Umbilical discharge in neonates: a case-based management protocolperformed from a different perspective
Wet umbilicus, our approach
Authors
Abstract
AimThis study aimed to retrospectively investigate causes of umbilical discharge (UD), its clinical course, treat ment modalities and follow-up in infants with UD complaints in a major teaching hospital in Turkey.
MethodsInfants with an UD complaint who were referred to our clinic by a pediatrician or a family physician from January 2013 to June 2014 were investigated.
ResultsThe study included 291 infants between the ages of 3 and 114 days. Of these infants, 194 (67%) had an umbilical granuloma, 83 (28.3%) had an umbilical polyp, and 14 (4.8%) had omphalitis. Among 14 infants with omphalitis who were treated with topical antibiotics, six infants had refractory or recurrent discharge and ultrasonography (US) was performed which revealed a 1-3 mm sized cystic appearance with no connection to the peritoneum or other tissues. These infants received systemic antibiotics in addition to topical antibiotics. During the follow-up period, cystic appearance was not present in US in three of these six patients and in the remaining three patients who did not present for follow-up we learned via phone calls that their complaints had not recurred.
ConclusionCauterization using a silver nitrate pencil was sufficient in the umbilical granuloma. Ligating, excising and cauterizing the base of the lesions was sufficient in an umbilical polyp. In cases with persistent or recurrent UD, high-resolution US should be primarily performed, which may direct the subsequent management.
Keywords
Introduction
The umbilical cord is generally separated by the third day after birth leaving a characteristic depressed scar.1 Epithelization in this area should normally occur within two or three days. Persistent discharge 3-5 days after the separation of the umbilical cord suggests the presence of granuloma, polyp, omphalitis, and omphalomesenteric duct (OMD) and urachal canal remnants.2 Any retained umbilical cord elements may lead to umbilical abnormalities; discharge, inflammation, a palpable mass or a hernia,either alone or in combination, may be the clinical presentations of these abnormalities.3 Deep ligation and chemical cauterization are usually sufficient in the treatment of umbilical granulomas or polyps, which are the most common causes of umbilical discharge.4 However, all urachal abnormalities (urachal sinus, urachal cyst, patent urachus, and urachal diverticulum) and omphalomesenteric abnormalities (Meckel’s diverticulum, bands, cysts) require surgical intervention.5 The present study aimed to investigate the causes of umbilical discharge, its clinical course, treatment modalities and follow-up in infants presenting with the complaint of umbilical discharge.
Materials and Methods
Infants with the complaint of umbilical discharge who were referred to our clinic by a pediatrician or a family practice physician from January 2013 to June 2014 were included in the present study. Infants with bleeding from the umbilicus or those in whom the umbilical cord was not detached were excluded. The Educational Planning Board of Etlik Zubeyde Hanım Women’s Health Training and Research Hospital Ankara, Turkey, ethically approved the study (#25, 02, 2016/205). Informed consents of the patients were obtained from their parents/guardians.The 1–10 mm sized sticky, and platy granulomas with a large base remaining after the detachment of the umbilical cord were cauterized using a 75% silver nitrate pencil. The umbilicus was pressurized from both sides, and a protective cream (Vazelin® - Sifa Kimya Ilac Kozmetik San. & Tic. A.S. Konya, Turkey) was applied to the intact tissue around the granuloma to prevent damage to the surrounding tissues during the cauterization process. The procedure was performed once weekly and continued for 1–3 weeks.Polyps with stems or mushroom-shaped polyps were tied and cau terized. For this purpose, the periumbilical area was cleaned with povidone-iodine solution. For pain relief, 1 h before excision, Emla® 5% cream (AstraZeneca, Turkey) was applied on the lesions as a thin layer (about 0.5 g). The area was covered with 3M™ Tegaderm™ (3M Health Care, Germany) transparent film or with an airtight substance such as a plastic wrap. A 4-0 silk suture was used for thin and fragile polyps, and a 3-0 silk suture was used for thick polyps; the polyps were tied at the radix. The polyp materials with larger bases and darker colors were sent to the pathology department for histopathological evaluation. For infants with omphalitis in whom skin hyperemia and oedema were present within the umbilical area, their parents/guardians were suggested to apply a topical antibiotic cream twice a day using cotton swabs. In addition to the local treatment, systemic antibiotic treatment was commenced in infants in whom hyperemia and oedema extended further and who had purulent and bloody discharge from the umbilicus. These patients were hospitalized for treatment. The infants in whom omphalitis findingsdid not resolve or recurred underwent ultrasonography (US) for a potential regional pathology.
Results
During the study period, 671 infants were referred to our clinic with the complaint of discharge from the umbilicus. Of these, 201 infants with bleeding from the umbilicus and 179 in whom the umbilicus was not detached were excluded from the study. Thus, a total of 291 patients were included in the present study.The age of the infants ranged between 3 and 114 days (mean age, 23 days). Of these infants, 31 (10.6%) were premature. The mean time of umbilical cord detachment was 7.2 days. An umbilical granuloma was found in 194 (67%) infants, and an umbilical polyp was found in 83 (28.3%) infants. Omphalitis was found in 14 (4.8 %) infants. In six infants (2%) with refractory or recurrent omphalitis symptoms, a 1-3 mm sized cystic appearance was detected in ultrasonographical (US) examination. In these infants, the umbilical discharge stopped following administration of local and systemic antibiotic treatments. During the follow-up period, three of these six patients underwent a control US examination, and the cystic appearance was found to disappear. The other three infants were reached via phone calls, and it was learned that the complaints did not recur. Histopathological evaluation performed in 23 infants with larger based or darker colored polyps revealed the presence of gastric and/or small bowel mucosa. The details of and the scheme of the procedures performed in our cases are presented in Table 1 and Figure 1. The longest symptom-free follow-up period was 26 months. No cases of umbilical fasciitis or gangrene were observed. On US, no anomaly such as OMD or patent urachus was noted.
Discussion
In our study, the umbilical cord was determined to be detached from its base on an average of 7.2 days. These values are very different from those for infants without any umbilical problems.1 The reason could be that infants in this study may have recurrent umbilical problems because almost all infants admitted to our clinic showed the pathology of late separation of the umbilical cord or inflammation or underlying problems of the umbilicus. The umbilical granuloma is the most common cause of a discharge from the umbilicus.6 It is not a congenital defect; it shows persistent inflammation of the granulation tissue, which has not yet epithelialized.4 Umbilical granuloma presents as a round, pedunculated, wet, and generally pink lesion that varies in size (usually from 3 to 10 mm).4 Granulation tissue generally responds to treatment with silver nitrate (75%). Another treatment option includes cryosurgery.2 If no response is obtained after two attempts of silver nitrate treatment, surgical excision may be required. Regarding surgery, some authors recommend double ligature technique in order to avoid burns during cauterization and to decrease complicationsrate.2 In our series, the incidence of granuloma was consistent with the published medical literature. We received a satisfactory, complication-free response to our cauterization treatment; moreover, no surgical excision was necessary in any of our granuloma cases.Following granulomas, the second leading cause of discharge, particularly mucus, from the umbilicus is the umbilical polyp.5 Umbilical polyps are small-sequestrated shiny, spherical, bright red or pink nodules
that contain ectopic alimentary mucosa.1 Controversial approaches are present regarding the management of umbilical polyps. Some authors have suggested that simple topical application of silver nitrate on one or two occasions is usually all that is needed to get rid of the alimentary epithelium.7 whereas others have suggested surgical removal combined with peritoneal exploration for the presence of OMD.8 Pacili et al.9 investigated 13 patients with umbilical polyps considering the need for peritoneal cavity exploration for the presence of OMD. However, they detected no anomaly in six patients undergoing peritoneal cavity exploration for suspicious OMD anomaly and reported that the remaining seven patients not undergoing peritoneal cavity exploration were asymptomatic during the mean 5.8 years of follow-up; therefore, Pacili et al.9 concluded in their report that the presence of an umbilical polyp was usually accompanied with the absence of OMD anomalies, removal of the umbilical polyp was mostly sufficient, and exploration of the peritoneal cavity was not required in children with an umbilical polyp. On the other hand, the defenders of surgical exploration for OMD have considered a true polyp as an indicator for the existence of an underlying anomaly.5 Kutin et al. reported that the probability of an OMD anomaly was 30%–60% in the presence of an umbilical polyp.8 Additionally, dermoid cysts and other neoplastic lesions rarely present as an umbilical mass, although they are usually encountered in older patients. Teratoma, rhabdomyosarcoma, malignant fibrous histiosarcoma and a wide variety of rare tumors have also been reported in the umbilicus.5 They advocate surgical exploration for anomalies once the presence of intestinal mucosa at the umbilicus has been confirmed. In our series, we performed a conservative non-exploratory approach, ligation, excision and cauterizing as the first, second, and the third steps. Larger based and darker colored polyps were sent for pathological examination in 23 out of 89 cases with polyps, and the presence of alimentary mucosa was confirmed. However, this result did not change our approach towards a consecutive explorative surgery, also not advocated by the defenders of the non-surgical approach in the literatüre.7 This has raised the question of whether performing a pathological examination was not necessary at all. The cause in some neonatal cases is reported as omphalitis.10 Umbilical infections are often related to hygiene issues, which still remain an important concern in developing countries.5 Omphalitis is a polymicrobial infection in which the most commonly involved organisms are Staphylococcus aureus, group A streptococcus, Gram-negative bacteria and rarely anaerobes.4 There are various antimicrobial agents such as triple dye, bacitracin, silver sulphadiazine, povidone-iodine, chlorhexidine, and hexachlorophene, which are used for reducing colonization rates. Oral antibiotic treatment may be plausible but must be accompanied by close follow-up in patients having mild signs of inflammation but no systemic signs or symptoms.4 Although infrequent, omphalitis can rapidly progress to severe cellulitis or necrotizing fasciitis, and thus it should be treated promptly and aggressively.5 In a study in which 140 infants with omphalitis were followed up for a 20-year period, 8 infants were reported to develop polymicrobial necrotizing fasciitis.11 In our series, we observed no cases of umbilical fasciitis or gangrene. This might be an indicator of our treatment approach and follow-up being satisfactory. On the other hand, although the severity of omphalitis did not increase, some of the omphalitis cases were refractory to treatment or their symptoms recurred. In children in whom umbilical discharge complaints do not improve or recur, various investigations, including US, fistulography /sinogram, abdominal X-ray or computed tomography, can be performed to determine the underlying anomaly. Fistulography may be used to demonstrate sinus track and communicating cysts. However, cannulation and demonstration of small cysts may be difficult.6 Recently, high-resolution US has been shown to demonstrate the anatomy of the umbilical structures and has been used in excluding an associated intraperitoneal sinus or track and may prevent a mini-laparotomy; in the study by Boothroyd and Cudmore, US examination was reported to allow conservative management with good results.6 In our series, we used US in a limited manner. Only six omphalitis cases who were refractory to treatment or whose symptoms recurred and umbilical discharge reoccurred underwent US which revealed a cystic appearance with a size of 1–3 mm under the umbilicus, having no connection with other structures. US findings led us to add systemic antibiotics to the treatment regimen, and discharge stopped, and the cysts disappeared in the follow-up US examination 3 cases. The other 3 were reached via phone call, and they stated that no symptom was present. Although we did not meet any anomaly case in our limited experience with US, we also consider US to be helpful in directing the management, particularly in refractory or recurrent omphalitis cases. In our follow-up study on children, we observed that no patient required surgical intervention due to the embryonic remnant. The reason might be that pediatricians and family physicians refer all infants with umbilical discharge or umbilical pathology to our clinic. A limitation of our study is that we were not able to perform a long-term follow-up of the patients. The longest follow-up period was 26 months. We can attribute this limitation to the fact that none of our patients required surgery. Figure 2 represents a summary of the scheme for approaching the umbilical mass or discharge, which may serve as a guide in the treatment of patients with umbilical discharge and as an outline for our conclusion. In conclusion, aggressive treatment was not required in most of the infants in our study. In a large majority of our patients, umbilical granuloma was detected they responded well to silver nitrate cauterization. Umbilical polyps were the second most common formations and benefited from ligation, excision, and cauterization of their base. Additional investigations were only required in patients with umbilical discharge due to refractory omphalitis or in whom complaints recurred. The High-resolution US was particularly helpful in identifying the very small cystic appearances. Parents should be educated meticulously about the signs of infection and the need to contact a health care provider immediately in the presence of an infection. Evaluation of infants with umbilical discharge in a prospective long-term follow-up study according to the scheme suggested in our study would yield better results.
Declarations
Animal and Human Rights Statement
This study was conducted in accordance with institutional ethical standards. Ethical approval was obtained from the Educational Planning Board of Etlik Zübeyde Hanım Women’s Health Training and Research Hospital
Informed Consent
Written informed consent was obtained from the parents or legal guardians of all participants.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
None.
Scientific Responsibility Statement
The authors are responsible for the conception, design, data collection, analysis, interpretation, writing, and final approval of the manuscript.
References
-
Abhyankar A, Lander AD. Umbilical disorders. Surgery (Oxford). 2004;22:214-217. doi:10.1383/surg.22.9.214.50245
-
Lotan G, Klin B, Efrati Y. Double-ligature: a treatment for pedunculated umbilical granulomas in children. Am Fam Physician. 2002;65:2067-2068.
-
Piparsaliya S, Joshi M, Rajput N, Zade P. Patent vitellointestinal duct: a close differential diagnosis of umbilical granuloma: a case report and review of the literature. Surg Sci. 2011;2:134-136. doi:10.4236/ss.2011.23027
-
Pomeranz A. Anomalies, abnormalities, and care of the umbilicus. Pediatr Clin North Am. 2004;51:819-827. doi:10.1016/j.pcl.2004.01.010
-
Snyder CL. Current management of umbilical abnormalities and related anomalies. Semin Pediatr Surg. 2007;16:41-49. doi:10.1053/j.sempedsurg.2006.10.006
-
Boothroyd AE, Cudmore RE. Ultrasound of the discharging umbilicus. Pediatr Radiol. 1996;26:362-364.
-
Beasley SW. The umbilicus. In: Hutson JM, O’Brien M, Woodward AA, Beasley SW, eds. Jones’ clinical paediatric surgery: diagnosis and management. 6th ed. Blackwell Publishing; 2008:117-120.
-
Kutin ND, Allen JE, Jewett TC. The umbilical polyp. J Pediatr Surg. 1979;14:741-744. doi:10.1016/s0022-3468(79)80257-2
-
Pacilli M, Sebire NJ, Maritsi D, Kiely EM, Drake DP, Curry JI, et al. Umbilical polyp in infants and children. Eur J Pediatr Surg. 2007;17:397-399. doi:10.1055/s-2007-989220
-
Mshelbwala PM, Sabiu L, Chirdan LB, Ameh EA, Nmadu PT. Persistent umbilical discharge in infants and children. Ann Trop Paediatr. 2006;26:133-135. doi:10.1179/146532806x107485
-
Lally KP, Atkinson JB, Woolley MM, Mahour GH. Necrotizing fasciitis: a serious sequela of omphalitis in the newborn. Ann Surg. 1984;199:101-103. doi:10.1097/00000658-198401000-00017
Figures

Figure 1. Distribution of pathologies in the study patients and the performed procedures
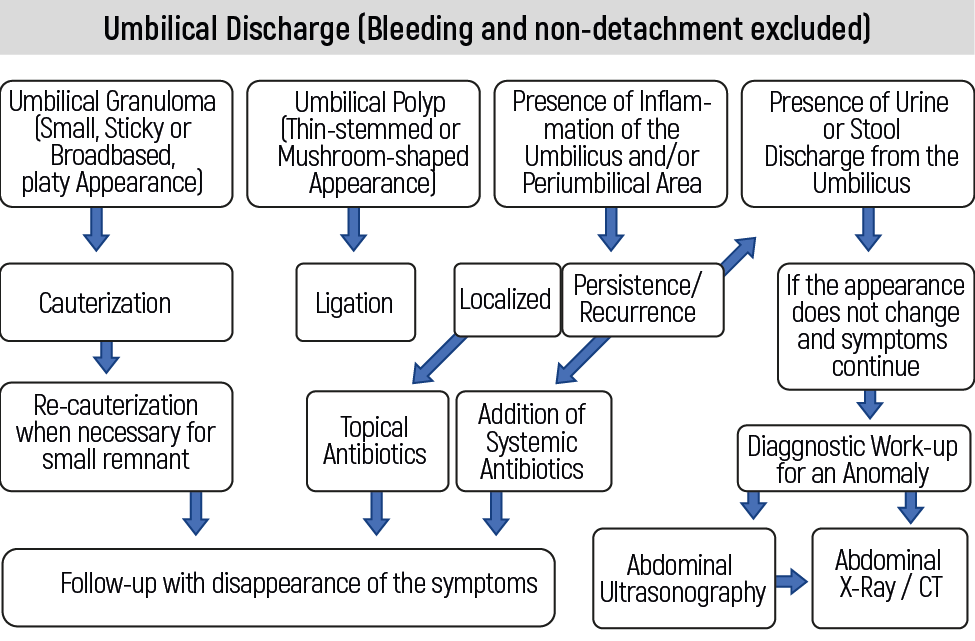
Figure 2. The suggested scheme for management of the cases with umbilical discharge. CT: computed tomography
Tables
Table 1. Distribution of the pathologies in the study patients and the performed procedures

Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Nazile Ertürk, Nihan Karaman Ayyıldız, Deniz Çavuşoğlu. Umbilical discharge in neonates: a case-based management protocolperformed from a different perspective. Eu Clin Anal Med 2018;6(3):28-31. doi:10.4328/ECAM.131
- Received:
- March 29, 2018
- Accepted:
- April 29, 2018
- Published Online:
- April 29, 2018
- Printed:
- September 1, 2018