Isolated pituitary stalk duplication
Pituitary stalk duplication
Authors
Abstract
IntroductionPituitary duplication is a rare anomaly with about 40 cases reported to date.
Case PresentationThe duplication of the pituitary stalk with a single gland is an exceptionally rare manifestation with only a few case reports in the current literature. Although incidentally discovered cases of pituitary duplication have been reported, patients with this disorder usually present with endocrine disturbance(s) regarding the adenohypophyseal axis and/or with accompanying pathologies such as median cleft face syndrome, craniocervical bony abnormalities, tuberomammillary/ pituitary mass(es) or various ocular and vascular disorders. Cross-sectional imaging modalities play a key role in the comprehensive evaluation of these patients.
ConclusionHere, we present a 12-year-old boy who presented with growth retardation and showed pituitary stalk duplication without a duplicated gland or associated findings
Keywords
Introduction
The pituitary gland and stalk develop from the primordium which can be distinguished on the 22nd day of gestation. The gland forms as a single structure from neural ectoderms that are tightly adhered to each other prior to the pituitary evagination. Although various mechanisms have been proposed to explain why and how pituitary duplication occurs in some cases, the exact cause remains unknown.1 The duplication may occur at different embryonic stages, and the scope of the presentation may vary depending on the stage at which the duplication occurs. Several cases of pituitary gland duplication have been reported to date. And the vast majority of these cases were accompanied by additional abnormalities such as tuberomammillary or pituitary mass, various craniofacial midline defects or some ophthalmological pathologies.1,2,3 However, cases of pituitary stalk duplication with a nonduplicated pituitary gland are extremely rare in the current literature.4,5,6 Here, we present a 12-year-old boy with isolated pituitary stalk duplication who presented with growth retardation.
Case Presentation
12-year-old boy with a complaint of short stature was admitted to the hospital. His height was 119 cm, weight was 21 kg and bone age was 8 years. He was the only child of non-consanguineous healthy parents and the family history was unremarkable. He was delivered at term following an uneventful pregnancy. Except for the developmental delay, his medical history was unremarkable. No dysmorphic facial features were noted on physical examination. Neurological and ophthalmological examinations were normal. Endocrine laboratory tests revealed low serum growth hormone (GH) and insulin-like growth factor 1 (IGF-1) [22 ng/ ml (normal range 93-567 ng/ml)] levels. Insulin tolerance test -as a GH stimulation test- revealed a low GH [2.1µg/L (normal>5 µg/L] level. A slightly increased serum prolactin level [3.8 ng/mL (normal range 4.8–23.3 ng/mL)] was also noted. Thyroid function tests, luteinizing hormone (LH), follicle-stimulating hormone (FSH), cortisol and electrolytes were all within normal ranges. Brain magnetic resonance imaging (MRI) revealed marked anterior pituitary hypoplasia. Pituitary stalk duplication and the downward extension of the third ventricle into the pituitary fossa via the split in the hypothalamus were also evident in the sagittal T1-weighted magnetic resonance image (Figure 1). Coronal T1- and T2-weighted magnetic resonance images nicely delineated the duplicated pituitary stalks and the split in the hypothalamus (Figure 2). No additional brain malformation was detected on MRI. Computed tomography (CT) of the head and cervical vertebrae revealed no craniocervical bony pathology.
Based on the clinical, laboratory and imaging findings, the patient was diagnosed with GH deficiency as the result of anterior pituitary hypoplasia and duplicated pituitary stalk. A GH replacement therapy was started and close monitoring of the endocrine functions was planned. Informed consent for publication was obtained from the patient.
Discussion
Pituitary duplication is a rare anomaly with about 40 cases reported to date.2 And the duplication of the pituitary stalk with a single gland is an exceptionally rare manifestation with only a few case reports in the current literature.4,5,6 The duplication of the pituitary gland and stalk seems to be two forms of the same disorder which are in continuation with each other and differ in terms of the embryonal stage at which the neural development interrupted. Although many factors such as prenatal exposure to teratogens, the inclusion of a dermoid in the midline, or various genetic disorders have been accused of giving rise to this rare embryonal disorder, the exact cause has not yet been clarified.1,2,3,4,5,6 Genetic causes of pituitary developmental anomalies, including pituitary duplication, have extensively been studied over the last few years.6,7,8 Recently, ROBO1 novel heterozygous variants have been reported in patients with pituitary stalk interruption syndrome.8 Further, Scala et al. reported a case of familial ROBO1 deletion associated with duplication of the pituitary stalk, anterior pituitary hypoplasia, and ectopic posterior pituitary.7 The pituitary imaging findings and endocrine laboratory results of the patient reported by Scala et al. were very similar to those of the patient we currently present. However, in the case reported by Scala et al., both the patient and the patient’s father showed facial dysmorphic features unlike in our case. Unfortunately, because the patient’s family did not give consent, genetic counseling could not be performed in our case. However, as recommended by Scala et al., investigation of ROBO1 haploinsufficiency in patients with congenital pituitary anomalies would add much to the existing information on the etiological mechanism of the pituitary duplication.
Although incidentally discovered cases of pituitary duplication have been reported,3 patients with this disorder usually present with endocrine disturbance(s) regarding the adenohypophyseal axis and/or with accompanying pathologies. According to the previous reports, median cleft face syndrome, skull base or cervical bony clefts or duplications, agenesis or hypoplasia of corpus callosum, sellar duplication, widened optic chiasm, tuberomammillary or pituitary mass, moya moya disease and morning glory disc anomaly can accompany pituitary duplication.1,2,3,4,5,6,7 Cross-sectional imaging modalities play a key role in the comprehensive evaluation of these patients. Craniofacial and cervical bony disorders can be demonstrated in detail, using multiplanar CT.3 And MRI is the method of choice for the assessment of the brain, orbita and vascular pathologies.9 Using conventional MRI sequences, we clearly demonstrated the hypoplastic adenohypophysis and double pituitary stalks. Brain MRI and craniocervical CT studies revealed no additional pathologies in our patient. To our knowledge, this is the first case report of pituitary stalk duplication without a duplicated gland or associated findings.
The management of the patients with pituitary duplication varies according to the clinical presentation, hormone profile and the presence or absence of the additional pathologies. Rapid hormone replacement therapy and close monitoring of endocrine functions are critical in patients presenting in childhood with hormone deficiencies and developmental delay.7 In addition, detailed neurological, ophthalmologic, and neuroradiological evaluation and follow-up are necessary to avoid missing a concomitant pathology in these patients.1
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. No animal or human studies were carried out by the authors for this article.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
None of the authors received any type of financial support that could be considered potential conflict of interest regarding the manuscript or its submission.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content including study design, data collection, analysis and interpretation, writing, some of the main line, or all of the preparation and scientific review of the contents and approval of the final version of the article.
References
-
Loddenkemper T, Friedman NR, Ruggieri PM, Marcotty A, Sears J, Traboulsi EI. Pituitary stalk duplication in association with moya moya disease and bilateral morning glory disc anomaly-roadening the clinical spectrum of midline defects. J Neurol. 2008;255(6):885-90. doi:10.1007/s00415-008-0799-5
-
Slavotinek A, Parisi M, Heike C, Hing A, Huang E. Craniofacial defects of blastogenesis: duplication of pituitary with cleft palate and orophgaryngeal tumors. Am J Med Genet A. 2005;135(1):13–20. doi:10.1002/ajmg.a.30694
-
Usta Y, Sakha F, White WL, Little AS, Knecht L. Duplicated pituitary gland and odontoid process. A case report. Neuroradiol J. 2012;25(3):360-3. doi:10.1177/197140091202500312
-
Madhusudhan KS, Kandpal H. Pituitary stalk duplication with intrasellar dermoid and herniation of the third ventricle. Pediatr Radiol. 2009;39(9):1013. doi:10.1007/s00247-009-1198-5
-
Petridis AK, Barth H. Pituitary stalk duplication in ventral-dorsal direction in a patient with pituitary gland adenoma and aqueductal stenosis. Clin Anat. 2010;23(8):879-80. doi:10.1002/ca.21030
-
Accornero S, Danesino C, Bastianello S, D’Errico I, Guala A, Chiovato L. Duplication of the pituitary stalk in a patient with a heterozygous deletion of chromosome 14 harboring the thyroid transcription factor-1 gene. J Clin Endocrinol Metab. 2010;95(8):3595-6. doi:10.1210/jc.2010-0621
-
Scala M, Accogli A, Allegri AME, Tassano E, Severino M, Morana G, et al. Familial ROBO1 deletion associated with ectopic posterior pituitary, duplication of the pituitary stalk and anterior pituitary hypoplasia. J Pediatr Endocrinol Metab. 2019;32(1):95-99. doi:10.1515/jpem-2018-0272
-
Bashamboo A, Bignon-Topalovic J, Moussi N, McElreavey K, Brauner R. Mutations in the human ROBO1 gene in pituitary stalk interruption syndrome. J Clin Endocrinol Metab. 2017;102(7):2401–6. doi:10.1210/jc.2016-1095
-
Shields R, Mangla R, Almast J, Meyers S. Magnetic resonance imaging of sellar and juxtasellar abnormalities in the paediatric population: an imaging review. Insights Imaging. 2015;6(2):241-60. doi:10.1007/s13244-015-0401-5
Figures
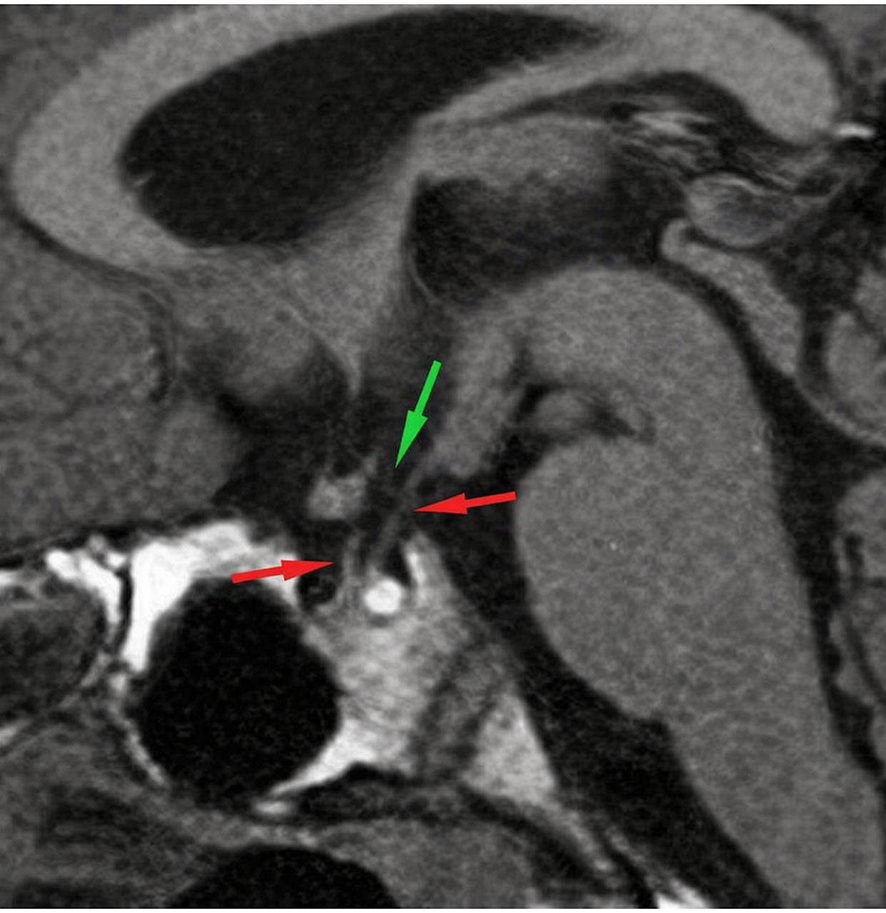
Figure 1. Pituitary duplication is a rare anomaly with about 40 cases reported to date.[2] And the duplication of the pituitary stalk with a single gland is an exceptionally rare manifestation with only a few case reports in the current literature.[4-6] The duplication of the pituitary gland and stalk seems to be two forms of the same disorder which are in continuation with each other and differ in terms of the embryonal stage at which the neural development interrupted. Although many factors such as prena tal exposure to teratogens, the inclusion of a dermoid in the midline, or various genetic disorders have been accused of giving rise to this rare embryonal disorder, the exact cause has not yet been clarified.[1-6] Genetic causes of pituitary developmental anomalies, including pitu itary duplication, have extensively been studied over the last few years.[6-8] Recently, ROBO1 novel heterozygous variants have been reported in patients with pituitary stalk interruption syndrome.[8] Further, Scala et al. reported a case of familial ROBO1 deletion associated with dupli cation of the pituitary stalk, anterior pituitary hypoplasia, and ectopic posterior pituitary.[7] The pituitary imaging findings and endocrine lab oratory results of the patient reported by Scala et al. were very similar to those of the patient we currently present. However, in the case re ported by Scala et al., both the patient and the patient’s father showed facial dysmorphic features unlike in our case. Unfortunately, because the patient’s family did not give consent, genetic counseling could not be performed in our case. However, as recommended by Scala et al., investigation of ROBO1 haploinsufficiency in patients with congenital pituitary anomalies would add much to the existing information on the etiological mechanism of the pituitary duplication. Although incidentally discovered cases of pituitary duplication have been reported [3], patients with this disorder usually present with endocrine disturbance(s) regarding the adenohypophyseal axis and/ or with accompanying pathologies. According to the previous reports, median cleft face syndrome, skull base or cervical bony clefts or dupli cations, agenesis or hypoplasia of corpus callosum, sellar duplication, widened optic chiasm, tuberomammillary or pituitary mass, moya moya disease and morning glory disc anomaly can accompany pituitary du plication.[1-7] Cross-sectional imaging modalities play a key role in the comprehensive evaluation of these patients. Craniofacial and cervical bony disorders can be demonstrated in detail, using multiplanar CT.[3] And MRI is the method of choice for the assessment of the brain, or bita and vascular pathologies.[9] Using conventional MRI sequences, we clearly demonstrated the hypoplastic adenohypophysis and double pituitary stalks. Brain MRI and craniocervical CT studies revealed no additional pathologies in our patient. To our knowledge, this is the first case report of pituitary stalk duplication without a duplicated gland or associated findings. The management of the patients with pituitary duplication varies ac cording to the clinical presentation, hormone profile and the presence or absence of the additional pathologies. Rapid hormone replacement therapy and close monitoring of endocrine functions are critical in pa tients presenting in childhood with hormone deficiencies and devel opmental delay.[7] In addition, detailed neurological, ophthalmologic, and neuroradiological evaluation and follow-up are necessary to avoid missing a concomitant pathology in these patients.[1]

Figure 2. A 12-year-old boy who presented with the complaint of short stature. (a) Coronal T1-weighted magnetic resonance image shows duplicated pituitary stalks (red arrows), a split in the hypothalamus (blue arrows) and the passage in the hypothalamus where the third ventricle extends into the pituitary fossa (green arrow). (b) Coronal T2-weighted magnetic resonance image shows duplicated pituitary stalks (red arrows), a split in the hypothalamus (blue arrows) and the passage in the hypothalamus where the third ventricle extends into the pituitary fossa (green arrow).
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Meltem Özdemir, Rasme Pelin Kavak, Begüm Demirler Şimşir, Tuba Akda, Esra Soyer Güldoğan. Isolated pituitary stalk duplication. Eu Clin Anal Med 2020;8(1):4-6. doi:10.4328/ECAM.10019
- Received:
- January 6, 2021
- Accepted:
- January 6, 2020
- Published Online:
- February 3, 2020
- Printed:
- January 1, 2020