Metastatic lung carcinoma with unknown primary site: A Case Report
Metastatic carcinoma with undefined origin
Authors
Abstract
IntroductionCarcinoma of unknown primary origin is defined as metastatic disease in which the primary tumor site is not detected despite all detailed examinations performed. CUP accounts for 3-5% of all cancer cases. The annual incidence is 7-12 in 100,000. It is the 7-8th most prevalent cancer and has the 4th highest mortality. The average age of diagnosis is 60-65 years. In children, it accounts for less than 1% of all cancers.
Case Presentation
A 71-year-old male applied to our clinic with the complaint of cough and shortness of breathduring exercise for the last 4 months. In thoracic CT, an irregularly margined, 17x27 mm diameter, mass lesion was seen in the superior part of the left lower lobe of the lung, adjacent to a fissure. Transthoracic fine needle aspiration biopsy performed on the lesion showed an adenocarcinoma. PET-CT showed no metastatic lesion and the patient was operated on.
ConclusionThe pathology report showed a metastatic character of the tumor, yet the primary origin could not be detected.
Keywords
Introduction
Carcinoma of unknown primary origin (CUP) is defined as metastatic disease in which the primary tumor site is not detected despite all detailed examinations and examinations performed.1 CUP accounts for 3-5% of all cancer cases. The annual incidence is 7-12 in 100,000. It is the 7-8th most prevalent cancer and has the 4th highest mortality. The average age of diagnosis is 60-65 years. In children, it accounts for less than 1% of all cancers.2 Primary tumors can be detected during the course of the disease in 20-30% of cases. With autopsy this ratio can reach 50-75%, yet in 30-40% of cases the primary origin remains unknown. In CUP, despite all the available treatments, the median survival time is bleak at 4-12 months. Fewer than 50% of patients live longer than 1 year. The 5-year-survival rate is reported in various series as between 6-10%.3,4 The most common symptom of CUP is pain (80%). Other signs that have been reported are lymphadenopathy, pathological fractures, masses in lungs and other abdominal findings, respiratory findings, weight loss, and skin nodules.1 The first step in the diagnosis of primary tumor is anamnesis and comprehensive physical examination. Specific immunohistochemical and histopathological evaluations of the obtained material are important in determining the primary origin. Diagnostic procedures include complete blood count,biochemistry, tumor markers, complete urine analysis, occult blood in the stool, thorax-abdomen-pelvic CT or MRI, mammography and ultrasonography, PET-CT, and endoscopy.2 The most common encountered type in CUP is adenocarcinoma (80%), yet squamous cell carcinomas and undifferentiated carcinomas are also frequently detected histopathological types.5 Adenocarcinomas, squamous cell carcinomas, or poorly differentiated carcinomas are frequently included in the evaluation of patients with single, small, and removable metastases, with varying degrees of differentiation. These patients are diagnosed with single metastatic lesions in various areas such as brain, lung, liver, bone, lymph node, adrenal gland, or skin. Radiotherapy can be applied according to the indications after local excision.5,6
Case Presentation
Case ReportA 71-year-old male applied to our clinic with the complaint of cough and shortness of breath during exercise for the last 4 months. The patient had a known cerebrovascular disease history. He had a smoking history of 30 pack-years but had not smoked for 10 years. On physical examination, respiratory voices were decreased bilaterally. No pathology was found in other systemic examinations. BP: 130/70 mm/Hg, SpO2: 96 (room air), Pulse: 85 beat/min. Biochemical parameters: CRP: 2.1 mg/dl, W: 6,000, ESR: 6 mm/h. Thorax CT was requested upon the detection of a nodular lesion in the left lower lung zone of the PA X-ray (Figure 1). An irregularly margined, 17x27 mm diameter, mass lesion was seen in the superior part of the left lower lobe of the lung, adjacent to a fissure (Figure 2). TTFNAB was performed on the mass lesion; CK7, CK20, TTF1 focally positive, Napsin-A and P63 negative adenocarcinoma was detected. In the
patient’s PET-CT, in the left lung superior lower lobe the 20.5x19.8 mm primary lesion with spiked margins and surrounded with ground glass densities had moderate metabolic activity. Mediastinal lymphadeno megaly or distant metastasis was not detected (Figure 3). Left lower lobectomy and mediastinal lymph node dissection was performed with left thoracotomy. The pathology report was tumor Napsin-A and TTF-1 negative, CDX2 positive in the majority of ell nuclei. CEA +, KI-67 positivity was in the range of 15-20%. According to immunohistochemical results, the tumor was not a ‘Primary Lung Carcinoma,’ it was metastatic. It was thought that it would be beneficial to investigate the pancreatic and the gastrointestinal system in the investigation for he primary origin. The patient underwent endoscopy and colonoscopy for primary tumor detection, but the results were non-diagnostic. Abdominal MR, MR-CP, and cholangiography were performed, but no pathology was detected. No additional pathology was detected in other systemic examinations. In the second year of follow-up, no pathology was detected in the whole-body scan. The patient, whose immunohistochemical examination excluded primary lung carcinoma and showed metastasis, the primary origin could not be detected. He was followed annually with whole-body scans.
Discussion
Immunohistochemistry is the detection of antigens in a particular tissue using marked antibodies. When tissue sections containing antigens are incubated in a solution containing marked antibodies against these antigens, the antibodies specifically bind to those antigens. Thus, the location of the antigen-antibody complexes (intracellular, extracellular, membrane) can be observed with a microscope.7 The differential diagnosis of a lung mass includes benign and malignant tumors of the lung, metastatic tumors, and inflammatory and infectious diseases.8 The incidence of metastatic lung cancer is increasing day by day. Pathologists have difficulties in distinguishing between primary and metastatic tumors. Especially in patients who come to the clinic with a solitary pulmonary nodule, it is difficult to distinguish primary lung cancer from metastatic cancer. When immunohistochemical markers are used, it is possible to estimate the primary origin of metastatic tumors.9 TTF-1 expression has been shown to be a reliable marker for the detection of lung cancer.10,11 TTF-1 has a high specificity (100%) and sensitivity (75-94%) especially in the differential diagnosis of pulmonary adenocarcinomas and extrapulmonary metastatic adenocarcinomas.12 Napsin, which is an aspartic protease and plays a role in the maturation of surfactant B7, is helpful in differential diagnosis in imprecise cases. A combination of Napsin-A and TTF-1 is useful in distinguishing primary lung adenocarcinomas.13 Stella et al. have described metastatic disease in which the primary tumor site cannot be detected despite all detailed examinations as metastatic cancers of unknown primary origin.1 In our case, diagnostic tests performed on the solitary nodule in the lung were initially evaluated as primary lung adenocarcinoma; excisional biopsy showed metastatic characteristics in the pathology results. However, despite all the detailed examinations seeking the origin, it could not be determined. In a study by Fabrizio et al., TTF-1, Napsin-A, CDX-2, SP-A, MUC5AC, and CK-5 were screened for as immunohistochemical markers in 531 patients with lung adenocarcinomas between 2003 and 2013. If the sum of the scores had a positive value, an “alveolar differentiation” was defined; if the sum of the scores was negative, a “bronchiolar differentia tion” was defined. If the sum of the scores was 0, two categories were defined: “Hallow type” if the neoplastic cells showed no markers and “mixed type” if the neoplastic cells showed both alveolar and bronchiolar markers.13 CDX-2 is a transcription factor involved in the regulation of intestinal epithelial cells and is generally positive in intestinal adenocarcinomas. However, another study by Nottegar et al. showed that CDX-2 is also prominent in intestinal type adenocarcinomas of the lung.13 In the light of these studies of primary lung cancer, our case, although metastatic adenocarcinoma was primarily considered, may also be among primary lung adenocarcinomas showing TTF-1, Napsin-A negativity, and CDX-2 positivity. However, as other immunohistochemical markers cannot be evaluated due to limitations of our clinic, a precise diagnosis could not be made.In conclusion, our case, which presented with a mass in the lung, was primarily considered as metastatic cancer, but no symptoms of the primary tumor had been detected by the end of 2 years of follow-up. The patient continues to be treated and followed with an unknown metastatic cancer protocol. However, it should be kept in mind that primary lung adenocarcinomas may rarely have immunohistochemical markers such as metastatic carcinomas in this and similar cases, and all possible immunohistochemical markers that might be useful in differential diagnosis should be studied.
Declarations
Animal and Human Rights Statement
All procedures performed in this study involving human participants were conducted in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content including study design, data collection, analysis and interpretation, writing, and final approval of the manuscript.
References
-
Stella GM, Senetta R, Cassenti A, Ronco M, Cassoni P. Cancers of unknown primary origin: current perspectives and future therapeutic strategies. J Transl Med. 2012;10:12. doi:10.1186/1479-5876-10-12
-
Pavlidis N, Pentheroudakis G. Cancer of unknown primary site. Lancet. 2012;379(9824):1428-1435. doi:10.1016/s0140-6736(11)61178-1
-
Pavlidis N, Pentheroudakis G. Cancer of unknown primary site: 20 questions to be answered. Ann Oncol. 2010;21(suppl 7):vii303-vii307. doi:10.1093/annonc/mdq278
-
Natoli C, Ramazzotti V, Nappi O, Giacomini P, Palmeri S, Salvatore M, et al. Unknown primary tumors. Biochim Biophys Acta. 2011;1816(1):13-24. doi:10.1016/j.bbcan.2011.02.002
-
Kaprealian T, Yom SS. Management of the neck and unknown primary of the head and neck. In: Hansen EK, Roach M, eds. Handbook of evidence-based radiation oncology. 2nd ed. Springer; 2010:197-200. doi:10.1007/978-0-387-92988-0_13
-
Capelozzi VL. Papel da imuno-histoquímica no diagnóstico do câncer de pulmão. J Bras Pneumol. 2009;35:375-382. doi:10.1590/s1806-37132009000400012
-
Horn L, Johnson DH. Neoplasm of the lung. In: Harrison’s principles of internal medicine. 19th ed. McGraw-Hill; 2015:506-522.
-
Bohinski RJ, Bejarano PA, Balko G, Warnick RE, Whitsett JA. Determination of lung as the primary site of cerebral metastatic adenocarcinomas using monoclonal antibody to thyroid transcription factor-1. J Neurooncol. 1998;40(3):227-231. doi:10.1023/a:1006102607697
-
Kaufmann O, Dietel M. Expression of thyroid transcription factor-1 in pulmonary and extrapulmonary small cell carcinomas and other neuroendocrine carcinomas of various primary sites. Histopathology. 2000;36(5):415-420. doi:10.1046/j.1365-2559.2000.00890.x
-
Ordóñez NG. Thyroid transcription factor-1 is a marker of lung and thyroid carcinomas. Adv Anat Pathol. 2000;7(2):123-127. doi:10.1097/00125480-200007020-00007
-
Di Loreto C, Di Lauro V, Puglisi F, Damante G, Fabbro D, Beltrami CA. Immunocytochemical expression of tissue-specific transcription factor-1 in lung carcinoma. J Clin Pathol. 1997;50(1):30-32. doi:10.1136/jcp.50.1.30
-
Travis WD, Brambilla E, Nicholson AG, Yatabe Y, Austin JHM, Beasley MB, et al. The 2015 World Health Organization classification of lung tumors: impact of genetic, clinical and radiologic advances since the 2004 classification. J Thorac Oncol. 2015;10(9):1243-1260. doi:10.1097/jto.0000000000000630
-
Nottegar A, Tabbò F, Luchini C, Brunelli M, Bria E, Veronese N, et al. Pulmonary adenocarcinoma with enteric differentiation: immunohistochemistry and molecular morphology. Appl Immunohistochem Mol Morphol. 2016.
Figures
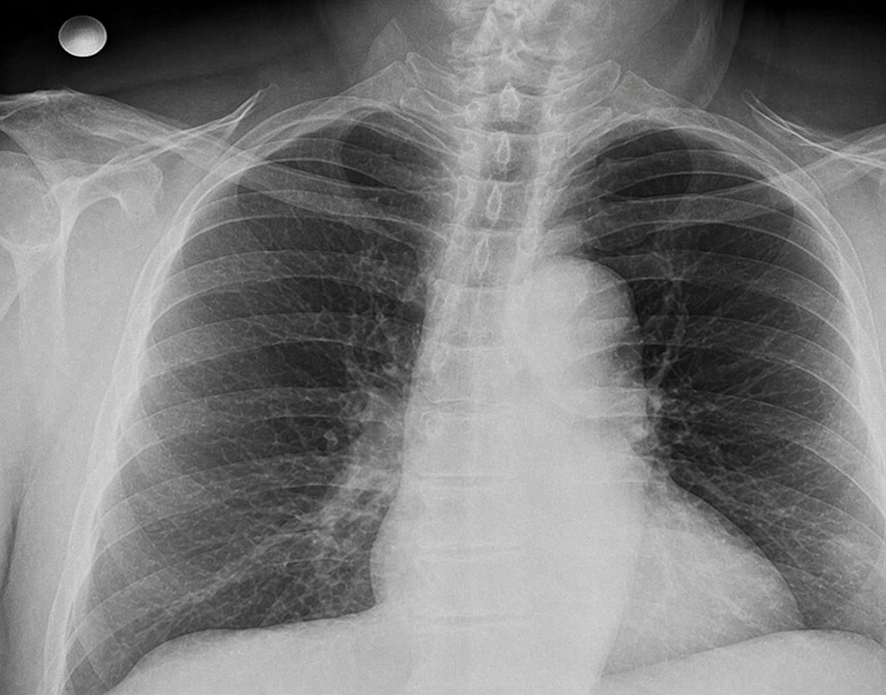
Figure 1. Postero-anterior X-ray film
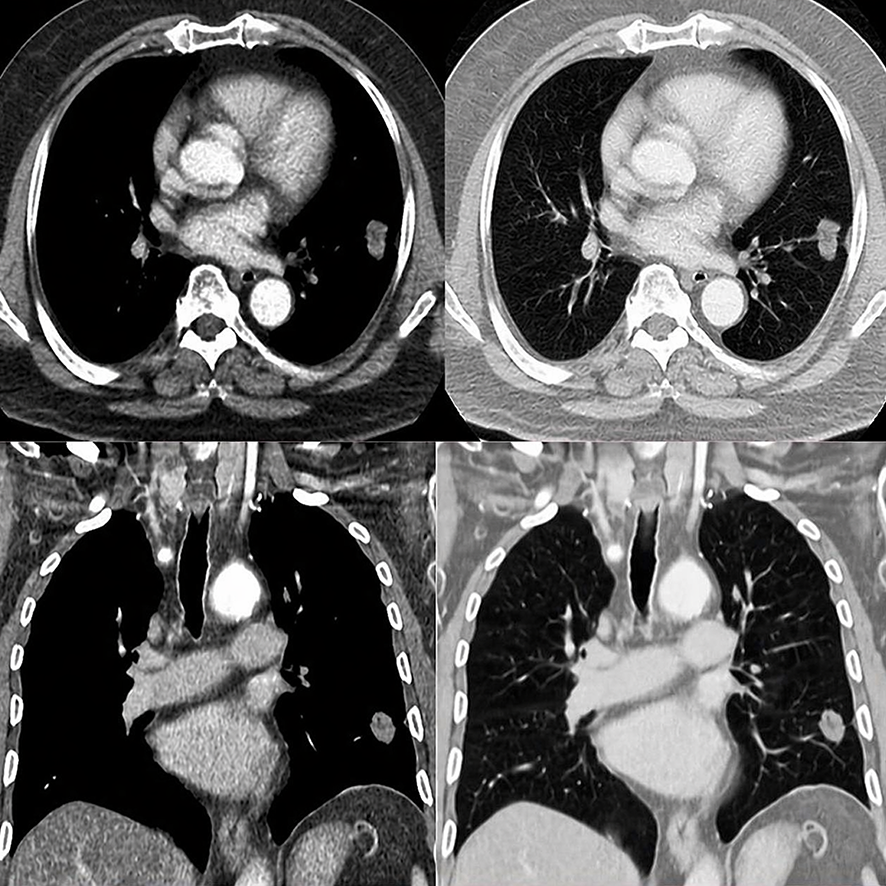
Figure 2. Thorax CT of the case

Figure 3. PET-CT sections of the case
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Kübra Aşık Cansız, Suat Konuk, Hacı Ali Kılıçgün, Çetin Boran, Tuncer Tuğ. Metastatic lung carcinoma with unknown primary site. Eu Clin Anal Med 2018;6(3): 35-38.
- Received:
- April 11, 2018
- Accepted:
- April 27, 2018
- Published Online:
- April 28, 2018
- Printed:
- September 1, 2018