Epstein barr virus induced thrombosis: A Case Report
Epstein barr virus
Authors
Abstract
IntroductionEpstein Barr virus (EBV), which may develop at any age, is a common infection of childhood and young adulthood. EBV is transmitted by oropharyngeal secretions, close contact, blood, and by contaminated articles. Clinically, it is characterized by fever, sore throat, fatigue, and generalized lymphadenopathy. EBV-associated thrombosis has rarely been reported, mostly in immunocompromised patients.Case PresentationIn this paper, we report on a 46-year old male admitted with fatigue, lack of appetite, and abdominal pain. In our case, chronic active EBV-triggered superior mesentericvein thrombosiswas detected; factor V leiden mutationwas found. The patient was operated on for mesenteric ischemia. Recurrent acute kidney injury (AKI) developed due to short bowel syndrome. ConclusionAKI was treated with fluid and electrolyte replacement. In this article, we present an immunocompetent patient with superior mesentericvein thrombosis and hereditary thrombophilia.
Keywords
Introduction
Studies indicate that approximately 90% of adults worldwide are infected with EBV or herpes virus type 4.1 In immunocompetent children, acute infection is usually asymptomatic; it presents as an infectious mononucleosis (IM) in 30-50% of the immunocompetent adolescents and adults.2,3 In immunocompressed patients, EBV is associated with various lymphoproliferative and neoplastic (burkitt lymphoma and nasopharyngeal carcinoma) disorders. Primary infection occurs mainly during adolescence and causes IM in 35% to 50% of the cases. Typically, IM leads to the characteristic triad of fever, pharyngitis, and lymphadenopathy and can be accompanied by splenomegaly. IM may also cause severe acute complications such as hematologic and neurologic complications, upper airway obstruction, myocarditis, splenic rupture, mucosal oedema, and can also lead to an increased bleeding tendency.4
Viral infections are associated with coagulation disorders. Viral infections can affect the coagulation cascade, primary hemostasis, coagulation, and fibrinolysis. As a result, thrombosis and disseminated intravascular coagulation and hemorrhage may occur. The association between venous thromboembolism and EBV has rarely been described. The mechanisms by which EBV infection might promote thrombosis are not fully understood. Possible mechanisms include transient elevation of anti-phospholipid antibodies and EBV-induced oxidative endothelial cell injury.5,6
Case Presentation
A 46-year old male patient complained of fatigue and loss of appetite for a one-month duration and of abdominal pain for the previous week. His history revealed that he had bilateral lower extremity thrombosis 15 years previously and cerebrovascular disease 10 years previously. At the time of admission, the general condition of the patient was moderate and he was not on any medicine. His physical examination revealed a blood pressure of 130/75mmHg, body temperature of 38,9°C, pulse of 98/min, and abdominal tenderness and rebound. His laboratory findings were as follows: glucose: 158mg (100-106), blood serumurea nitrogen (BUN): 15,8 mg/dl (6-20), serum creatinine (CRE): 1,0 mg/dl, (07-1,2), alanine aminotransferase (ALT): 24 IU/L (0-41), aspartate aminotransferase (AST): 22 IU/L (0-40), lactate dehydrogenase (LDH): 278 IU/L (135-225), gamma-glutamyl transferase (GGT): 160IU/L (0-50),
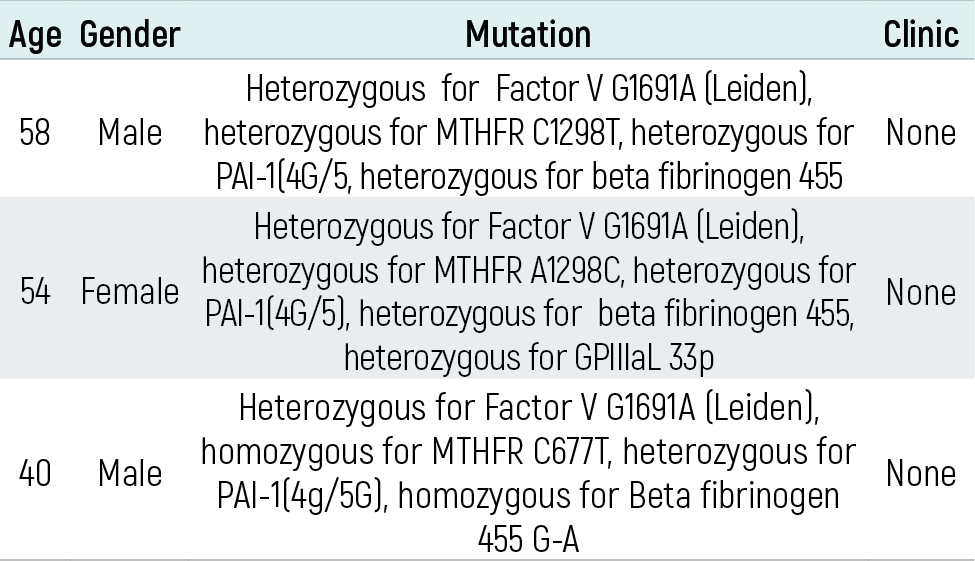
serum sodium: 141 mEq/L (136-145), potassium: 4,4 mEq/L (3,5-5,5), total protein: 6,4 gr/dl(6,4-8,3), serum albumin: 3,8 gr/dl (3,5-5,2), leucocyte count: 15000 mm3/L (4000-10000), hemoglobin (Hb): 14 gr/dl (13-16), hematocrit (Htc): 43%, platelet count (Plt): 138000/mm³ (150000-450000), C-reactive protein (CRP): 129 mg/L (0-8), sedimentation: 30 mm/hr, prothrombin time: 20 (10,7-13), international normalized ratio (INR): 1,7 (0,8-1,2), partial thromboplastin time: 85 (22-36), and procalcitonine: 0,15 (<0.1microgram/L). Because of increased abdominal pain in his follow-up examination andhaving both defence and rebound in physical examination, the patient underwent abdominal tomography which revealed increased spleen size, patchy hypodense areas (long axis of the largest one 7 cm), and free fluid in the perisplenic and perihepatic areas (ischemia). The superior mesenteric vein was totally occlusive to the level of celiac truncus. Intestinal walls at the lower quadrant of the abdomen were dilated up to 4,5cm. There were multiple lymph nodes (largest having a diameter of 2cm) in the paraaortic and paracaval regions and in the mesenteric region. There was fluid between the intestinal walls at the lower quadrant of the abdomen. The portal vein was not clear at the liver hilus, which was compatible with cavernous transformation. Thrombosis was observed in the lumen at the renal vein level of the inferior vena cava. Lower extremity Doppler revealed thrombosis allowing minimal flow at the right femoral and popliteal veins. In the middle and distal parts of the left femoral vein, an echogenic thrombus resistant to compression and preventing blood flow from peripheral veins was observed. The lung ventilation perfusion scintigraphy showed moderate risk for pulmonary embolism. The patient was operated on for mesenteric embolism. The whole small intestine wall was necrotized starting 70 cm from the treits up to 20 cm to the ileocecal valve. The necrotized section was resected and the patient underwent an ileostomy. The results of the biopsy revealed hemorrhag ic necrosis and reactive lymphadenopathy. Peripheral smear showed normochromic normocytes, 68% polymorphonuclear, 38% lymphocyte and atypical lymphocyte, 4% monocyte, and sufficient thrombocytes. Protein C, protein S, antithrombin III and anti-cardiolipines were within the normal range.The patient tested heterozygous for factor V G1691A (leiden), homozygous for MTHFR C677T, heterozygous for PAI-1(4g/5G), homozygous for fibrinogen 455 G-A, and heterozygous for GPIIIaL33P mutations. Factors VII and VIII were within the normal range. In terms of paroxysmal nocturnal hemoglobinuria, the flair test was normal. Enoxaparin sodium 6000 anti-Xa/0,6 ml (2x1 dose) was initiated. Then, enoxaparin sodium was ceased and coumadin 5 mg was started (international normalized ratio was kept between 3,0-3,5). The patient applied to the emergency service with nausea and vomiting one week after hospital discharge. Upon examination, he was diagnosed with AKIwith uremic symptoms and laboratory findings. The laboratory findings of the patient are given in Table 1. Serological examinations showed that ANA,anti-Ds DNA, p-ANCA, c-ANCA, anti-GBM antibodies were negative, complements were within the normal range, and viral markers positive EBV VCA IgM, positive EBV VCA IgG and positive EBV EBNA IgG and other viral markers were negative. This was interpreted as a late primary infection or reactivation in terms of EBV. Complete urinalysis was normal. The amount of proteinuria in 24-hr urine was 640 mg/day. The patient had watery output from his ileostomy 10-15 times a day (nearly 3500 cc/day). Recurrent AKI developed due to short bowel syndrome.The follow-up examination revealed development of recurrent AKI (a total of 4 times). The patient underwent haemodialysis upon uremic symptoms in his first AKI. Fluid electrolyte replacement was performed. After two months, his follow-up examination revealed that EBV VCA IgM was negative. After two months, the amount of proteinuria in 24-hr urine was 120 mg/day. AKI did not reoccur after closing his ileostomy after 3 months. Cardiovascular panel thrombotictests were carried out in 3 siblings of the patent. The results are given Table 2.
Discussion
Clinical outbreak of thromboembolism may differ among individuals carrying a prothrombotic genetic risk profile within their families. Moreover, thrombus formation is affected by environmental factors beyond the genetic ones. As our case had positive EBV VCA IgM positive, EBV VCA IgG positive and EBV EBNA IgG positive tests, we estimated that he had a reactivation. EBV infection can contribute to the occurrence of venous thrombosis in immunocompetent patients. We believe that the mutations as a result of chronic and active EBV reactivations could cause thrombosis by triggering a thrombosis cascade. Although 3 siblings of the patient had mutation, none had thrombosis. Moreover, our case had deep vein thrombosis 20 years previously and he was not receiving thromboembolism prophylaxis. In the literature, it is emphasised that there is an association between viral infections and thrombosis. Hepatitis viruses may increase thrombosis risk by several mechanisms. Acute viral hepatitis can induce inflammatory changes in surrounding tissues, in particular the endothelium of the portal vein system, leading to activation of the coagulation system by inflammation and increasing the risk of portal vein thrombosis. Also, anti-phospholipid antibodies may have a role in thrombosis pathogenesis.7 Cytomegalovirus-associated thrombosis has been extensively reported in the medical literature. Genetic predisposing factors for thrombosis in patients with CMV-associated thrombosis, such as factor V leiden mutation, were also previously reported.8 The most accepted theory indicates that acute CMV infection is associated with a transient appearance of anti-phospholipid antibodies.9 However, in some other reported cases, no hemostatic abnormalities could be found. A few cases have been reported related to EBV. Predisposing risk factors for thrombosis have sometimes been found in the reported cases such asprotein C deficiency, hereditary thrombophilia, and transient elevation of anti-phospholipid antibodies.6,10,11,12 Occasionally, EBV is associated with renal involvement. Patients may present with haematuria and/or proteinuria. Renal complications include acute kidney failure, tubulointerstitial nephritis, glomerulonephritis, haemolytic uremic syndrome, and nephrotic syndrome .13,14 Although renal involvement in EBV infection occurs most frequently in the form of tubulointerstitial nephritis, sometimes mesangial proliferation or focal tubular necrosis are also observed. 640 mg/day proteinuria was detected in our case and no biopsy was performed. In his follow-up, we found that proteinuria disappeared after EBV IgM became negative. In our case, recurrent AKI developed due to short bowel syndrome associated with the bowel resection performed for mesenteric ischemia. The patient had watery output from his ileostomy 10-15 times a day (nearly 3500 cc). In short bowel syndrome, abnormal fluid and electrolyte absorption may develop depending on the location and amount of resection. Insufficient fluid absorption causes dehydration, which leads to AKI. Sufficient oral or intravenous hydration helps serum creatinine levels return to normal limits. EBV infection may contribute to the thrombosis occurrence of mesenteric veins, portal veins, and lower extremity veins in immunocompetent patients. In patients presenting with thrombosis, clinical and laboratory evaluations should be made, and treatment should be arranged in accordance with the obtained results, or morbidity and mortality will increase. Recurrent AKI may develop due to short bowel syndrome associated with the bowel resection performed for mesenteric ischemia. A close follow-up and fluid and electrolyte replacements would prevent end-stage renal failure in these patients.As a result, we wish to raise awareness of EBV infection as a precipitating factor of venous thromboembolism among patients with hereditary thrombophilias.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. No animal or human studies were carried out by the authors for this article.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
None of the authors received any type of financial support that could be considered potential conflict of interest regarding the manuscript or its submission.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content including study design, data collection, analysis and interpretation, writing, some of the main line, or all of the preparation and scientific review of the contents and approval of the final version of the article.
References
-
Rickinson AB, Kieff E. Epstein-Barr virus. In: Knipe DM, Howley PM, Griffin DE, Martin MA, Lamb RA, eds. Fields’ virology. 4th ed. Lippincott Williams & Wilkins; 2001:2575-2627.
-
Lennette ET. Epstein-Barr virus (EBV). In: Lennette EH, Lennette DA, Lennette ET, eds. Diagnostic procedures for viral, rickettsial, and chlamydial infections. American Public Health Association; 1995:299-312.
-
Steven NM. Infectious mononucleosis. EBV Rep. 1996;3:91-95.
-
Luzuriaga K, Sullivan JL. Infectious mononucleosis. N Engl J Med. 2010;362:1993-2000. doi:10.1056/nejmcp1001116
-
Dalpke AH, Thomssen R, Ritter K. Oxidative injury to endothelial cells due to Epstein-Barr virus–induced autoantibodies against manganese superoxide dismutase. J Med Virol. 2003;71:408-416. doi:10.1002/jmv.10501
-
Yamazaki M, Asakura H, Kawamura Y, Ohka T, Endo M, Matsuda T. Transient lupus anticoagulant induced by Epstein-Barr virus infection. Blood Coagul Fibrinolysis. 1991;2:771-774. doi:10.1097/00001721-199112000-00012
-
Zignego AL, Ferri C, Pileri SA, Caini P, Bianchi FB; Italian Association for the Study of the Liver Commission on Extrahepatic Manifestations of HCV Infection. Extrahepatic manifestations of hepatitis C virus infection: a general overview and guidelines for a clinical approach. Dig Liver Dis. 2007;39:2-17. doi:10.1016/j.dld.2006.06.008
-
Abgueguen P, Delbos V, Chennebault JM, Payan C, Pichard E. Vascular thrombosis and acute CMV infection in immunocompetent patients: report of 2 cases and literature review. Clin Infect Dis. 2003;36:134-138. doi:10.1086/374664
-
Gharavi AE, Pierangeli SS, Espinola RG, Liu X, Colden-Stanfield M, Harris EN. Antiphospholipid antibodies induced in mice by immunization with a cytomegalovirus-derived peptide cause thrombosis and activation of endothelial cells in vivo. Arthritis Rheum. 2002;46:545-552. doi:10.1002/art.10130
-
Husein B, Iqbal J. Epstein-Barr virus and cerebral vein thrombosis. Infect Dis Clin Pract. 2012;20:95-96. doi:10.1097/ipc.0b013e318234c350
-
Knees U, Macdonald E, Stiegler H, Ohly A, Pontz BF. Pelvic vein thrombosis in protein C deficiency after infectious mononucleosis. Monatsschr Kinderheilkd. 1993;141(12):928-931.
-
Mashav N, Saar N, Chundadze T, Steinvil A, Justo D. Epstein-Barr virus–associated venous thromboembolism: a case report and review of the literature. Thromb Res. 2008;122(4):570-571. doi:10.1016/j.thromres.2008.03.005
-
Kano K, Yamada Y, Sato Y, Arisaka O, Ono Y, Ueda Y. Glomerulonephritis in a patient with chronic active Epstein-Barr virus infection. Pediatr Nephrol. 2005;20:89-92. doi:10.1007/s00467-004-1645-3
-
Joh K, Kanetsuna Y, Ishikawa Y, Aizawa S, Imadachi A, Tatsusawa O, Ohishi T. Epstein-Barr virus genome-positive tubulointerstitial nephritis associated with immune complex–mediated glomerulonephritis in chronic active Epstein-Barr virus infection. Virchows Arch. 1998;432:567-573. doi:10.1007/s004280050207
Tables
Table 1. Laboratory Finding of Patient
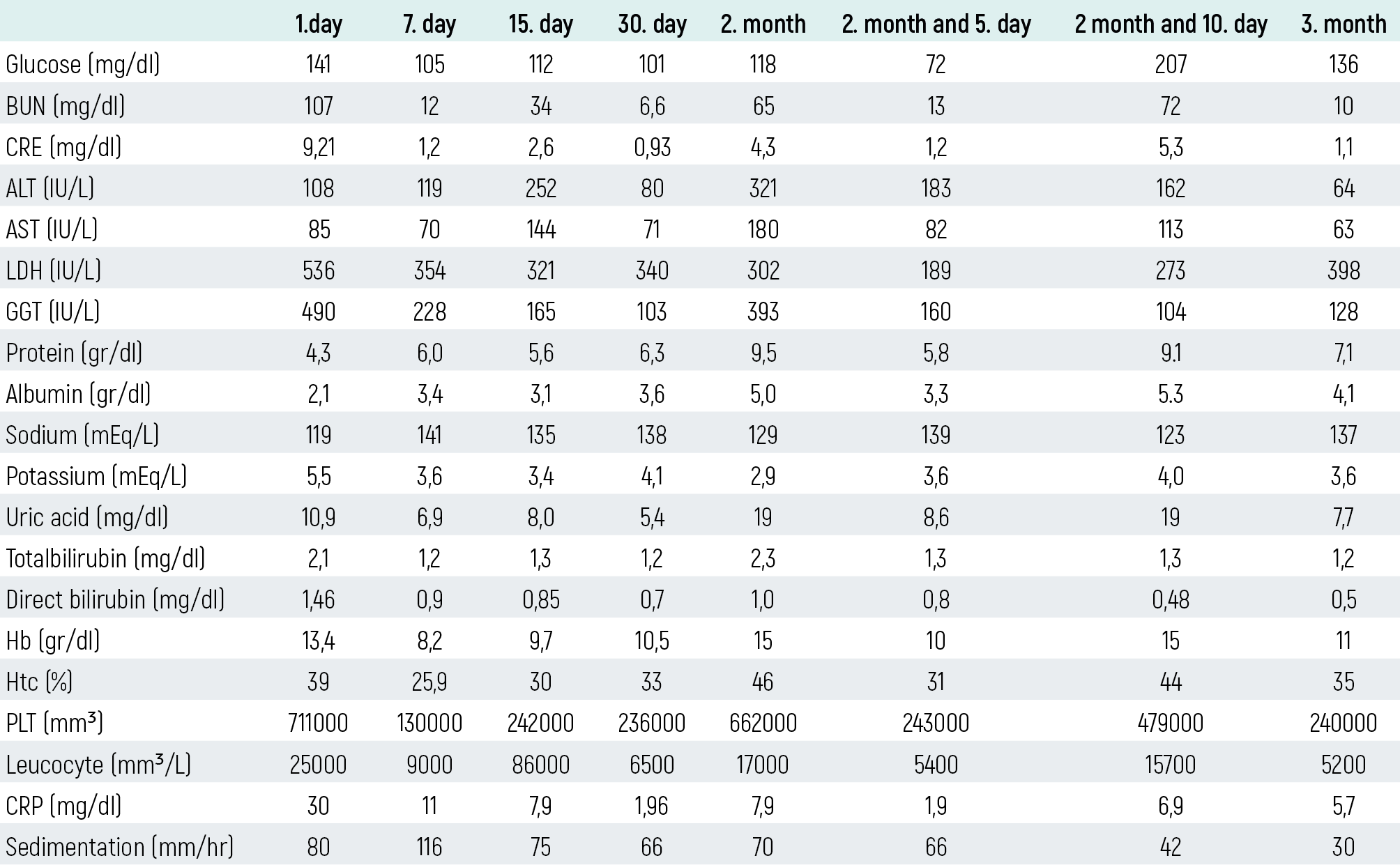
Table 2. Cardiovascular panel of the siblings
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Can Hüzmeli, Ferhan Candan, Demet Alaygut, Sinan Soylu, Mansur Kayataş. Epstein Barr Virus Induced Thrombosis. Eu Clin Anal Med 2016;4(2): 58-61.
- Received:
- February 7, 2016
- Accepted:
- February 16, 2016
- Published Online:
- May 1, 2016
- Printed:
- May 1, 2016