Multidetector computed tomography findings of craniosynostosis
CT imaging in craniosynostosis
Authors
Abstract
AimThe aim of this study was to investigate the demographic characteristics and multidetector computed tomography (MDCT) findings of children with craniosynostosis.
MethodsWe retrospectively evaluated 30 patients admitted to our center with suspicion of craniosynostosis and who had undergone 64-slice MDCT scans.
ResultsOverall, 12 patients were diagnosed with craniosynostosis in the study. The mean age was 11.9 months (2–24 months). The synostosis sites were metopic (n=4), coronal (n=4), sagittal (n=2), bilateral lambdoid (n=1), and metopic-coronal-lambdoid-sagittal (n=1).
ConclusionRapid scanning with MDCT minimizes image degradation from patient movement, especially in children. Three-dimensional CT still has a place in the evaluation of patients with skull deformities and potential craniosynostosis.
Keywords
Introduction
Craniosynostosis, or craniostenosis, is the premature fusion of cranial sutures. It may be isolated or accompanied by craniofacial syndromes, such as Apert, Crouzon, Pfeiffer, Carpenter, and Saethre–Chotzen, and causes disfigurement of the skull. Craniosynostosis is usually classified into two categories, namely simple (one suture) and complex (two or more sutures).1 The etiology is basically divided into primary and secondary categories. In primary craniosynostosis, there is an intrinsic defect in the suture. Secondary craniosynostosis displays the premature closure of normal sutures because of another medical condition, such as deficient brain growth. Primary craniosynostosis can be idiopathic or familial.2 Secondary craniosynostosis results from a known underlying disorder (i.e., systemic and metabolic conditions such as hyperthyroidism, hypercalcemia, hypophosphatasia, vitamin D deficiency, renal osteodystrophy, Hurler’s syndrome, sickle cell disease, and thalassemia).3 Types of major suture synostoses include dolichocephaly, scaphocephaly, brachycephaly, anterior plagiocephaly, turricephaly, posterior plagiocephaly, trigonocephaly, oxycephaly, and cloverleaf deformity, also known askleeblattschädel.4 The diagnosis relies on a physical examination and radiographic studies, including plain radiography and CT.5 CT scans are particularly useful in the evaluation of calvarial deformities, intracranial abnormalities, and postoperative follow-up of calvarial deformities.4 The aim of this study was to investigate the demographic characteristics and MDCT findings of children with craniosynostosis.
Materials and Methods
The CT findings of 30 patients who were admitted to our center for suspicion of craniosynostosis were evaluated retrospectively. Twelve patients were diagnosed with craniosynostosis. Eighteen patients who had normal sutures for their age were excluded from the study. We therefore assessed 12 patients who had MDCT scans for craniosynostosis. They were admitted to our hospital with complaints of deformities of the head, swelling in the head, and growth retardation. The patients’
demographic details were recorded and included age, sex, family history, pregnancy/birth features (twin pregnancies, methods of birth, birth weight), maternal features (age, smoking, uterine malformation/fibroids, fertility treatment), paternal features (age, smoking, work), and infant sleeping position. The MDCT findings included suture synostosis (single and complex) and incidental findings (prominent extra-axial cerebrospinal fluid (CSF), ventriculomegaly, hydrocephalus, etc.) Three-dimensional (3D) CT volume rendered images of the cranial suture were generated in all cases. For the assessment, a 64-slice MDCT scanner (Toshiba Aquilon, Toshiba Medical Systems, Otawara, Japan) was used, and the CT scans involved the administration of radiation. However, at our institution, we are compliant with the ALARA (as low as reasonably achievable) concept. The imaging parameters used were 120 kV and 150 mA. The evaluations were done by two experienced radiologists.
Results
We evaluated the CT findings of 12 patients (male/female: 6/6) with craniosynostosis at our center. The mean age was 11.9 months (2–24 months). There was no family history of craniosynostosis for any of the patients. The mean maternal age was 29.5 years (22–38 years) and the mean paternal age was 37.08 years (27–68 years). The demographic characteristics of the study groups are shown in Table 1. The MDCT findings included suture synostosis and incidental findings. Ten cases were simple craniosynostosis and two cases were complex craniosynostosis. The synostosis sites were metopic (n=4), coronal (n=4), sagittal (n=2), bilateral lambdoid (n=1), and metopic-coronal-lambdoid-sagittal (n=1) (Figures 1-5) (Table 2). Incidental MDCT findings were present in six patients. The incidental findings included extra-axial CSF (n=3), septum pellucidum variants (n=3), and cerebral atrophy (n=1). In addition, fontanellar bone (wormian bone) was detected in one patient (Table 2).
Five patients had barrel stave osteotomies, which involved the expansion of the vault by creating multiple parallel osteotomies. The controls were normal.
Discussion
Craniosynostosis occurs due to a prematurely fused cranial vault and presents as a craniafacial malformation.6 The prevalence of craniosynostosis is different in several populations, such as the Caucasian, Asian, American Indian, African, and Australian populations. In the literature, most cases (72%) are sporadic. The gender distribution is similar for both genders.7 In our study, the male-to-female ratio was 1:1 and all the cases were sporadic. The time to diagnosis of craniosynostosis varies according to clinical severity. Although most of the cases are diagnosed in the first few months, some mild cases are not diagnosed in the early period of life.8 This was mirrored in our study where the mean age was 11.9 months.
According to the literature, the potential risk factors include white maternal race, advanced maternal age, male infant sex,9 maternal smoking,10 maternal residence at high altitude,11 use of nitrosatable drugs (e.g., nitrofurantoin, chlordiazepoxide,chlorpheniramine),12 paternal occupation (e.g., agriculture and forestry careers, mechanics, repairmen),13 fertility treatments, complications during pregnancy, duration of gestation, and birth weight.14,15 In our study, all the mothers were of the white race and there was only one elderly parent. In one case, both the father and the mother smoked, while in another case, only the mother smoked. Only four patients were born vaginally. There were no twin pregnancies. All the patients had normal birth weights. None of the patients had a constant sleeping position that could cause craniosynostosis. The fathers’ occupations comprised mostly workers although one father was retired, another was a driver, and a third was a carpenter.
Plain radiography is the first step in the evaluation of suspected craniosynostosis, and sutures can be identified more accurately on a CT scan.6 In particular, the diagnosis of craniosynostosis includes CT scan with 3D surface-rendered reconstructions.6 Moreover, rapid scanning with 64-slice MDCT minimizes image degradation due to patient movement; in selected cases however, patients may have to be sedated. Planar bone algorithm images in the axial, sagittal, and coronal planes facilitate problem solving if the presence of suture fusion is unclear from the 3D images.4 In our study, 3D 64-slice MDCT volume rendered images of the cranial suture was performed in all cases. The MDCT findings included suture synostosis and incidental findings.In the literature, craniosynostosis sutures can be both isolated and multiple. The frequencies of the most common isolated suture types are sagittal suture (56%), coronal suture (25%), metopic suture (4%), and lambdoid suture (2%). The frequency of multiple sutures is 13%.16,17,18 In our study, the synostosis sites comprised metopic and coronal sutures (33%), sagittal sutures (16%), bilateral lambdoid sutures (8%), and metopic-coronal-lambdoid-sagittal sutures (8%). Incidental findings were present in 50% of the patients. Septum pellucidum variants were present in three cases, and three cases of prominence of the subarachnoid space and one case of cerebral atrophy were identified. The determination of this issue is important as it can affect surgery. It is possible that the presence of benign extra-axial CSF in patients undergoing cranial remodeling for craniosynostosis may predispose them to an increased risk of subdural bleeding.19,20 Incidental CT findings should therefore be stated in the report.
Conservative management is the mainstay for secondary craniosynostosis. Surgical treatment is typical for primary craniosynostosis where there is an obvious restriction of brain growth and raised intracranial pressure. Surgery is advised as soon as the infant is able to tolerate it, usually between the ages of 3 and 9 months, because the calvarial bones are malleable and heal effectively.1,4 In our study, five patients had surgery where barrel stave osteotomy was the selected method. There were some limitations to our study. First, our study was retrospective. Second, the study power was reduced because the number of patients was inadequate. Finally, magnetic resonance imaging (MRI) is an excellent tool to evaluate brain incidental anomalies such as ventricular dilatation, hypoplastic corpus callosum, and hypoplastic cerebellar vermis.
In conclusion, this report reviewed the criteria and methods used for the early diagnosis of craniosynostosis. In patients with potential risk factors, CT should be conducted. Rapid scanning with 64-slice MDCT minimizes image degradation from patient movement, especially in children. However, 3D CT still has a place in the evaluation of skull deformities and potential craniosynostosis, and the planning of surgical reconstruction.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments.
Informed Consent
Informed consent was obtained from all participants.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the scientific content of the article, including the study design, data collection, analysis and interpretation, manuscript preparation, and approval of the final version of the manuscript.
References
-
Ocal E, Sun PP, Persing JA. Craniosynostosis. In: Albright AL, Pollack IF, Adelson PD, eds. Principles and practice of pediatric neurosurgery. Thieme Medical; 2007:265-285.
-
Kimonis V, Gold JA, Hoffman TL, Panchal J, Boyadjiev SA. Genetics of craniosynostosis. Semin Pediatr Neurol. 2007;14(3):150-161. doi:10.1016/j.spen.2007.08.008
-
Cohen MM Jr. Sutural pathology. In: Cohen MM Jr, MacLean RE, eds. Craniosynostosis: diagnosis, evaluation and management. Oxford University Press; 2000:158-171.
-
Khanna PC, Thapa MM, Iyer RS, Prasad SS. Pictorial essay: the many faces of craniosynostosis. Indian J Radiol Imaging. 2011;21(1):49-56. doi:10.4103/0971-3026.76055
-
Hoffman WY, McCarthy JG, Cutting CB, Zide BM. Computerized tomographic analysis of orbital hypertelorism repair: spatial relationship of the globe and the bony orbit. Ann Plast Surg. 1990;25(2):124-131. doi:10.1097/00000637-199008000-00009
-
Aviv R, Rodger E, Hall C. Craniosynostosis. Clin Radiol. 2002;57(2):93-102. doi:10.1053/crad.2001.0836
-
Lajeunie E, Catala M, Renier D. Craniosynostosis: from a clinical description to an understanding of bone formation of the skull. Childs Nerv Syst. 1999;15(11-12):676-680. doi:10.1007/s003810050457
-
Kabbani H, Raghuveer TS. Craniosynostosis. Am Fam Physician. 2004;69(12):2863-2870.
-
Alderman BW, Lammer EJ, Joshua SC, Cordero JF, Ouimette DR, Wilson MJ, et al. An epidemiologic study of craniosynostosis: risk indicators for the occurrence of craniosynostosis in Colorado. Am J Epidemiol. 1988;128(2):431-438. doi:10.1093/oxfordjournals.aje.a114983
-
Kallen K. Maternal smoking and craniosynostosis. Teratology. 1999;60(3):146-150. doi:10.1002/(sici)1096-9926(199909)60:33.3.co;2-v
-
Alderman BW, Zamudio S, Baron AE, Joshua SC, Fernbach SK, Greene C, et al. Increased risk of craniosynostosis with higher antenatal maternal altitude. Int J Epidemiol. 1995;24(2):420-426. doi:10.1093/ije/24.2.420
-
Gardner JS, Guyard-Boileau B, Alderman BW, Fernbach SK, Greene C, Mangione EJ. Maternal exposure to prescription and non-prescription pharmaceuticals or drugs of abuse and risk of craniosynostosis. Int J Epidemiol. 1998;27(1):64-67. doi:10.1093/ije/27.1.64
-
Bradley CM, Alderman BW, Williams MA, Checkoway H, Fernbach SK, Greene C, et al. Parental occupations as risk factors for craniosynostosis in offspring. Epidemiology. 1995;6(3):306-310. doi:10.1097/00001648-199505000-00020
-
Panchal J, Uttchin V. Management of craniosynostosis. Plast Reconstr Surg. 2003;111(6):2032-2048. doi:10.1097/01.prs.0000056839.94034.47
-
Argenta LC, David LR, Wilson JA, Bell WO. An increase in infant cranial deformity with supine sleeping position. J Craniofac Surg. 1996;7(1):5-11. doi:10.1097/00001665-199601000-00005
-
Vannier MW, Hildebolt CF, Marsh JL, Pilgram TK, McAlister WH, Shackelford GD, et al. Craniosynostosis: diagnostic value of three-dimensional CT reconstruction. Radiology. 1989;173(3):669-673. doi:10.1148/radiology.173.3.2813770
-
Fearon JA, McLaughlin EB, Kolar JC. Sagittal craniosynostosis: surgical outcomes and long-term growth. Plast Reconstr Surg. 2006;117(2):532-541. doi:10.1097/01.prs.0000200774.31311.09
-
Marsh JL, Vannier MW. Comprehensive care for craniofacial deformities. Mosby; 1985.
-
Amodio J, Spektor V, Pramanik B, Rivera R, Pinkney L, Fefferman N. Spontaneous development of bilateral subdural hematomas in an infant with benign infantile hydrocephalus: color Doppler assessment of vessels traversing extra-axial spaces. Pediatr Radiol. 2005;35(11):1113-1117. doi:10.1007/s00247-005-1503-x
-
Swift D, McBride L. Chronic subdural hematoma in children. Neurosurg Clin N Am. 2000;11(3):439-446. doi:10.1016/s1042-3680(18)30106-2
Figures

Figure 1. Trigonocephaly, 1a. Diagram of metopic suture synostosis in the characteristic trigone-shaped skull, 1b. Axial CT scan image shows trigonocephaly, 1c–f. Superior, anterior, lateral, and anterosuperior 3D MDCT volume rendered images show trigonocephaly secondary to premature fusion of the metopic suture.
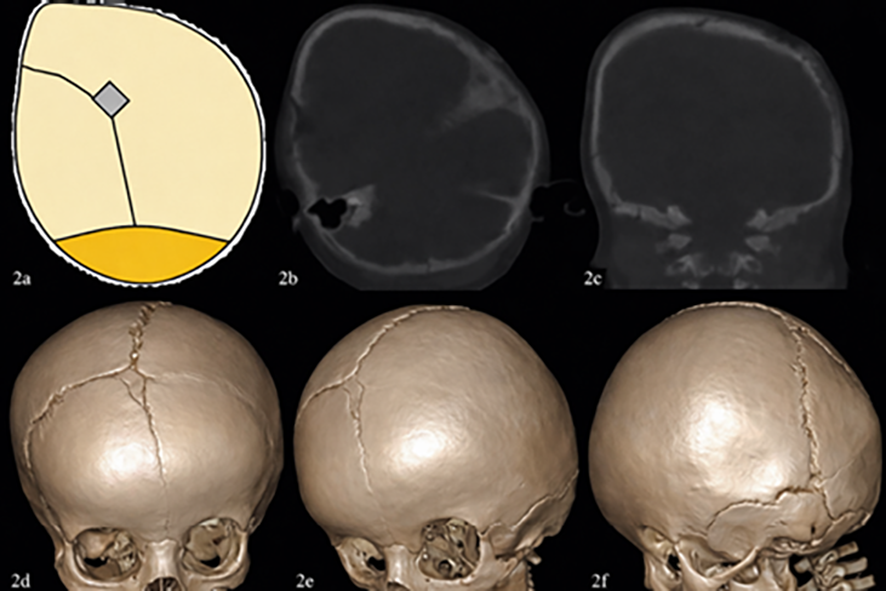
Figure 2. Anterior plagiocephaly, 2a. Diagram of unilateral left coronal suture synostosis, 2b c. Axial and coronal CT scan images show anterior plagiochephaly secondary to premature fusion of the unilateral left coronal suture synostosis, 2d–f. Anterior, left anteriolateral oblique, and lateral 3D MDCT volume rendered images show anterior plagiochephaly.
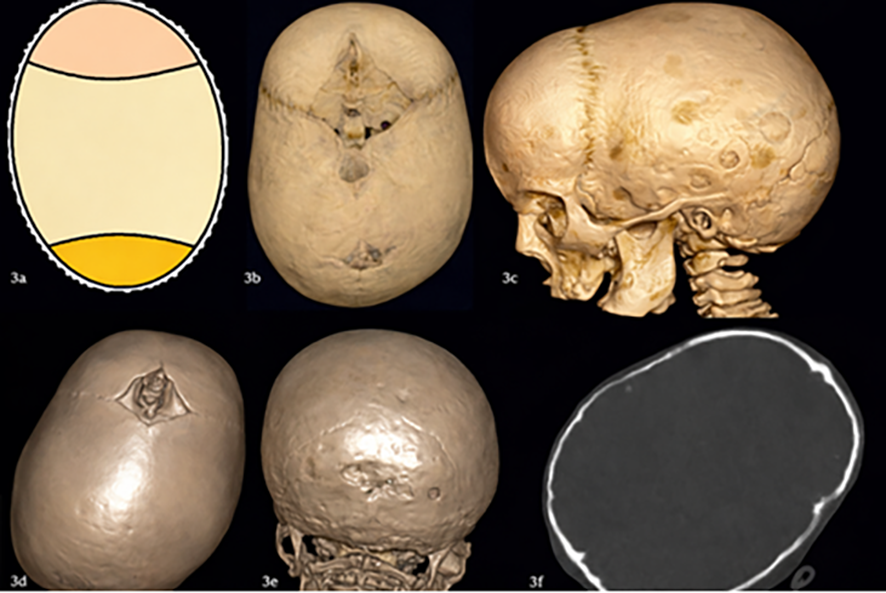
Figure 3. Scaphocephaly, 3a. Diagram of sagittal suture synostosis, 3b–e. Superior, lateral, superior, and posterior 3D MDCT volume rendered images show scaphocephaly secondary to premature fusion of the sagittal suture, 3f. Axial CT scan image shows scaphocephaly.
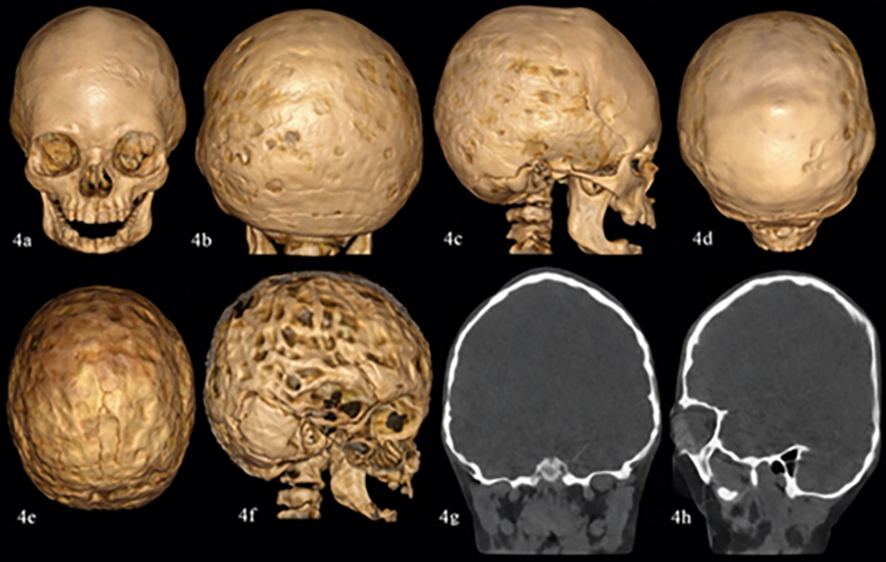
Figure 4. Turricephaly, 4a–d. Anterior, posterior, lateral, and superior 3D MDCT volume rendered images, 4e–f. Endocranial 3D MDCT volume rendered images show turricephaly secondary to bilateral lambdoid sutures synostosis and scalloping on the inner tabula of the skull secondary to increased intracranial pressure, 4g–h. Coronal and sagittal CT scan images show turricephaly and scalloping on the inner tabula of the skull secondary to increased intracranial pressure.
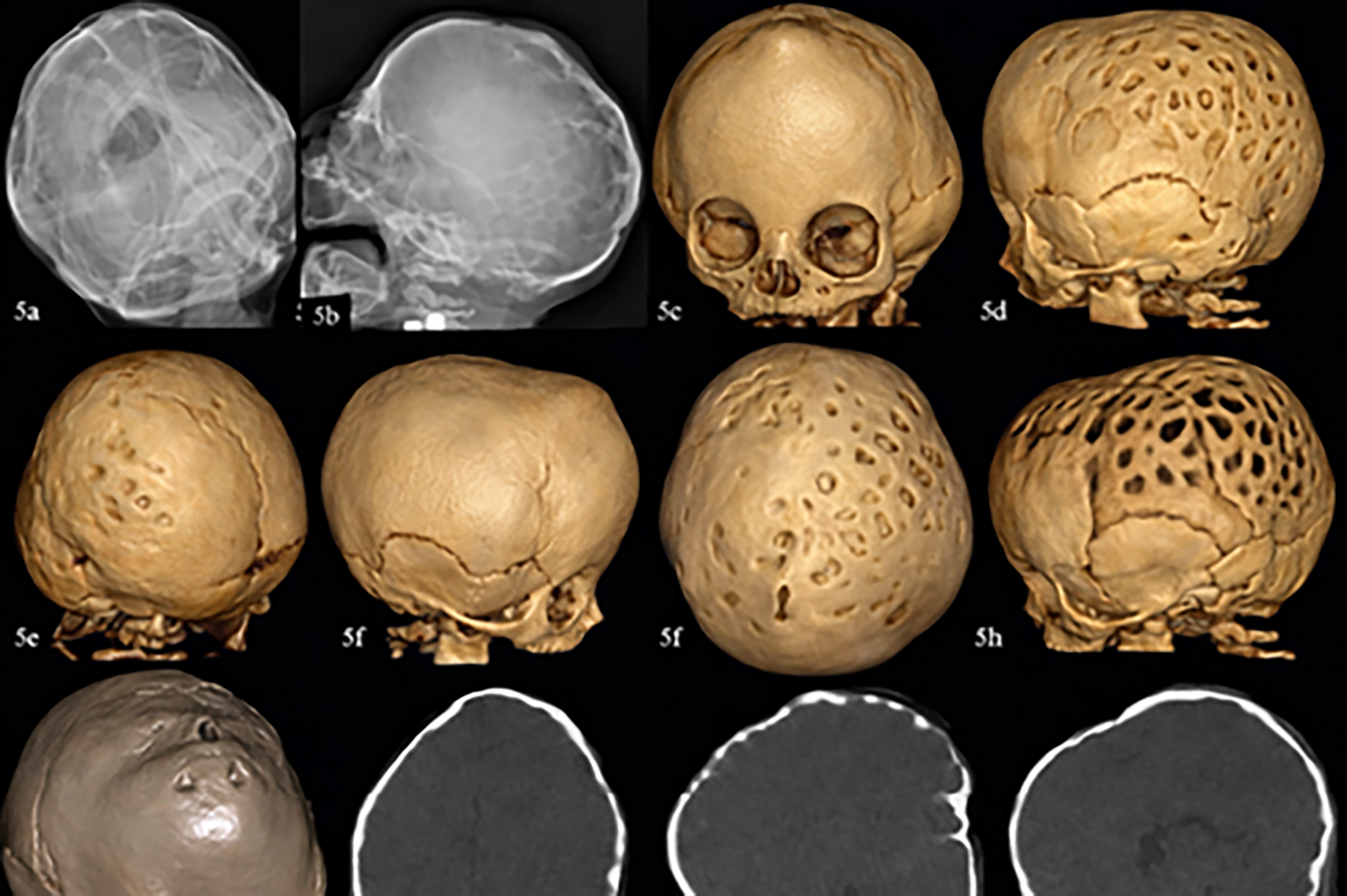
Figure 5. Trigonocephaly and cloverleaf deformity , 5a–b. Anterior-posterior and lateral plan radiographs show cloverleaf deformity secondary metopic, coronal, sagittal, and partial right lambdoid sutures synostosis and scalloping on the inner tabula of the skull secondary to increased intracranial pressure, 5c–i. Anterior, right lateral, posterior, left lateral, superior, and endocranial 3D MDCT volume rendered images, 5j–l. Axial, para-sagittal, and mid-sagittal CT scan images show trigonocephaly secondary metopic sutures synostosis and scalloping on the inner tabula of the skull secondary to increased intracranial pressure.
Tables
Table 1. The demographic characteristics of the study groups

B; Boy, G; Girl, M; Maternal, P; Paternal, C/S;Caesarean Section, N; Normal
Table 2. The MDCT findings of children with craniosynostosis
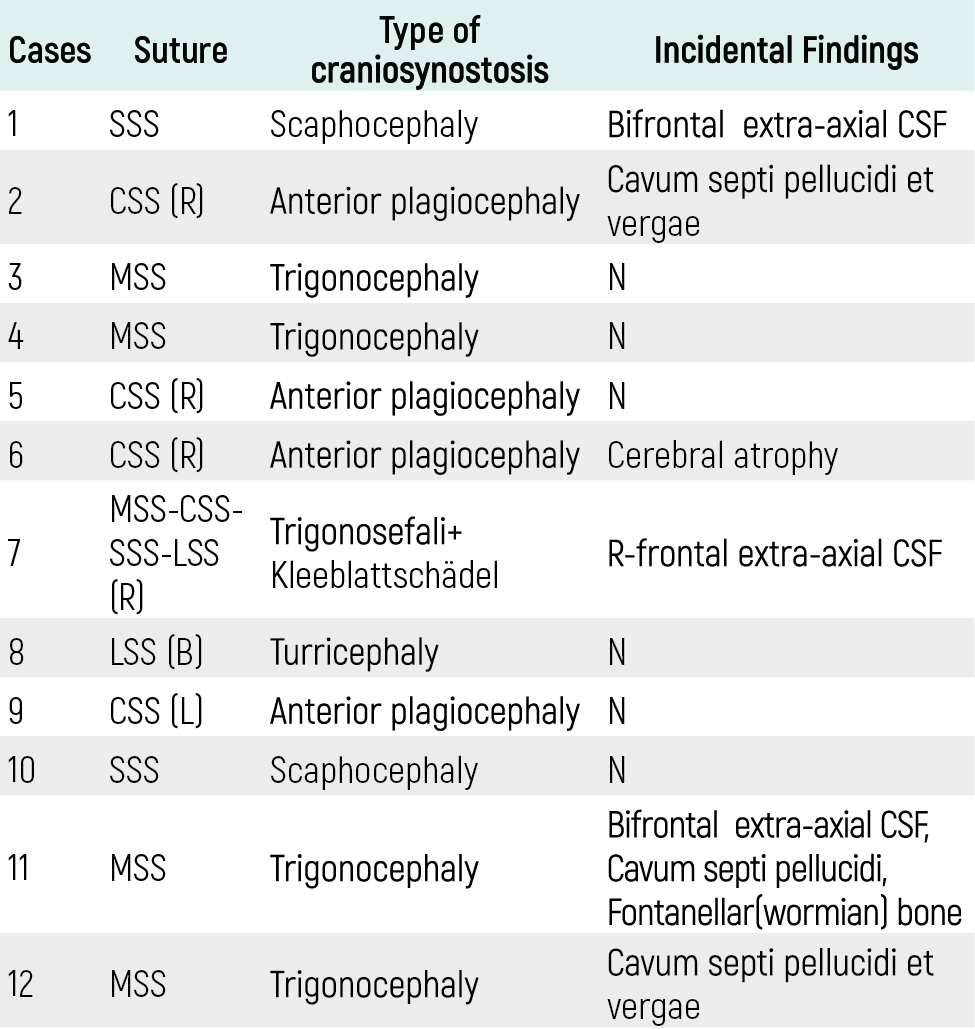
MSS; metopik suture synostosis, CSS; coronal suture synostosis, LSS; lamdoid suture synostosis, SSS; sagital suture synostosis, R; right, L; left, B; bilateral.CSF; Cerebrospinal Fluid.
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Nesrin Atcı, Hanifi Bayaroğulları, Pınar Döner, Alperen Kayalı, Gülen Burakgazi, Fatma Öztürk, Sinem Karazincir. Multidetector computed tomography findings of craniosynostosis. Eu Clin Anal Med 2016;4(1):5-8. doi:10.4328/ECAM.71
- Received:
- November 24, 2015
- Accepted:
- November 14, 2015
- Published Online:
- January 1, 2016
- Printed:
- January 1, 2016