Effects of nutrient deficiencies on the development of restless leg syndrome in pediatric patients with primary malnutrition
Relationship between nutritional status and restless legs syndrome
Authors
Abstract
AimAlthough it is emphasized in the literature that conditions such as celiac disease, obesity, and iron deficiency cause an increase in Restless legs syndrome (RLS) incidence, there are not enough studies evaluating the effects of primary malnutrition on the development of RLS. Therefore, in this study, we aimed to evaluate the effects of vitamin and mineral deficiencies on the risk of developing RLS in pediatric patients with primary malnutrition.
MethodsA this study included a total of 100 patients aged 11-18 years who presented to Pediatric Gastroenterology, Hepatology, and Nutrition outpatient clinic and who were diagnosed with malnutrition due to low oral intake between July 2017 and July 2018 and 70 control subjects.
ResultsThe RLS was detected in 18 (18%) in the primary malnutrition group and in four patients (5.7%) in the control group. Anemia, hypoferritinemia, vitamin D deficiency, folic acid deficiency were significantly more common in the RLS group (p<0.05). When potential risk factors for RLS development are evaluated according to logistic regression analysis, 30.222 times in patients with anemia; 27,692 times in patients with hypoferritinemia; 29,951 times in patients with vitamin D deficiency; 10.08 times in patients with vitamin D deficiency; 10,615 times in patients with multivitamin deficiency; we detected 3.622 times higher risk of developing RLS in malnourished patients. Moderately weak and severe stunting increased the risk of developing RLS 2,971 and 4,670 times, respectively, while severe weak, moderate stunting did not pose a significant risk for the development of RLS.
ConclusionOur study shows that malnutrition, anemia, vitamin and mineral deficiencies increase the risk of developing RLS.
Keywords
Introduction
Restless legs syndrome (RLS) is characterized by neurological events characterized by annoying paresthesia in and irresistible instinct to move legs during sleep or rest. Although it has mostly idiopathic and hereditary occurrence, it may develop secondary to iron deficiency, end-stage renal disorders, pregnancy, rheumatological disorders, diabetes, and neurological disorders such as spinal cord injuries, multiple sclerosis, Parkinson’s disease, and polyneuropathy. Its prevalence is reported to be 1-15%.1
Considering the studies indicating the role of the dopaminergic system in the RLS pathogenesis.1 as well as the key role of iron on the dopaminergic system, malnutrition, as an important cause of iron deficiency, gains importance. Several studies have indicated an increased incidence of RLS in Coeliac disease and iron deficiency.2 In this study, we also aimed to investigate the relationship between RLS prevalence and nutritional status among patients with malnutrition due to low oral intake, a subject which has sparsely studied so far.
Materials and Methods
Patient SelectionThis study included a total of 100 patients aged 11-18 years who presented to Pediatric Gastroenterology, Hepatology, and Nutrition outpatient clinic and who were diagnosed with malnutrition due to low oral intake between July 2017 and July 2018 and 70 control subjects. All patients and their families gave informed consent prior to study entry. RLS was diagnosed by the criteria established by the International Restless Legs Syndrome Study Group (IRRLS) for the 11-18 age group.3 The questionnaire assessed RLS diagnostic criteria using 5 questions and those criteria were requestioned using 6 cross questions. Patients meeting all RLS criteria were diagnosed with RLS. In order to confirm the RLS diagnosis, patients meeting the RLS criteria were interviewed via telephone and cross questions were asked. When conflicting answers were obtained from a patient or his/her family during 15-30-minute interviews, this patient was excluded.
Assessment of Nutritional StatusIn all patients participating in the study, height was measured without socks and shoes using a calibrated vertical portable stadiometer, to the nearest millimeter. Weight was measured with light clothing using a digital electronic weighing scale, to the nearest decimal fraction of a kilogram. Weight Z score, height Z score, Weight by height (WBH) Z score, body mass index (BMI) Z score were calculated according to age and sex using World Health Organization (WHO) data. Patients with a Z
score below -2 in any of the parameters of body weight, height, WBH, BMI were considered as malnourished. Hemogram, vitamin B12, folic acid ferritin, and vitamin-D levels were simultaneously studied.
Severity of malnutrition was classified as fallows.4Moderate underweight: Weight-for-age Z-score ≥−3 SDS to <−2 SDS Severe underweight: Weight-for-age Z-score <−3 SDS Normal: Weight-for-age Z-score >−2 SDS Moderate stunting: Height-for-age Z-score ≥−3 SDS to <−2 SDS Severe stunting: Height-for-age Z-score ≥−3 SDS Normal: Height-for-age Z-score >−2 SDS
Assessment of Laboratory ParametersLaboratory studies performed one month earlier were examined. Hemogram, vitamin D, vitamin B12, folic acid, and ferritin levels were examined. The tests that were lacked were performed after patients and relatives were informed and their informed consent was obtained. Local Ethics Committee approved this study. Serum folic acid, vitamin B12, and ferritin were calculated at 28 0C by a photo multiplier using the electrochemiluminescence method in a Roche Cobas 6000 (601) device and after 18-minute and 27-minute incubation period
Levels were Defined as Follows• Vitamin D deficiency, <20 ng/ml
• Vitamin D insufficiency, 21-29 ng/ml
• Normal levels of Vitamin D≥30 ng/ml.5 Ferritin (µg/L): <30 ng/mL was considered hypoferritinemia.6 Vitamin B12: <300 pg/mL was considered vitamin B12 deficiency.7 Folate: <4 µg/L was considered folic acid deficiency.8
Multivitamin deficiency: At least two of Ferritin, Vitamin B12, folic acid, vitamin D deficiency, and vitamin D insufficiency were considered multivitamin deficiency Anemia: A Hemoglobin level less than the age-based normal level was considered anemia
Exclusion Criteria were as Follows• Patients below the age of 11 years or above the age of 18 years,
• Patients with chronic conditions other than insufficient intake, which could cause malnutrition, such as Coeliac disease, cystic fibrosis, heart failure, chronic renal failure, cerebral palsy, Down syndrome, chronic diarrhea, malabsorption secondary to bowel surgery, feeding by gastrostomy, inflammatory bowel disease, and diabetes.
• Patients with disorders mimicking RLS, such as positional leg pain, growth pain, tendon, ligament and muscle pain, arthritis, Osgood-Schlatter disease, and patellar chondromalacia.
• Patients that had been treated with vitamin and/or iron within the last three months.
Statistical AnalysisStatistical Package for the Social Sciences for Windows (SPSS Inc., Chicago) 22.0 software package was used for all statistical analyses. Study data were expressed as mean ± standard deviation, number (n), and percentage (%). Distribution of quantitative variables was tested using the Kolmogorov Smirnov test. Those with normal distribution were compared using the
Student’s t test or one-sided analysis of variance (ANOVA) and those without normal distribution using the Mann Whitney-U test or the Kruskal-Wallis test. Statistical significance was tested with the Chisquare test, the Student’s t-test, or the Mann-Whitney U test. Logistic regression analysis was used to demonstrate any correlation between a dependent variable and one or more independent variables. A p-value of less than 0.05 was considered statistically significant.
Results
The mean age was 13.8429±2.19113 (11-17) years in the control group and 13.015±1.79991 (11-17.5) years in the malnutrition group (Table 1). The female-tomale ratio was 2/3 in the control group and 3/2 among the patients with malnutrition. There was no significant difference between the groups with and without RLS with respect to gender distribution (P=0.461, Table 2). Among 23 patients meeting the RLS diagnostic criteria, five were excluded from the RLS group after cross questions, and 18 (18%) patients with malnutrition were diagnosed with RLS. In the control
group, two out of six patients were excluded from the RLS group after questioning with the cross questions and four (5.7%) patients were diagnosed with RLS.
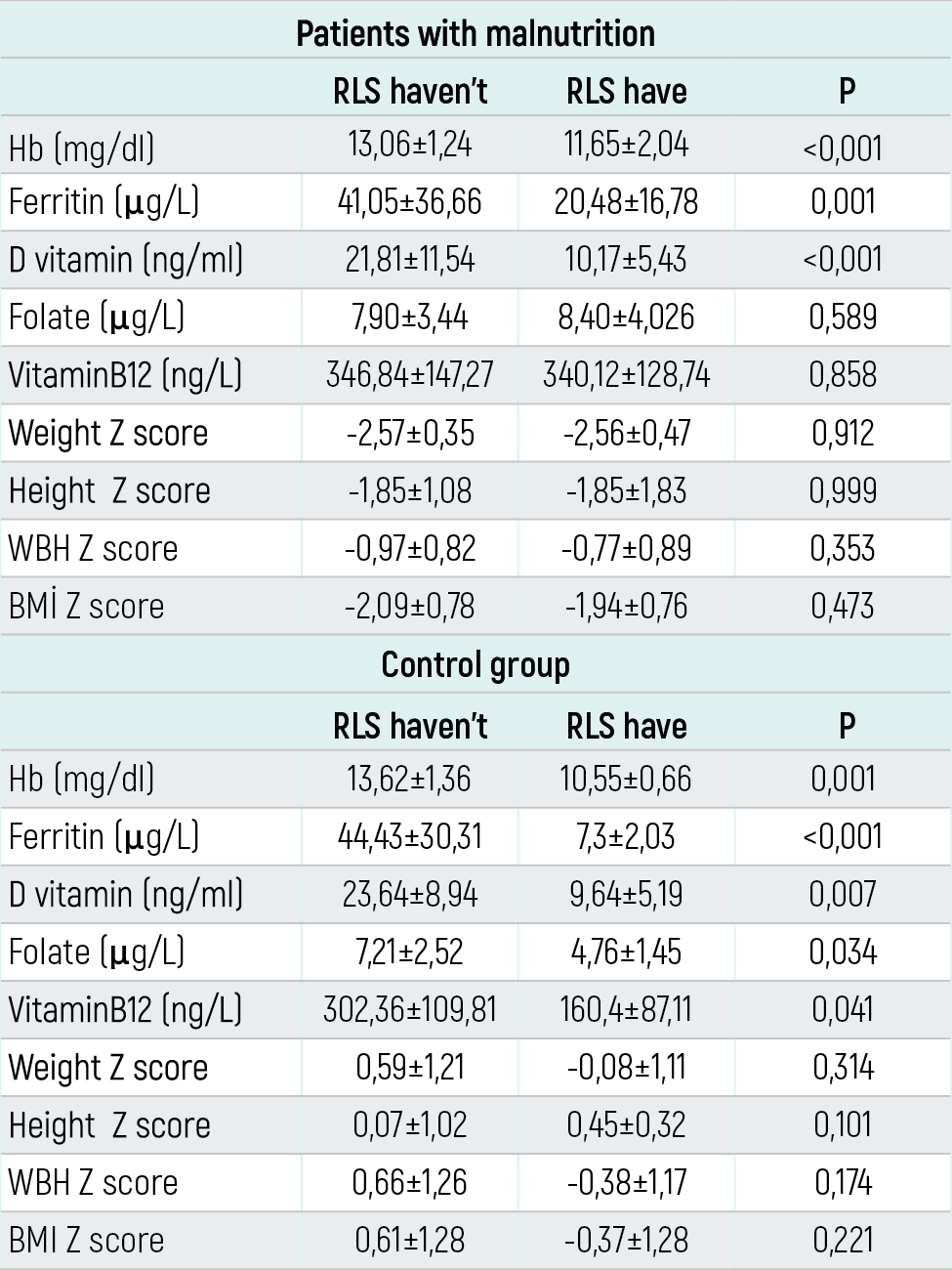
The examination of patients with and without RLS in terms of clinical and laboratory findings revealed that both groups had similar gender distribution. However, Anemia, hypoferritinemia, vitamin D deficiency, vitamin D insufficiency, folic acid deficiency, and multivitamin deficiency were significantly more common in the RLS group (P<0,001, P<0,001, P<0,001, P=0,007, P=0,044, P<0,001, respectively). Both groups were similar with regard to vitamin B12 deficiency (P=0,052) (Table 2) The analysis of the laboratory parameters and the anthropometric measurements between the RLS patients and the controls showed that among patients with malnutrition, RLS patients had a significantly lower Hb, ferritin, and vitamin D levels (P=<0,001, P=0,001, P=<0,001,
respectively) while folate, vitamin B 12 serum levels and weight Z score, height Z score, WBH Z score, BMI Z score were similar between those with RLS and without. (P=0,589, P=0,858, P=0,912, P=0,999, P=0,353, P=0,473, respectively). In the control group, patients with RLS had significantly lower Hb, ferritin, vitamin D, folate, and vitamin B12 levels compared to those without RLS (P=0,001, P=<0,001, P=0,007, P=0,034, P=0,041, respectively); there was no significant difference between both groups with respect to weight Z score, height Z score, WBH Z score, BMI
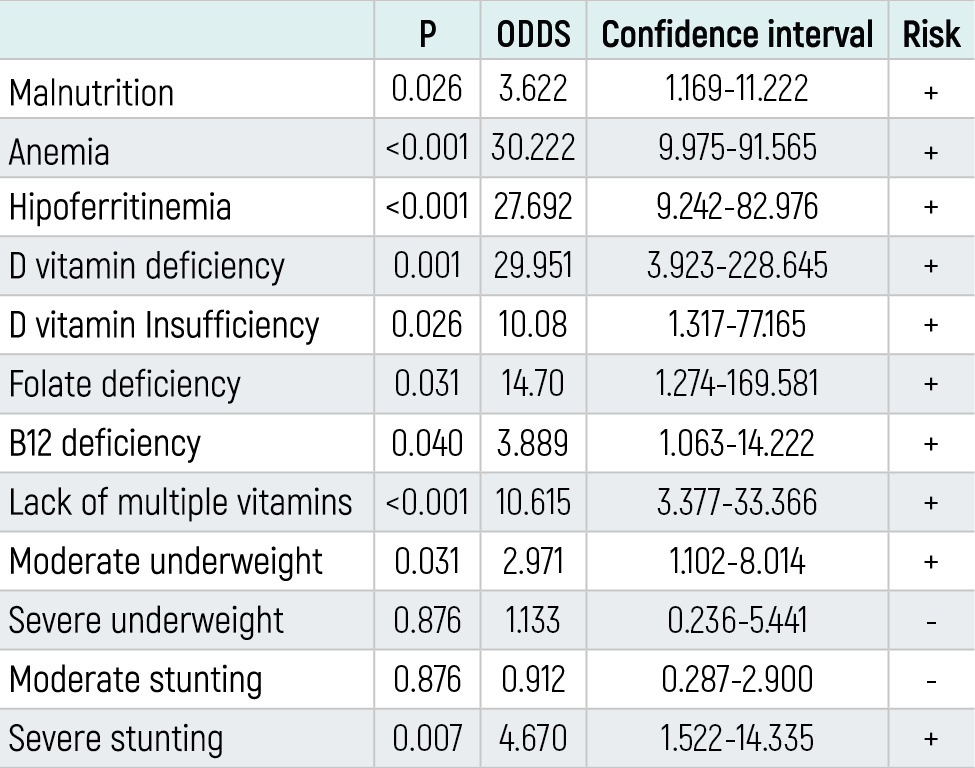
Z score (P=0,314, P=0,101, P=0,174, P=0,221, respectively) (Table 3). According to a logistic regression analysis of the risk factors potentially affecting RLS development (ODDS Ratio), the latter was 30.222 times greater in patients with anemia; 27.692 times greater in patients with hypoferritinemia; 29.951 times greater in patients with vitamin D deficiency; 10.08 times greater in patients with vitamin D insufficiency; 3.889 times greater in patients with vitamin B12 deficiency; 14.7 times greater in patients with folate deficiency; 10.615 times greater in patients with multivitamin deficiency; and 3.622 times greater in patients with malnutrition (Table 4). Moderate underweight and severe stunting increased the risk of RLS development by respectively 2.971 and 4.670 times, whereas severe underweight, moderate stunting did not confer a significant risk for developing RLS (Table 4).
Discussion
Restless leg syndrome has no specific biochemical marker; it is diagnosed on clinical grounds. Studies on adults have suggested that symptoms started at childhood or adolescence in about a third of patients.9 Some of pediatric studies in the literature have reported a greater RLS prevalence in girls.10,11 However, as supported by our study, comprehensive epidemiological studies have denied any gender difference for RLS prevalence.12 Altunayoglu et al.13 in a domestic adult prevalence study, reported a RLS prevalence of 4.5%. A prevalence study from Kayseri province showed a RLS prevalence of 2.9% among adolescents aged 13-16 years.14 We demonstrated a RLS prevalence of 5.7% among control patients and 18% in malnutrition patients. We linked our higher RLS prevalence than the literature reports to a smaller sample size, accompanying iron and vitamin deficiencies, and malnutrition.
Although Vito et al.15 reported that RLS prevalence was two times more common in the overweight group compared to the normo-weight group, that difference did not reach statistical significance. In contrast, our study revealed 3.622 times more common RLS prevalence in the malnutrition group compared to the control group (P=0.026). Baran et al.16 demonstrated an increased RLS prevalence in obese adolescents than the control subjects (21.7% vs 1.5%). Our study found an increased prevalence of RLS in patients with malnutrition than the control group (18% vs 5.7%, P=0,001). We attributed that difference to a higher prevalence of factors like anemia, iron, and vitamin deficiencies which could alter RLS prevalence among patients with malnutrition. We also noted that vitamin and iron levels that could affect RLS prevalence were not questioned in detail in the majority of studies reporting that obesity increases RLS prevalence.15,16,17 Moccia et al.18 reported that it increased RLS prevalence further among patients with coeliac disease (31% vs 4%), and although there was no significant correlation between RLS and iron metabolism, anemia was more common in patients with coeliac disease and RLS compared to those with coeliac disease but no RLS (P=0.003). Işıkay et al.2 found RLS prevalence as low as 3% in the coeliac group but reported a significant negative correlation between RLS severity and serum ferritin, folate, and vitamin D levels. Our work, on the other hand, found that anemia, low ferritin level, vitamin D deficiency, folate deficiency, and multivitamin deficiency were significantly more common in the RLS group than the control group (P<0.001, P<0.001, P<0.001, P=0.044, P<0.001, respectively). There was no significant difference between both groups with regard to vitamin B12 deficiency (18.2% vs 5.4%, P=0.052). Iron, a cofactor of the enzyme tyrosine hydroxylase necessary for dopamine production, has an important role for RLS pathophysiology; dopaminergic drugs are known to be used for RLS treatment with favorable results being attained in some patients.19,20 Previous studies indicated a negative correlation between iron deficiency, serum ferritin level and RLS symptom severity.21,22 We similarly demonstrated that lower serum ferritin level increased RLS development risk by 27.692 folds (P<0.001) while anemia increased it by 30,222 times (P<0.001). Literature data related to folic acid and RLS are generally limited to adult studies. Lee et al.23 reported that folic acid levels were lower in patients with RLS compared to those without. Işıkay et al.2 reported a negative correlation between folic acid level and RLS severity. There are also several studies in the literature suggesting that there is no significant difference between RLS patients and controls with respect to folic acid level.13,24 Our work revealed a significantly lower serum folic acid level in RLS patients than controls (9.1% vs %0.7%, P=0,044). A logistic regression analysis showed that folic acid deficiency increased RLS risk by 14.7 folds (P=0. 031). In a study on adult patients with musculoskeletal symptoms, vitamin D deficiency was found significantly more common in RLS patients, with vitamin D deficiency increasing RLS risk by 5-fold.25 Another study reported a significant negative correlation between vitamin D levels and RLS.2 Our study, in line with the previous studies, demonstrated that RLS prevalence was significantly higher among patients with vitamin D deficiency (p<0.001) and that RLS risk increased by 29.951 folds among patients with vitamin D deficiency (p=0.001). We also found that moderate malnutrition and severe stunting increased the risk of RLS (2.971 times P = 0.031 and 4.670 times P = 0.007, respectively). The limitations of our study include the lack of investigation of sociodemographic properties among correctable causes of malnutrition, as well as of the effects of RLS on sleep-wakefulness. Additionally, RLS prevalence was higher in our study than the normal population, which we attributed to a small sample size, accompanying iron and vitamin deficiencies, and malnutrition. However, to the best of our knowledge, the importance of our study stems from its status of being the only study investigating the relationship between malnutrition due to low intake and RLS among pediatric patients. In conclusion, RLS is an important, prevalent condition in the general population, which impairs sleep quality and affects social life in an unfavorable manner. Our study supports the notion that malnutrition, anemia, and vitamin deficiencies, as correctable causes, increase the prevalence of RLS.
Declarations
Animal and Human Rights Statement
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional research committee and the Declaration of Helsinki.
Informed Consent
Written informed consent was obtained from all participants and/or their parents prior to inclusion in the study.
Conflict of Interest
The authors declare no conflict of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the scientific content of the article, including study design, data collection, analysis and interpretation, manuscript preparation, and approval of the final version of the manuscript.
References
-
Chokroverty S. Editor’s corner: restless leg syndrome, a common disease uncommonly diagnosed. Sleep Med. 2003;4(2):91-93. doi:10.1016/s1389-9457(03)00008-x
-
Işıkay S, Işıkay N, Per H, Çarman KB, Kocamaz H. Restless leg syndrome in children with celiac disease. Turk J Pediatr. 2018;60(1):70-75. doi:10.24953/turkjped.2018.01.010
-
Allen RP, Picchietti DL, Garcia-Borreguero D, Ondo WG, Walters AS, Winkelman JW, et al. Restless legs syndrome/Willis-Ekbom disease diagnostic criteria: updated International Restless Legs Syndrome Study Group (IRLSSG) consensus criteria—history, rationale, description, and significance. Sleep Med. 2014;15(8):860-873. doi:10.1016/j.sleep.2014.03.025
-
Holick MF, Binkley NC, Bischoff-Ferrari HA, Gordon CM, Hanley DA, Heaney RP, et al. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011;96(7):1911-1930. doi:10.1210/jc.2011-0385
-
Yao Y, Fu S, Zhang H, Li N, Zhu Q, Zhang F, et al. The prevalence of depressive symptoms in Chinese longevous persons and its correlation with vitamin D status. BMC Geriatr. 2018;18(1):198. doi:10.1186/s12877-018-0886-0
-
Short MW, Domagalski JE. Iron deficiency anemia: evaluation and management. Am Fam Physician. 2013;87(2):98-104.
-
Sezer RG, Bozaykut A, Akoğlu HA, Özdemir GN. The efficacy of oral vitamin B12 replacement for nutritional vitamin B12 deficiency. J Pediatr Hematol Oncol. 2018;40(2):e69-e72. doi:10.1097/mph.0000000000001037
-
Zeeshan F, Bari A, Farhan S, Jabeen U, Rathore AW. Correlation between maternal and childhood vitamin B12, folic acid and ferritin levels. Pak J Med Sci. 2017;33(1):162-166. doi:10.12669/pjms.331.10998
-
Durmer JS. Restless legs syndrome, periodic leg movements and periodic limb movement disorder. In: Sheldon SH, Ferber R, Kryger MH, Gozal D, eds. Principles and practice of pediatric sleep medicine. Saunders/Elsevier; 2014:337-350. doi:10.1016/b978-1-4557-0318-0.00043-7
-
Picchietti DL, Picchietti MA. Restless legs syndrome. In: Kothare SV, Kotagal S, eds. Sleep in childhood neurological disorders. Demos Medical; 2011:57-70.
-
Xue R, Liu G, Ma S, Yang J, Li L. An epidemiologic study of restless legs syndrome among Chinese children and adolescents. Neurol Sci. 2015;36(9):971-976. doi:10.1007/s10072-015-2206-1
-
Picchietti D, Allen RP, Walters AS, Davidson JE, Myers A, Ferini-Strambi L. Restless legs syndrome: prevalence and impact in children and adolescents—the Peds REST study. Pediatrics. 2007;120(2):253-266. doi:10.1542/peds.2006-2767
-
Altunayoglu Cakmak V, Koc B, Nuhoglu I, Topbas M, Ucuncu SY, Deger O, et al. Prevalence of restless legs syndrome in Trabzon in the northeast Black Sea region of Turkey: comorbidities, socioeconomic factors and biochemical parameters. Neurol Res. 2015;37(9):751-762. doi:10.1179/1743132815y.0000000058
-
Per H, Günay N, İsmailoğulları S, Öztop DB, Günay O. Determination of restless legs syndrome prevalence in children aged 13–16 years in the provincial center of Kayseri. Brain Dev. 2018;40:256-257. doi:10.1016/j.braindev.2017.08.007
-
De Vito K, Li Y, Batool-Anwar S, Ning Y, Han J, Gao X. Prospective study of obesity, hypertension, high cholesterol, and risk of restless legs syndrome. Mov Disord. 2014;29(8):1044-1052. doi:10.1002/mds.25860
-
Baran RT, Atar M, Pirgon Ö, Filiz S, Filiz M. Restless legs syndrome and poor sleep quality in obese children and adolescents. J Clin Res Pediatr Endocrinol. 2018;10(2):131-138. doi:10.4274/jcrpe.5165
-
Gao X, Schwarzschild MA, Wang H, Ascherio A. Obesity and restless legs syndrome in men and women. Neurology. 2009;72(14):1255-1261. doi:10.1212/01.wnl.0000345673.35676.1c
-
Moccia M, Pellecchia MT, Erro R, Zingone F, Marelli S, Barone DG, et al. Restless legs syndrome is a common feature of adult celiac disease. Mov Disord. 2010;25(7):877-881. doi:10.1002/mds.22903
-
Jellen LC, Lu L, Wang X, Unger EL, Earley CJ, Allen RP, et al. Iron deficiency alters expression of dopamine-related genes in the ventral midbrain in mice. Neuroscience. 2013;252:13-23. doi:10.1016/j.neuroscience.2013.07.058
-
Nagandla K, De S. Restless legs syndrome: pathophysiology and modern management. Postgrad Med J. 2013;89(1053):402-410. doi:10.1136/postgradmedj-2012-131634
-
Sun ER, Chen CA, Ho G, Earley CJ, Allen RP. Iron and the restless legs syndrome. Sleep. 1998;21(4):371-377. doi:10.1093/sleep/21.4.381
-
Rizzo G, Manners D, Testa C, Tonon C, Vetrugno R, Marconi S, et al. Low brain iron content in idiopathic restless legs syndrome patients detected by phase imaging. Mov Disord. 2013;28(13):1886-1890. doi:10.1002/mds.25576
-
Lee KA, Zaffke ME, Baratte-Beebe K. Restless legs syndrome and sleep disturbance during pregnancy: the role of folate and iron. J Womens Health Gend Based Med. 2001;10(4):335-344. doi:10.1089/152460901750269652
-
Vahdat M, Sariri E, Miri S, Rohani M, Kashanian M, Sabet A, et al. Prevalence and associated features of restless legs syndrome in a population of Iranian women during pregnancy. Int J Gynaecol Obstet. 2013;123(1):46-49. doi:10.1016/j.ijgo.2013.04.023
-
Oran M, Unsal C, Albayrak Y, Tulubas F, Oguz K, Avci O, et al. Possible association between vitamin D deficiency and restless legs syndrome. Neuropsychiatr Dis Treat. 2014;10:953-958. doi:10.2147/ndt.s63599
Tables
Table 1. Evaluation of clinical and laboratory features of malnourished patients according to control group

RLS: Restless legs syndrome
Table 2. Evaluation of clinical and laboratory findings of patients with and without RLS
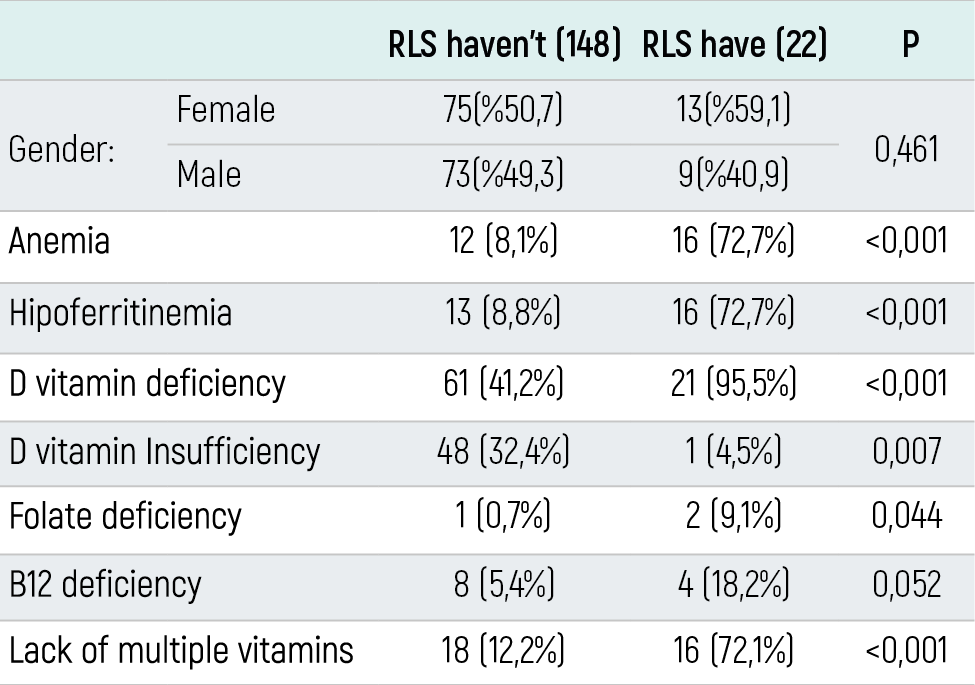
Table 3. Evaluation of the differences between the anthropometric measurements and laboratory parameters of the patients with and without RLS.
RLS: Restless legs syndrome, WBH: Weight by height, BMI: Body mass index
Table 4. Evaluation of factors that may affect RLS development by logistic regression analysis
RLS: Restless legs syndrome
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Şükrü Güngör, Serkan Kırık. Effects of nutrient deficiencies on the development of restless leg syndrome in pediatric patients with primary malnutrition. Eu Clin Anal Med 2020;8(2):7-11. doi:10.4328/ECAM.10020
- Received:
- January 24, 2020
- Accepted:
- February 13, 2020
- Published Online:
- February 20, 2020
- Printed:
- May 1, 2020