doi:10.1210/jc.2007-0267
- Çimen S, Öztekin Ö, Gencer M, Muluk E. Places of female reproductive hormones and leptin levels in the etiopathogenesis of PCOS. Ege Tıp Derg. 2003;42(2):127-131.
- Freeman EW, Gracia CR, Sammel MD, Lin H, Lim LC, Strauss JF. Association of anti-müllerian hormone levels with obesity in late reproductive age women. Fertil Steril. 2007;87(1):101-106. doi:10.1016/j.fertnstert.2006.05.074
- Karl RH, George M, Nicholas K, LaTasha BC. Correlation of ovarian reserve tests with histologically determined primordial follicle number. Fertil Steril. 2011;95(1):170-175.
- Lekamge DN, Barry M, Kolo M, Lane M, Gilchrist RB, Tremellen KP. Anti-müllerian hormone as a predictor of IVF outcome. Reprod Biomed Online. 2007;14(5):602-610. doi:10.1016/s1472-6483(10)61053-x
Tables
Table 1. Comparison of the measured parameters of median min and max values in control, pregnant, prepubertal group and with ovarian cyst group.
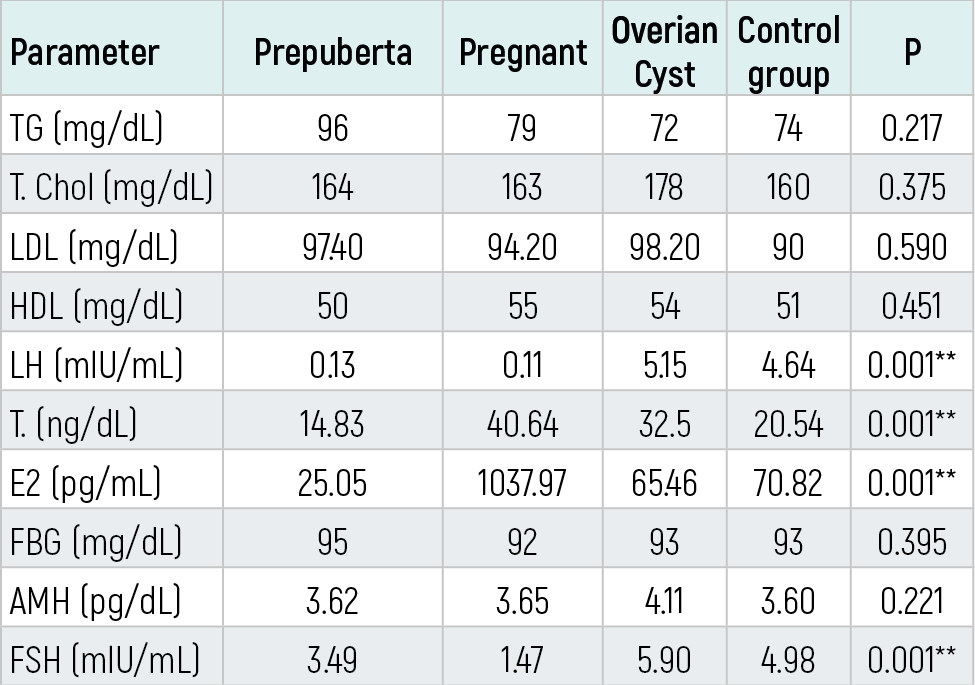
Table 2. Comparison of the measured parameters of median min and max values in postpubertal (control) and prepubertal group.

Table 3. Comparison of the measured parameters of median min and max values in postpubertal (control) and pregnant women group.
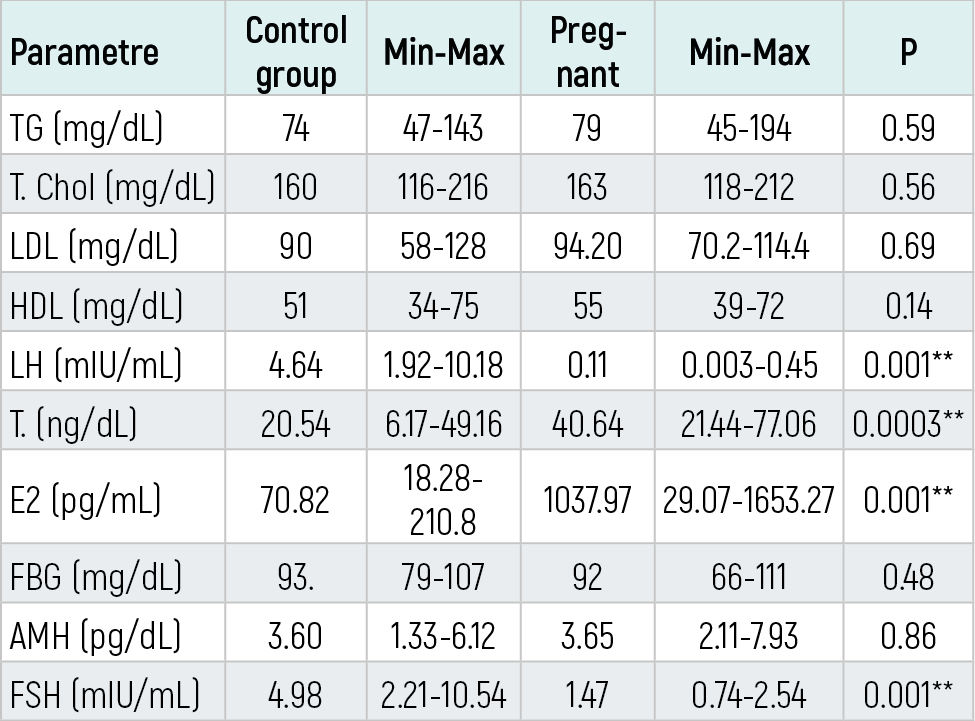
Table 4. Comparison of the measured parameters of median min and max values in postpubertal (control ) and with ovarian cyst group.
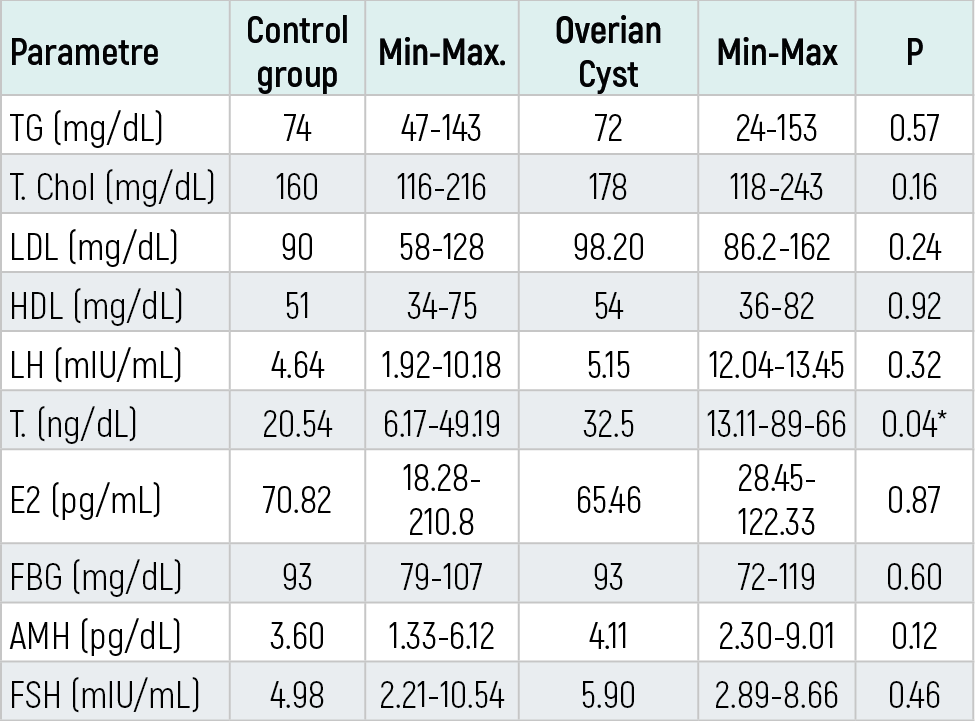
Table 5. The correlations between parameters of the prepubertal group.
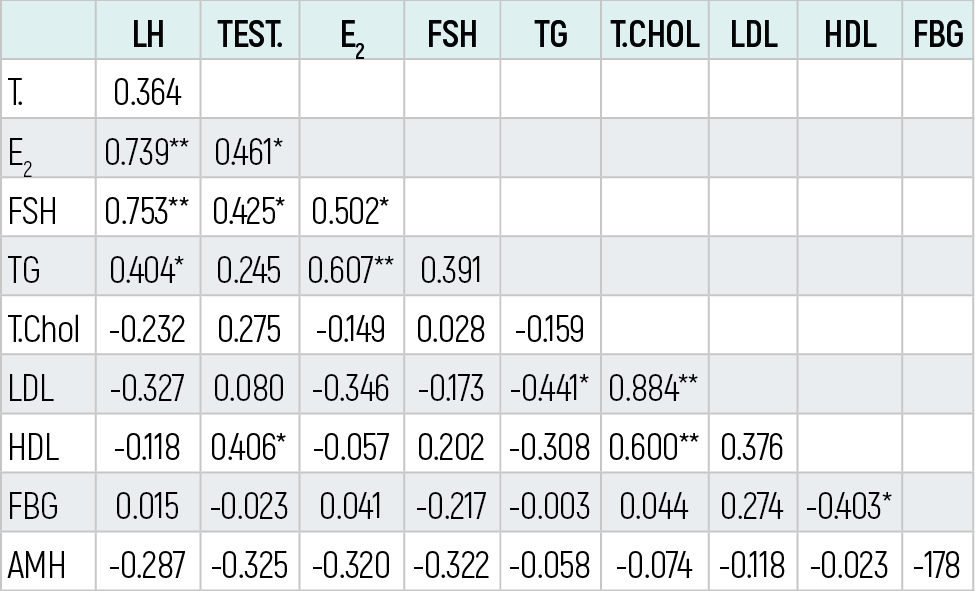
Table 6. The correlations between parameters of the pregnant group.
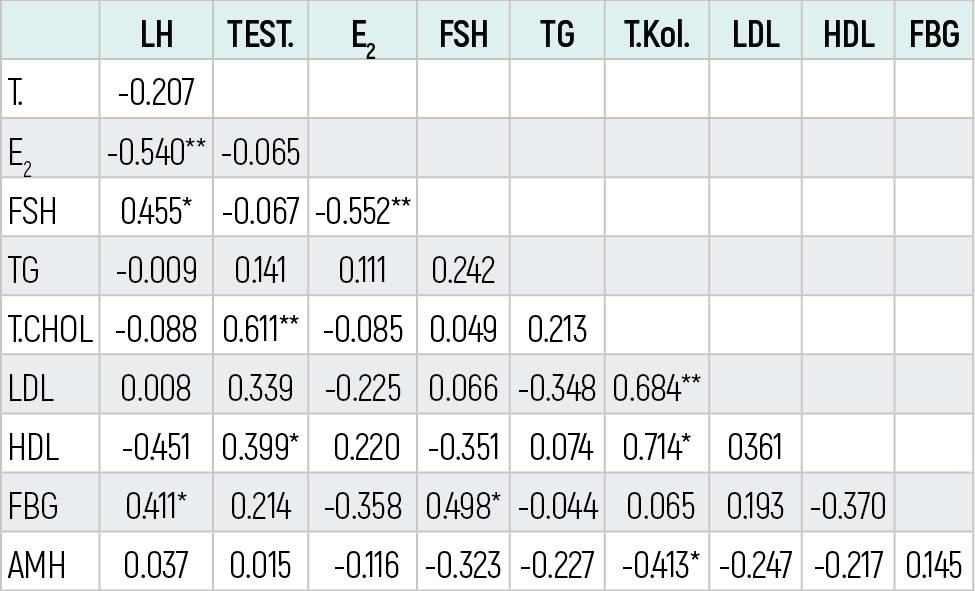
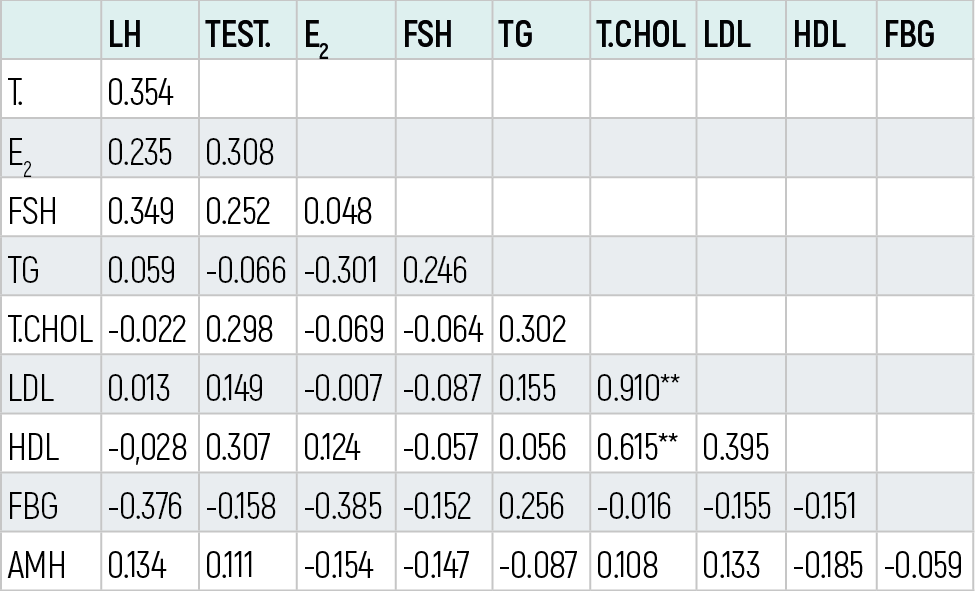
Table 7. The correlations between parameters of the ovarian cysts group
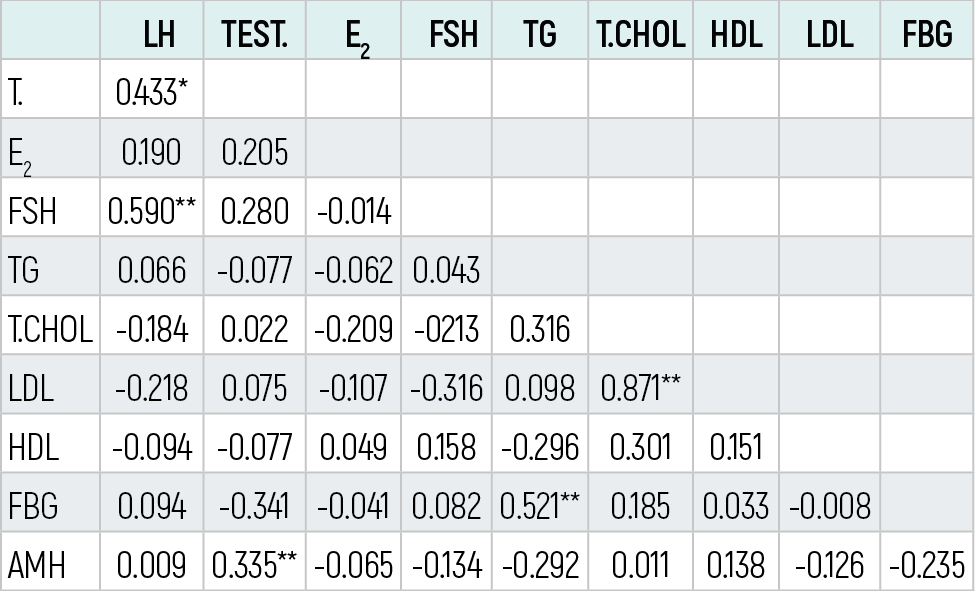
Table 8. The correlations between parameters of the postpubertal (control) group
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Levent Sarıyıldız, Turan Akdağ, Ali Muhtar Tiftik. Anti-müllerian hormone (AMH) in adults with polycystic ovarysyndrome and pregnants. Eu Clin Anal Med 2026;4(3):77-81. doi:10.4328/ECAM.92
- Received:
- 22.05.2016
- Accepted:
- 29.05.2016
- Published Online:
- 01.09.2016
- Printed:
- 01.09.2016