Abstract
AimIn this study, we aimed to evaluate geriatric patients admitted to the emergency department with CO intoxication with regard to their demographic and epidemiological factors, and to assess changes in their inflammatory parameters.MethodsThis was a retrospective study enrolling patients aged 65 years or older with a carboxyhemoglobin (COHb) level above 5%. The patients were grouped into 2 groups as mild to moderate/severe intoxication groups. Demographic, epidemiological data and inflammatory parameters were evaluated. A p-value of less than p<0.05 was considered statistically significant.ResultsThis study included 95 patients. The mean COHb level of the patients was 24. Among the study population, 63.2% presented with mild intoxication and 36.8% with moderate-severe intoxication. A comparison of the inflammatory parameters with respect to intoxication severity and cardiac involvement revealed a significantly lower platelet-lymphocyte ratio (p<0.001), but significantly higher (p<0.05) other parameters in patients with moderate-severe intoxication and cardiac involvement.ConclusionIn the present study, in which we aimed to investigate CO intoxication in the geriatric age group, we found that CO intoxication in elderly patients had characteristics similar to those of the general population. Also, we observed significant changes in all systemic inflammatory parameters in moderate-severe intoxication cases compared to mild intoxication cases.
Keywords
Introduction
Carbon monoxide (CO) intoxication is one of the most common intoxications encountered in daily life and ranks at the top among suicidal and accidental intoxications resulting in death. The mode of clinical presentation ranges from headache to coma and death, and the mortality rate is between 1% and 3%.1 Reversible carboxyhemoglobin (COHb) complex which is formed in the blood after exposure to CO, causes a reduction in oxygencarrying capacity, impairs cellular oxidative metabolism and leads to tissue hypoxia. The latter results in increased oxidative stress at the cellular level and inflammatory processes, including the formation of endogenous free oxygen radicals.2-3-4 Prior studies have defined the role of white blood cell (WBC), neutrophilto-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR]), red cell distribution width (RDW) studied from peripheral blood as inflammatory marker and/or stress markers in various conditions. It is hypothesized that these inflammatory parameters may be used as potential markers to detect inflammation in various oncological and cardiac disorders.5-6-7-8 The geriatric population makes up 6.2% of the global population. It is estimated that by 2050 geriatric population will reach 20%.2 The need for emergency medical care and health resources increases in the elderly. It has been reported that the incidence and mortality and complication rates in the geriatric population differ from those in other age groups.9 Factors such as age-related comorbidities, the sequelae of former surgeries, using multiple medications, and immune compromise lead to more atypical and severe disease courses in the geriatric population. Although elderly patients make up only a minority of intoxicated people, they suffer from a higher mortality rate that linearly increases with aging.10 There is a small body of information in the literature on the incidence and course of CO intoxication in elderly persons. We, herein, aimed to evaluate geriatric patients admitted to the emergency department with CO intoxication with regard to demographic and epidemiological aspects, and to detect any changes in their inflammatory parameters.
Materials and Methods
Study PopulationThis was a retrospective study approved by the local ethics committee. All patients aged 65 years or older who presented to Keçiören Training and Research Hospital Emergency Medicine Clinic with (CO) intoxication between 01.06.2013-01.06.2018 were enrolled. The medical records of patients with carbon monoxide intoxication were scanned from the hospital automation system (Akgün Health Information System®). Patients with a COHb level equal to or above 5% in blood gas analysis were enrolled. Patients with missing data, oncological or hematological disorders, recent myocardial infarction (<30 days), immune suppression, chronic renal failure, severe liver disease were excluded. Demographic data, systemic and neurological examination findings, full blood count parameters studied after admission to the emergency department hemoglobin, neutrophil count, lymphocyte count, platelet count, erythrocyte distribution width (RDW), serum troponin level, treatment modality applied normobaric (NBOT) or hyperbaric oxygen therapy (HBOT) were recorded. The patients were grouped into two groups on the basis of intoxication severity as follows: a) Mild intoxication: patients with non-persistent symptoms who were responsive to NBOT; b) Moderate-severe intoxication: patients with protracted symptoms [chest pain, weakness, tachycardia, tachypnea despite the administration of NBOT; those with life-threatening symptoms (hypotension, dysrhythmias, myocardial ischemia, noncardiogenic pulmonary edema, seizures, coma, cardiac arrest, respiratory arrest); and those who have had indications for HBOT or have underwent HBOT. The patients were also categorized into two groups on the basis of cardiac involvement that is troponin positivity and ischemic ECG signs. Those with troponin positivity or ischemia on the ECG were considered to have cardiac involvement.Laboratory ParametersSystemic inflammatory parameters white blood cell (WBC), neutrophil/lymphocyte ratio (NLR), platelet/lymphocyte (PLR), red cell distribution width (RDW) were evaluated in the complete blood count in geriatric patients. In our emergency department, venous blood samples were taken with heparin-containing syringes from patients with suspected carbon monoxide intoxication and studied with the Gestat 1825 (Japan) device. A complete blood count is studied with Abbott Cell Dyn 3700 (USA) device. RDW, WBC were analyzed using an automated blood cell counter. NLR was calculated as the ratio of neutrophil count to lymphocyte count, the PLR was calculated as the ratio of platelet count to lymphocyte count. Troponin and biochemical parameters were studied with the Siemens ADVIA Centaur XPT immunoassay system (German) and the Beckman Coulter AU 5800 (Japan) device.Statistical AnalysisStudy data were analyzed using IBM SPSS16.0 (Chicago, IL, USA) statistical software. The normality of discrete and continuous numerical variables was checked with the Shapiro-Wilk test. Since the data did not meet the criteria for normal distribution, they were expressed as median and interquartile range (IQR, 25%–75); categorical variables were expressed as number and percentage (%). Categorical variables were compared between the groups using the Chi-square test and continuous variables using the Mann-Whitney-U test. A p-value of less than 0.05 was considered statistically significant.
Results
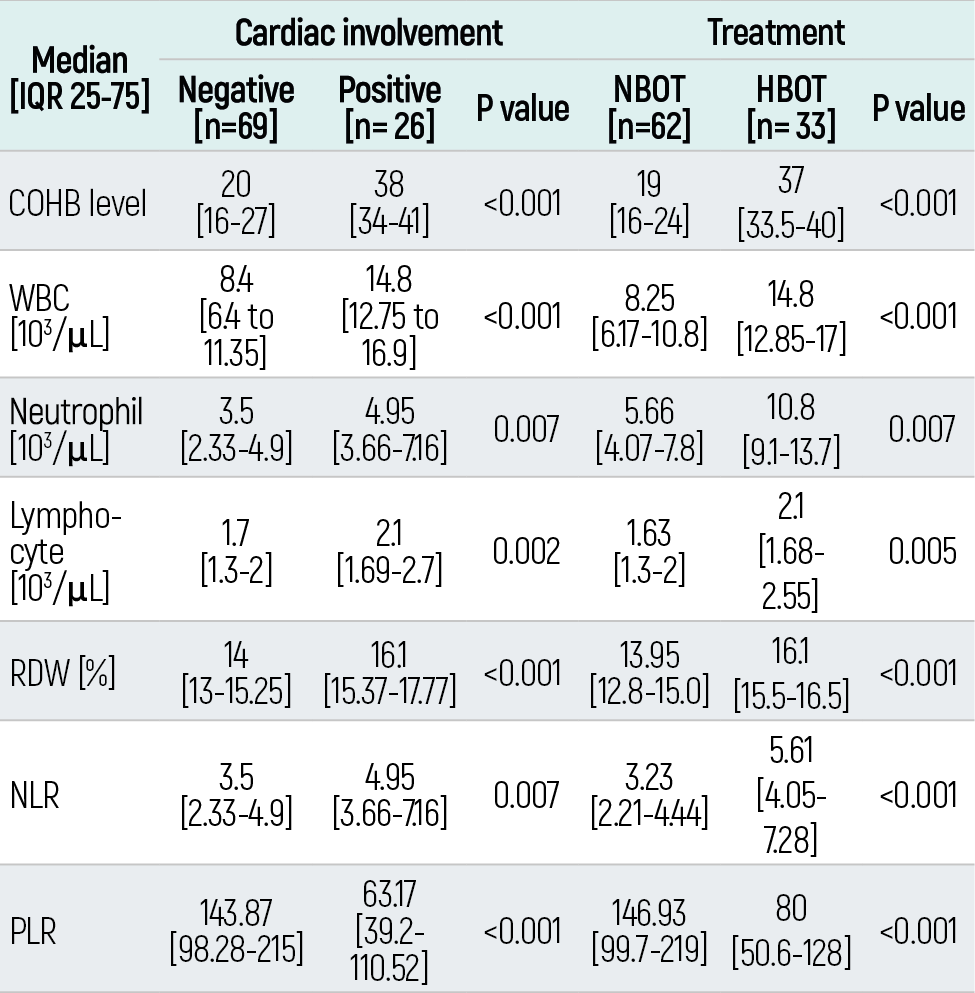
A total of 104 geriatric patients were identified for enrollment. Among these, 9 were excluded due to having missing data or meeting exclusion criteria. As a result, a total of 95 geriatric patients were included in the study for statistical analyses. Fifty-one (53.7%) patients were women; the median age of the whole study population was 70 [IQR 25-75%: 6678] years. The most common comorbidity was hypertension (62.1%). The most common symptom was headache, observed in 59 (62.1%) patients. The mean COHb level of the patients was 24 (IQR 25-75).11-12-13-14-15-16-17 The demographics, vital signs, and laboratory findings of the whole study group are shown in Table 1. The study population was categorized into two groups based on the intoxication severity, with 63.2% of the patients having had mild intoxication and 36.8% moderate-severe intoxication. Comparison of inflammatory parameters based on the intoxication severity revealed significantly lower NLR [p<0.001], but significantly higher other parameters [p<0.05] in the moderate-severe intoxication group than in the mild intoxication group (Table 2). The study population was categorized into cardiac involvement positive and negative groups based on troponin levels and ECG signs. Among those who had cardiac involvement, PLR was significantly lower [p<0.001] and other parameters were significantly higher (p<0.05) than in patients without cardiac involvement (Table 3). The patients were categorized into NBOT and HBOT groups depending on the treatment applied. The HBOT group had significantly lower PLR (p<0.001), but significantly higher other parameters (p<0.05) (Table 3).
Discussion
The geriatric population is regarded as a group that requires a specialized approach to many disorders. CO intoxication, which causes the highest mortality and morbidity in the general population, should also be carefully investigated in the elderly.9 In the present study, we aimed to investigate CO intoxication in a geriatric age group, where we observed a significant increase in all systemic inflammatory parameters among the elderly patients with moderatesevere intoxication compared to the ones with mild intoxication. We believe that this finding most probably stemmed from physiological compensatory mechanisms that lose their effectiveness with aging as well as a more profound systemic response to intoxication resulting in a more prominent increase in systemic inflammatory parameters. Considering this finding along with the inadequacy of COHb level alone to predict prognosis, we are of the opinion that systemic inflammatory parameters including NLR and PLR may guide clinicians to determine CO severity. It has been reported in the literature that psychological and mental evaluation skills are impaired among the geriatric population as a result of both cognitive impairment processes and multiple chronic disorders.10 As a result, relative incompetence to perceive and protect themselves from hazardous conditions may lead to a susceptibility to CO intoxication in this age group. Physiological handicaps secondary to advanced age lead to an expectation for more common complications and a greater mortality rate after CO exposure. The rate of cardiac complications among the general population with CO intoxication is around 15-30 %.18-19 In this study, we revealed a mortality rate of 27.4%, which was similar to that in the general population. It is a well-known fact that the cardiopulmonary reserve of the geriatric population is reduced, which may result in a more severe cardiac involvement in this population than in other age groups.20 However, we believe that such an assumption cannot be generalized to the whole geriatric population, since geriatric patients with comorbidities or susceptible to them have a wide age range and quality of care, as well as a variable physiological reserve; and when they suffer such disorders they are detected to be in variable stages of the disease. We believe that the rate of cardiac involvement demonstrated in this study supports this view. We observed the rates of 34.7% and 5.3% for HBOT need and mortality, respectively. Prior studies have reported highly variable rates for HBOT need and mortality for CO intoxication in the general population. Doğan et al. reported a rate of 32.4% for HBOT need, Emektar et al. 15%, Cervellin et al. 60.5%, and Jung et al. 87.5%.21-22-23-24 The reported mortality rates of CO intoxication range between 1% and 31%.11 We believe that this heterogeneity including our study have stemmed from the heterogeneity of the study groups.It has been stressed that COHb level alone is inadequate for predicting the complications of CO intoxication, including neurological sequelae.12-13 In contrast, NLR and PLR have been recently reported to be predictive of disease severity and prognosis in many systemic disorders affecting the general population.14-15 There is a limited number of studies exploring the role of those novel systemic inflammatory parameters in CO intoxication. A recent study by Han et al. reported that a higher admission NLR ratio and WBC count were predictors of myocardial injury in CO intoxication, with 4.83 being the optimal cut-off level for NLR with a sensitivity of 85.7% and a specificity of 45.4%.16 We found significantly higher NLR level and WBC count among geriatric patients with cardiac involvement than in those without. Similar to the results reported by Han et al., we revealed an NLR level above 4.83 (4.95) in the cardiac injury positive group. Schnittger et al. studied the neutrophil responses of patients with CO intoxication who underwent HBOT; they reported that neutrophilia detected at the time of admission may be related to organ injury. Moreover, they advocated they HBOT did not reduce neutrophil count, but may have assumed a protective role against complications by mitigating neutrophil accumulation.17 We detected significantly higher NLR levels in patients who underwent HBOT due to the presence or risk of organ dysfunction than in those who did not. In addition to these parameters, other systemic inflammatory parameters were also significantly different between the two treatment groups. This may be due to a limited compensation ability that leads to maximum response to minimum exposure in the geriatric population. Hence, excess responses in all systemic inflammatory parameters as a sign of a total inflammatory involvement seems to be the most plausible reason of our finding. Our study had some limitations. Firstly, it was conducted in a single center, and thus its findings cannot be generalized to all centers. Secondly, as it had a retrospective design, it is possible that erroneous or missing data originated from the hospital automation system may have influenced our findings Inflammatory disorders are characterized by different complex processes, and the entirety of the inflammatory parameters attributed to those inflammatory processes was not studied in the present study. This may be considered the major limitation of our study. CO intoxication features heterogeneity with respect to both general features and disease severity in the geriatric population like in the general population, which cannot be attributable to the characteristic regression of the elderly patients. Moreover, we observed significant differences in all systemic inflammatory parameters in the geriatric cases with moderate-severe intoxication than the mildly intoxicated ones. We are of the opinion that systemic inflammatory parameters including NLR and PLR may guide clinicians in detecting disease severity of CO intoxication.
Declarations
Informed Consent
Due to the retrospective nature of the study, informed consent was waived.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
None.
Abbreviations
CO: Carbon monoxide
COHb: Carboxyhemoglobin
ECG: Electrocardiography
HBOT: Hyperbaric oxygen therapy
IQR: Interquartile range
NBOT: Normobaric oxygen therapy
NLR: Neutrophil-to-lymphocyte ratio
PLR: Platelet-to-lymphocyte ratio
RDW: Red cell distribution width
STROBE: Strengthening the Reporting of Observational Studies in Epidemiology
WBC: White blood cell
References
- Hampson NB, Piantadosi CA, Thom SR, Weaver LK. Practice recommendations in the diagnosis, management, and prevention of carbon monoxide poisoning. Am J Respir Crit Care Med. 2012;186(11):1095-1101. doi:10.1164/rccm.201207-1284ci
- Cagatay AA, Tufan F, Hindilerden F, Aydin S, Elcioglu OC, Karadeniz A, et al. The causes of acute fever requiring hospitalization in geriatric patients: comparison of infectious and noninfectious etiology. J Aging Res. 2010;2010:380892. doi:10.4061/2010/380892
- Thom SR. Carbon monoxide pathophysiology and treatment. In: Thom SR, Neuman T, editors. Physiology and medicine of hyperbaric oxygen therapy. Philadelphia, PA: Saunders; 2008:321-334. doi:10.1016/b978-1-4160-3406-3.50020-2
- Kaya H, Coskun A, Beton O, Zorlu A, Kurt R, Yucel H, et al. Carboxyhemoglobin levels predict the long-term development of acute myocardial infarction in carbon monoxide poisoning. Am J Emerg Med. 2016;34(5):840-844. doi:10.1016/j.ajem.2016.01.036
- Sun X, Luo L, Zhao X, Ye P, Du R. The neutrophil-to-lymphocyte ratio on admission is a good predictor for all-cause mortality in hypertensive patients over 80 years of age. BMC Cardiovasc Disord. 2017;17(1):167. doi:10.1186/s12872-017-0595-1
- Yan W, Li JZ, He KL. The relationship between neutrophil-to-lymphocyte ratio and major cardiovascular events in elderly patients with chronic heart failure. J Geriatr Cardiol. 2017;14(12):780-784.
- Doğan NO, Akıncı E, Gümüş H, Akıllı NB, Aksel G. Predictors of in-hospital mortality in geriatric patients presenting to the emergency department with ischemic stroke. Clin Appl Thromb Hemost. 2016;22(3):280-284. doi:10.1177/1076029614550820
- Emektar E, Corbacioglu SK, Dagar S, Uzunosmanoglu H, Safak T, Cevik Y. Prognostic value of the neutrophil-lymphocyte and platelet-lymphocyte ratios in predicting one-year mortality in patients with hip fractures aged over 60 years. Eurasian J Emerg Med. 2017;16:165-170. doi:10.5152/eajem.2017.51523
- Aygencel G, Karamercan A, Akinci E, Demircan A, Keles A. Metabolic syndrome and its association with ischemic cerebrovascular disease. Adv Ther. 2006;23(3):495-501. doi:10.1007/bf02850171
- Cavlak M, Akçan R, Tümer AR, Balseven AO, Lale A, Yildirim MS, et al. Forensic medicine evaluation of Alzheimer patients: a series from Ankara, Turkey. Turk J Med Sci. 2015;45(5):1047-1050. doi:10.3906/sag-1403-80
- Guzman JA. Carbon monoxide poisoning. Crit Care Clin. 2012;28(4):537-548. doi:10.1016/j.ccc.2012.07.007
- Hampson NB, Hauff NM. Carboxyhemoglobin levels in carbon monoxide poisoning: do they correlate with the clinical picture? Am J Emerg Med. 2008;26(6):665-669. doi:10.1016/j.ajem.2007.10.005
- Moon JM, Shin MH, Chun BJ. The value of initial lactate in patients with carbon monoxide intoxication in the emergency department. Hum Exp Toxicol. 2011;30(8):836-843.
- Kaplan M, Ates I, Oztas E, Yuksel M, Akpinar MY, Coskun O, et al. A new marker to determine prognosis of acute pancreatitis: PLR and NLR combination. J Med Biochem. 2018;37(1):21-30. doi:10.1515/jomb-2017-0039
- Akpinar MY, Ozin YO, Kaplan M, Ates I, Kalkan IH, Kilic ZMY, et al. Platelet-to-lymphocyte ratio and neutrophil-to-lymphocyte ratio predict mucosal disease severity in ulcerative colitis. J Med Biochem. 2018;37(2):155-162. doi:10.1515/jomb-2017-0050
- Han YY, Wang Y, Zhao GQ, Yang JL, Wang L, Wang WZ. Relationship between neutrophil-to-lymphocyte ratio and myocardial injury induced by acute carbon monoxide poisoning. Zhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi. 2018;36(5):362-364.
- Schnittger V, Rosendahl K, Lind F, Palmblad J. Effects of carbon monoxide poisoning on neutrophil responses in patients treated with hyperbaric oxygen. J Investig Med. 2004;52(8):523-530. doi:10.1136/jim-52-08-24
- Satran D, Henry CR, Adkinson C, Nicholson CI, Bracha Y, Henry TD. Cardiovascular manifestations of moderate to severe carbon monoxide poisoning. J Am Coll Cardiol. 2005;45(9):1513-1516. doi:10.1016/j.jacc.2005.01.044
- Henry CR, Satran D, Lindgren B, Adkinson C, Nicholson CI, Henry TD. Myocardial injury and long-term mortality following moderate to severe carbon monoxide poisoning. JAMA. 2006;295(4):398-402. doi:10.1001/jama.295.4.398
- Dai X, Hummel SL, Salazar JB, Taffet GE, Zieman S, Schwartz JB. Cardiovascular physiology in the older adults. J Geriatr Cardiol. 2015;12(3):196-201.
- Doğan NÖ, Savrun A, Levent S, Günaydın GP, Çelik GK, Akküçük H, et al. Can initial lactate levels predict the severity of unintentional carbon monoxide poisoning? Hum Exp Toxicol. 2015;34(3):324-329. doi:10.1177/0960327114538986
- Emektar E, Ramadan H, Yüzbaşıoğlu Y, Vural S, Coşkun F. Use of lactate clearance in determining serum lactate levels and effectiveness of treatment in carbon monoxide poisonings. KÜ Tıp Fak Derg. 2017;19(2):60-65.
- Cervellin G, Comelli I, Rastelli G, Picanza A, Lippi G. Initial blood lactate correlates with carboxyhemoglobin and clinical severity in carbon monoxide poisoned patients. Clin Biochem. 2014;47(18):298-301. doi:10.1016/j.clinbiochem.2014.09.016
- Jung JW, Lee JH. Serum lactate as a predictor of neurologic outcome in emergency department patients with acute carbon monoxide poisoning. Am J Emerg Med. 2019;37(5):823-827. doi:10.1016/j.ajem.2018.07.046
Tables
Table 1. Demographic properties of the study population
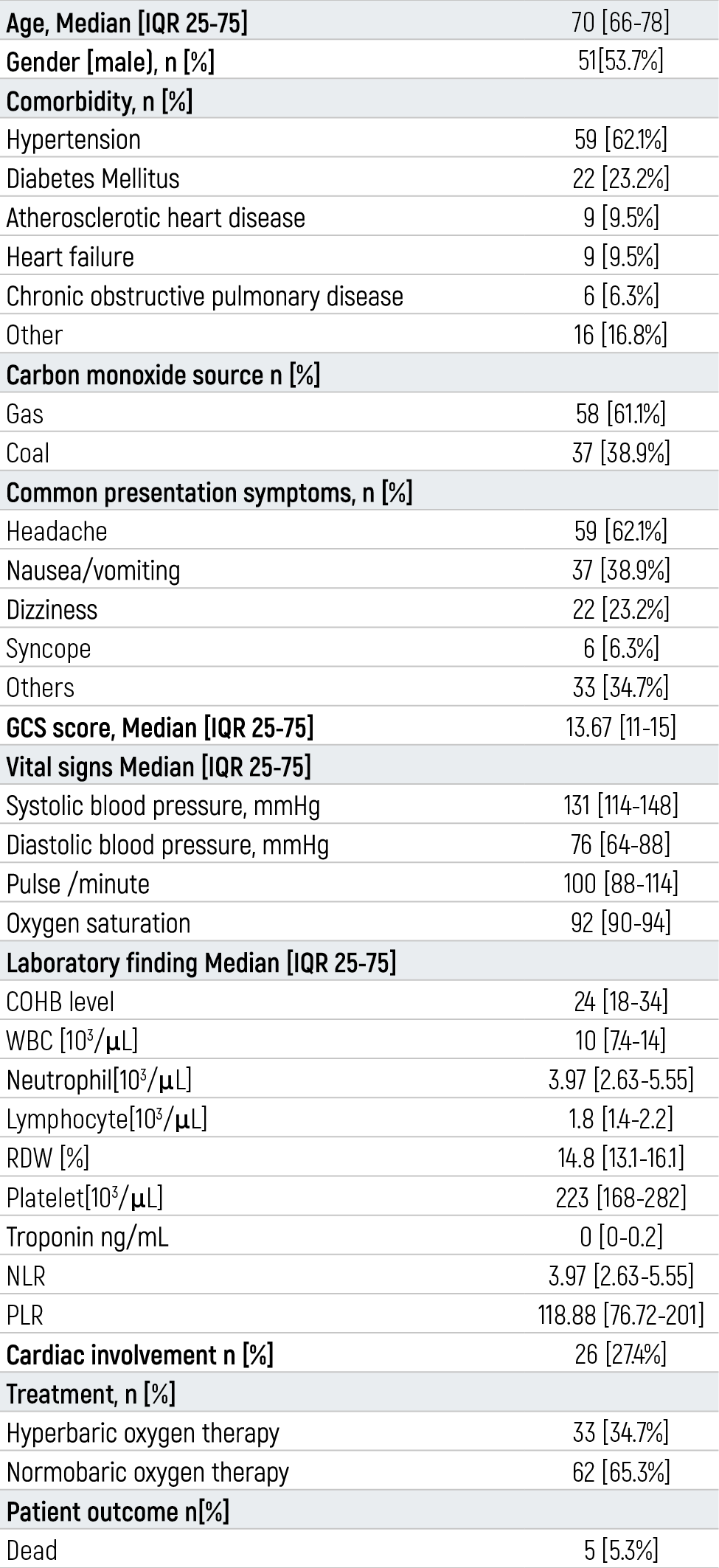
Table 2. Laboratory findings of patients according to toxicity severity
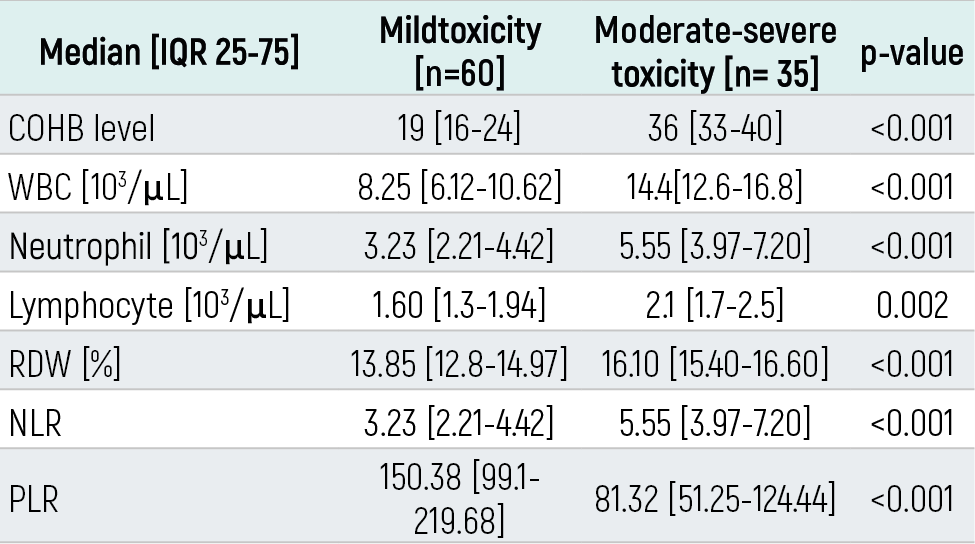
Table 3. Laboratory findings of patients according to cardiac involvement and treatment
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Hüseyin Uzunosmanoğlu, Seda Dağar, Şeref Kerem Çorbacıoğlu, Yunsur Çevik. Evaluation of geriatric patients with carbon monoxide intoxication presenting to the emergency department. Eu Clin Anal Med 2026;9(1):1-5. doi:10.4328/ECAM.10025
- Received:
- 21.10.2020
- Accepted:
- 21.11.2020
- Published Online:
- 03.12.2020
- Printed:
- 01.01.2021