An epiglottic vallecular cyst incidentally discovered during cervicalspinal magnetic resonance imaging: A Case Report
Epiglottic vallecular cyst
Authors
Abstract
IntroductionLaryngeal cyst is a rare entity that constitutes only 4.3-6% of all benign laryngeal tumors and epiglottic vallecular cyst (EVC) is a variant of laryngeal cysts. As EVCs mostly remain asymptomatic in adulthood, they are only followed up without any intervention.
Case PresentationHowever, recent studies have shown that EVCs are not as innocuous as they have previously been regarded. Therefore, the detection of these lesions is of clinical importance. The majority of the EVCs are unintentionally discovered by otolaryngologists, anesthesiologists or endoscopists. But they may also be incidentally detected by radiologists during imaging studies performed for another purpose.
ConclusionHere, we present a 41-year-old lady who admitted with complaints regarding her neck and left upper limb and an EVC was detected in her left vallecula during the cervical spinal magnetic resonance imaging study.
Keywords
Introduction
Laryngeal cyst is a rare entity that constitutes only 4.3-6% of all benign laryngeal tumors. And epiglottic vallecular cyst (EVC), also known as “epiglottic mucous retention cyst” or “base of the tongue cyst”, is a variant of laryngeal cysts. EVCs constitute 52% of all laryngeal cysts. They develop as the result of ductal obstruction and mucus retention in the submucosal glands.1 They are approximately twice as common in males and can be detected at any age.2 Although EVCs are considered as self-limiting benign lesions that mostly remain asymptomatic, they may at times cause airway obstruction and fatal complications.3 The majority of the EVCs are incidentally discovered by otolaryngologists, anesthesiologists or endoscopists. However, they may also be detected by radiologists during imaging studies for another purpose.2 Here, we present a 41-year-old lady who admitted with complaints regarding her neck and left upper limb and an EVC was detected in her left vallecula during the cervical spinal magnetic resonance imaging (MRI) study.
Case Presentation
A 41-year-old female who presented with progressive neck pain along with numbness and weakness of the left upper limb for the last 2 years was referred to the Department of Radiology for cervical spinal MRI. The MRI study was performed on a 1.5T unit (Magnetom Aera, Siemens, Erlangen, Germany) with a 20-channel head-neck coil. Besides the degenerative spinal changes which seemed to correspond to the complaints of the patient, MR images revealed a well-defined homogeneous mass measuring 13 x 12 x 8 mm (CC x TR x AP) in the left supraglottic area, expanding the left vallecula (Figure 1 and Figure 2). It was a cyst with a thin, regular wall and was abutting the bases of the left hemitongue and the left half of the epiglottis. The cyst followed cerebrospinal fluid signal intensity on T1- and T2-weighted images and showed no sign of infiltration or invasion in any sequences. Based on the characteristic imaging findings, the lesion was diagnosed as EVC. As the lesion was asymptomatic, no treatment was planned. However, the patient was informed about the presence of the cyst and its possible complications.
Discussion
In early infancy, an EVC may cause airway obstruction, feeding difficulties and developmental delay as the result of swallowing pressure and obstruction of the laryngeal inlet. And later in childhood, EVCs may cause stridor, cyanosis, respiratory difficulties or sudden airway obstruction.1,2 They may cause unexpected airway block and become life-threatening also in adulthood.3 However, most adult EVCs remain asymptomatic unless they reach a large size or show rapid growth due to bleeding or infection. And they are mostly discovered unintentionally during the routine otolaryngological examination, induction of general anesthesia or upper gastrointestinal endoscopy. Different from the previously reported cases, we herein report an incidentally discovered EVC during a routine imaging study. As most of the small EVCs, like the one we currently present, are silent lesions, follow-up without intervention to the cyst is a widely accepted clinical approach among otolaryngologists.1,2,3 However, recent studies have shown that EVCs are not as innocuous as they have been thought to be and suggested a reconsideration of the clinical approach to these lesions.1,4,5 In their study with a cohort of adults with acute epiglottitis, Yoon et al. showed that a pre-existing epiglottic cyst is associated with the development of a supraglottic suppurative infection. Furthermore, they also showed that, regardless of how the epiglottitis developed, the presence of an infected epiglottic cyst increases the risk for airway obstruction as well as recurrence of acute epiglottitis. Based on their results, they suggested the current clinical approach to EVCs be re-addressed. And they recommended that patients be informed about the associated risks and current interventions, even if the EVC is an asymptomatic one.5 According to the current approach, a symptomatic EVC can be treated either by elective endoscopic resection or by marsupialization. Both methods are reported to be quite safe with good long-term results. On the other hand, in cases of EVC causing acute airway obstruction, simple evacuation of the cyst is performed.6 As the lesion of the patient we present was a small and an asymptomatic one, no intervention was planned. However, the patient was informed about the presence of the cyst and its possible complications in detail.
Conclusion
Small and asymptomatic EVCs are often incidentally detected by otolaryngologists, anesthesiologists or endoscopists. However, they may also be detected during an imaging study performed for another purpose. These lesions may not always be innocuous. Therefore, regardless of how the lesion is detected, the patient should be informed about the associated risks and current interventions.
Declarations
Animal and Human Rights Statement
No animal experiments were performed in this study. All procedures involving the patient were conducted in accordance with institutional and ethical standards.
Informed Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Conflict of Interest
The authors declare no conflict of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the scientific content of the article, including study design, data collection, analysis and interpretation, manuscript preparation, and approval of the final version of the manuscript.
References
-
Berger G, Averbuch E, Zilka K, Berger R, Ophir D. Adult vallecular cyst: thirteen-year experience. Otolaryngol Head Neck Surg. 2008;138:321-327. doi:10.1016/j.otohns.2007.12.008
-
Lee SH, Lee DJ, Kim KM, Kim KN, Seo SW, Park KY, et al. Epiglottic cyst incidentally discovered during screening endoscopy: a case report and review of the literature. Korean J Fam Med. 2014;35:160-166. doi:10.4082/kjfm.2014.35.3.160
-
De Vries EJ, Seranno JA. Airway collapse due to unsuspected epiglottic cyst. Laryngoscope. 2010;120(suppl):S54. doi:10.1002/lary.21238
-
Sonny A, Nagaraj G, Ramachandran R. Asymptomatic epiglottic cyst: a rare cause of unanticipated difficult intubation. Middle East J Anesthesiol. 2011;21:119-120.
-
Yoon TM, Choi JO, Lim SC, Lee JK. The incidence of epiglottic cysts in a cohort of adults with acute epiglottitis. Clin Otolaryngol. 2010;35:18-24. doi:10.1111/j.1749-4486.2009.02069.x
-
Vourexakis Z. Epiglottic cysts in clinical practice. Cleve Clin J Med. 2016;83(5):388-389. doi:10.3949/ccjm.83a.15059
Figures

Figure 1. Sagittal T1- (a) and T2-weighted (b) magnetic resonance images demonstrating a well-defined cystic lesion with a thin regular wall in the supraglottic area (arrows). Note the cyst abuts the bases of the tongue and epiglottis. It expands the vallecula but there is no evidence of infiltration.
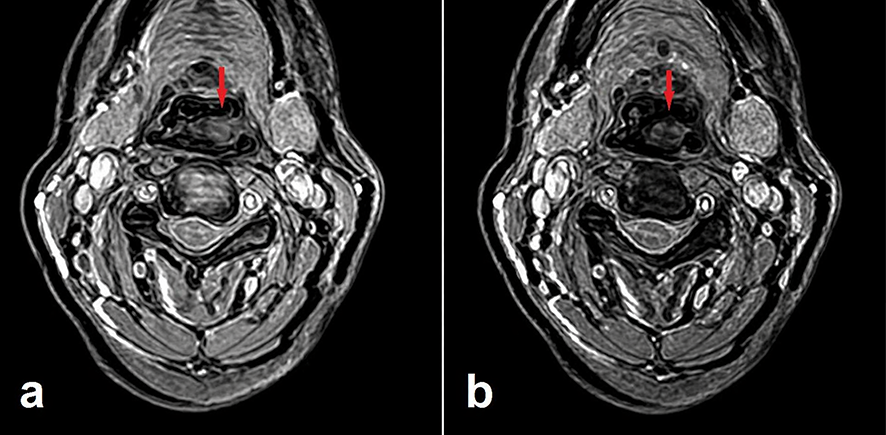
Figure 2. Consecutive axial gradient-echo T2-weighted magnetic resonance images show that the cyst is located in the left half of the supraglottic area (arrows).
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Rasime Pelin Kavak, Meltem Özdemir. An epiglottic vallecular cyst incidentally discovered during cervicalspinal magnetic resonance imaging: A Case Report. Eu Clin Anal Med 2020;8(1):1-3. doi:10.4328/ECAM.10017
- Received:
- December 5, 2019
- Accepted:
- December 21, 2019
- Published Online:
- December 22, 2019
- Printed:
- January 1, 2020