Aberrant internal carotid artery presenting as oropharyngeal mass
Oropharyngeal mass-aberrant ICA
Authors
A 52 years old male presented to us with complaints of throat discomfort and foreign body sensation for 2 years. The patient did not report of any other upper aerodigestive tract symptoms. There was no history of addiction or any other comorbidities and patient was in a good general state of health. On examination, the patient was found to have a globular pulsatile, non-tender swelling involving left side oropharynx and tonsillar fossa region. On laryngoscopic examination, endolarynx was found to be within normal limits. The general systemic examination was within normal limits. A contrast-enhanced CT scan was ordered and showed a markedly tortuous internal carotid artery on the left side reaching till midline (Figure 1). The patient was reassured after explaining the condition and advised for further follow up as needed.
The ICA normally rotates gradually and smoothly, first laterally and then posteromedially in relation to the ECA after its origin from the carotid bifurcation and then runs a straight course to the carotid canal.1 The normal tonsillo-carotid distance varies with age and is usually around 25 mm in adults.2 Pronounced anatomical aberrations involving the extracranial internal carotid artery (ICA) have been described to be present in 5-6% of the general population.3 The significance of such occurrence resides in clinical symptomatology from positional central hypoperfusion or surgical risk from pharyngeal/ neck surgeries, although they are asymptomatic in up to 80% of cases.3 These aberrations have been classified anatomically (tortuosity, kinking or coiling)4,5 and clinico-radiologically (depending on the distance of ICA from the pharyngeal wall).1 Utmost care needs to be exercised with careful visual and palpatory examination before undertaking diagnostic and therapeutic ventures of the pharyngeal cavity
Declarations
Animal and Human Rights Statement
No animal experiments were performed. All procedures involving the human participant were conducted in accordance with institutional and ethical standards.
Informed Consent
Written informed consent was obtained from the patient for publication of this Clinical Image and accompanying images.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the scientific content of the article, including study design, data collection, analysis and interpretation, manuscript preparation, and approval of the final version of the manuscript.
References
-
Leipzig TJ, Dohrmann GJ. The tortuous or kinked carotid artery: pathogenesis and clinical considerations. Surg Neurol. 1986;25:478-486. doi:10.1016/0090-3019(86)90087-x
-
Tillmann B, Christofides C. The “dangerous loop” of the internal carotid artery: an anatomic study. HNO. 1995;43:601-604.
-
Pfeiffer J, Ridder GJ. A clinical classification system for aberrant internal carotid arteries. Laryngoscope. 2008;118:1931-1936. doi:10.1097/mlg.0b013e318180213b
-
Metz H, Murray-Leslie RM, Bannister RG, Bull JW, Marshall J. Kinking of the internal carotid artery. Lancet. 1961;1:424-426. doi:10.1016/s0140-6736(61)90004-6
-
Weibel J, Fields WS. Tortuosity, coiling, and kinking of the internal carotid artery. I. Etiology and radiographic anatomy. Neurology. 1965;15:7-18. doi:10.1212/wnl.15.1.7
Figures
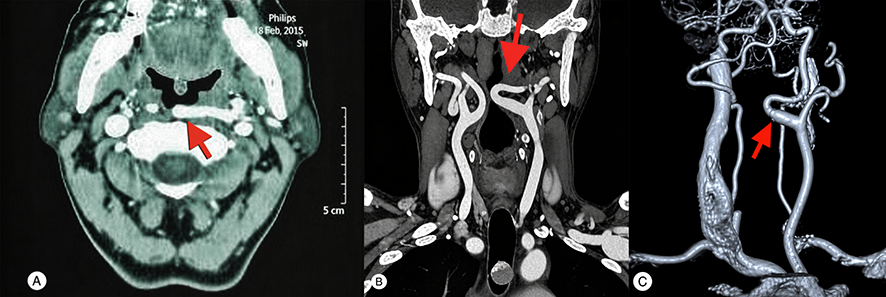
Figure 1. Contrast CT (A) Axial, (B) Coronal and (C) angiographic film showing tortuous medialized left internal carotid artery reaching till midline (red arrow).
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
- Received:
- October 31, 2018
- Accepted:
- October 16, 2018
- Published Online:
- January 14, 2019
- Printed:
- January 14, 2019