A study of distal sensory nerves in patients with newly diagnosed asymptomatic type 2 DM
A study of diabetic polyneuropathy
Authors
Abstract
AimThis study aimed to determine the importance of Medial Plantar (MP), Dorsal Sural (DS) and Medial Dorsal Cutaneous (MDC) sensory nerve conduction studies in addition to the other routine electrophysiological studies performed in newly diagnosed Type II Diabetes Mellitus (DM) for diagnosing diabetic polyneuropathy (PNP) at an early stage.
MethodsThis study included a total of 35 patients aged less than 60 years with newly diagnosed,untreated Type II Diabetes, and 30 healthy volunteers who applied to the Outpatient Clinic of Internal Medicine and Endocrinology at Şanlıurfa Training and Research Hospital and Harran University Faculty of Medicine Research and Application Hospital between April 2014 and August 2014.
ResultsOur study enrolled a total of 35 Type II Diabetes patients (20 females, 15 males) with a mean age of 47.22±8.15 years, and 30 healthy controls (17 females and 13 males) with a mean age of 49.30±6.56 years. The two groups did not significantly differ with respect to age and sex (p>0.05). MP, MDC, and DS sensory nerve conduction studies, performed additionally to the standard PNP protocol, revealed that the amplitudes and conduction velocities of each of the three nerves were significantly lower than those of the control group (p<0.01).
ConclusionIt is possible to diagnose diabetic PNP at an early, asymptomatic stage by studying sensory nerves conduction properties of MP, MDC, and DS in addition to the standard electrophysiological PNP protocol. Detection of PNP by these methods at an early stage may help taking measures to prevent progression intosymptomatic PNP.
Keywords
Introduction
Signs and symptoms related to peripheral nervous system with no other apparent cause in a diabetic patient are collectively referred to as diabetic neuropathy. Diabetic neuropathy can cause a wide spectrum of abnormalities ranging from autonomic and cardiovascular abnormalities to diabetic foot ulcers. The most common type of diabetic polyneuropathy (PNP) is the distal symmetric PNP and the associated neuropathic pain.1 It is well known that long-standing hyperglycemia causes neuropathy in diabetic patients. Neuropathy may also become manifest in the early stage of the glucose regulation disorder.2 The neuropathy prevalence has been reported 10% in newly diagnosed Type II Diabetes patients, stressing the importance of early diagnosis of that disorder.3 The present study aimed to determine the importance of Medial Plantar (MP), Dorsal Sural (DS) and Medial Dorsal Cutaneous (MDC) sensory nerve conduction studies (NCS) in addition to the other routine electrophysiological studies in newly diagnosed Type II Diabetes Mellitus (DM) for diagnosing diabetic PNP at an early stage.
Materials and Methods
This study enrolled 35 patients under the age of 60 years with newly diagnosed, untreated Type II diabetes, and 30 healthy volunteers who were admitted to the outpatient clinics of Internal Medicine and Endocrinology at Şanlıurfa Training and Research Hospital and Harran University Faculty of Medicine Research and Application Hospital between April 2014 and August 2014.
Patients with lumbar radiculopathy, mononeuropathy, and plexopathy diagnosed by neurological examination and electrophysiological studies were excluded from the study protocol. In addition, patients with renal failure, any other disease likely to cause peripheral neuropathy, drug use associated with peripheral neuropathy, or exposure to toxic substances were also excluded.
This study was conducted in accordance with the Declaration of Helsinki, and all subjects provided informed consent prior to participation. The study was approved (Approval No: 74059997.050.01.04/64) by the local ethics committee of Harran University.
All patients and control subjects underwent MP, DS, and MDC sensory nerve conduction studies (NCS) in the ENMG laboratory, in addition to the routine PNP study protocol, which included motor NCS of bilateral posterior tibial, peroneal, median, and ulnar nerves, as well as sensory NCS of bilateral sural, median, and ulnar nerves.
The electrophysiological studies were performed using the Nihon Kohden EMG-EP V-08 device. Skin temperature was maintained between 31–33 °C. Conduction studies were carried out using Ag/AgCl disk surface electrodes.
Subjects then underwent conventional sensory and motor nerve conduction studies of the lower and upper extremities. In the nerve conduction study, motor latency was measured from the onset of the negative deflection, and motor amplitude was measured between the peaks of the negative and positive deflections.
Motor nerve examinations were performed with a filter frequency of 10 Hz–5 kHz, a sweep speed of 5 ms/div, a stimulus duration of 0.2 ms, and a stimulus frequency of 1/sec. The corresponding settings for sensory nerve examination were 20 Hz–2 kHz, 1 ms/div, 0.2 ms, and 1/sec, respectively.
Sensory Nerve Conduction Studiesa) Both MP nerves were stimulated using a felt electrode in the direction of the recording electrode at a point distal to it, at the medial part of the sole between the metatarsal bones (Figure 1). Orthodromic recordings were obtained from the medial malleolus over the flexor retinaculum. The nerve conduction velocity, distal latency, and amplitude were measured.
b) Both MDC nerves were stimulated using a felt electrode in the direction of the recording electrode at a point distal to it, at the medial part of the dorsum of the foot between the first and second metatarsal bones (Figure 2). Orthodromic recordings were obtained over the medial one-third of the line connecting the medial and lateral malleoli. Additionally, the distal latency and sensory action potential of this nerve were measured.also measured.
c) The DS nerve was stimulated using a felt electrode to study the former’s sensory conduction and the antidromic recordings were made from the surface electrodes placed at the distal part of the fifth metatarsal bone on the dorsum of foot (Figure 3).
Statistical AnalysisThe statistical analyses of the study data were performed with SPSS (Statistical Package for Social Sciences) Windows 11.5 software package. A P value less than 0.05 was considered statistically significant. Descriptive statistics (mean, standard deviation), Mann Whitney U test, and Independent samples T-test was used for evaluation of the study data.
Results
Our study included a total of 35 patients with Type II diabetes (20 females, 15 males) with a mean age of 47.22±8.15 years and 30 healthy controls (17 females, 13 males) with a mean age of 49.30±6.56 years. The two groups did not differ significantly in terms of age and sex (p>0.05).
The routine study protocol, including motor nerve conduction studies (NCS) of the bilateral posterior tibial, peroneal, median, and ulnar nerves, as well as sensory NCS of the bilateral sural, median, and ulnar nerves, were within normal limits and similar in both groups (p>0.05). MP, DS, and MDC nerve action potentials were obtained in all subjects. The results of the DS, MP, and MDC sensory NCS were compared between the patient and control groups. In the control group, the mean amplitudes were 6.61 µV for the DS nerve, 8.23 µV for the MP nerve, and 3.92 µV for the MDC nerve. In the diabetic group, the mean amplitudes were 3.96 µV for the DS nerve, 3.95 µV for the MP nerve, and 2.41 µV for the MDC nerve. The diabetic group showed a significant decrease in the amplitudes of all three nerves compared to the control group (p<0.001) (Table 1).
The control group had a mean nerve conduction velocity (NCV) of 50.81 m/s for the DS nerve, 55.64 m/s for the MP nerve, and 43.92 m/s for the MDC nerve. The diabetic patient group had a mean NCV of 41.48 m/s for the DS nerve, 44.08 m/s for the MP nerve, and 39.56 m/s for the MDC nerve. The diabetic patients showed significant slowing in all three nerves compared to the control group (p<0.001).
Discussion
The signs of diabetic neuropathy may not be evident on routine electrophysiological studies performed early in the course of the disorder, and electrophysiological diagnosis becomes difficult in patients who are either asymptomatic or newly and slightly symptomatin.4
PNP has been reported to have a prevalence of 7% in the first year after the diagnosis of DM and 50% in a 25-year follow-up. Adding EMG and other ancillary tests to clinical evaluation results in a prevalence exceeding 60%; the rate even reaches 90% when subclinical cases are also considered.5
Our study demonstrated impaired DS, MDC, and MP nerve studies despite normal routine electrophysiological studies in newly diagnosed Type II DM. This finding aligns with the understanding that DS, MDC, and MP nerves are the most distal sensory nerves and confirms previous studies suggesting that early pathological events are more evident in the distal part of sensory fibers.6,7 Hence, detecting subclinical PNP in DM at an early stage is possible via conduction studies on the most distal nerves.
Although there are many electrophysiological studies in the literature examining diabetic neuropathy, studies investigating DS nerve conduction are limited. DS nerve conduction studies were first defined in 1974 by Burke et al., who reported that DS nerve values are highly variable.8
Our study revealed a mean MP nerve conduction velocity (NCV) of 50.81±3.12 m/s with a lower limit of 44 m/s. Of the 35 patients with diabetes, 14 patients had an MP NCV less than 44 m/s. Our results demonstrated that 40% of the diabetes group could be neurophysiologically diagnosed with PNP despite normal conventional nerve conduction studies.
Leventoğlu et al. also found a significantly slower DS nerve conduction velocity in early-stage Type II diabetes patients with neuropathic complaints consistent with PNP compared to normal values in routine electrophysiological studies and the control group.9 Similarly, we observed slowing in DS NCV even though our patients were neurologically asymptomatic. This suggests that approximately 40% of patients with newly diagnosed Type II DM who have no neuropathic complaints may already have electrophysiological abnormalities.
Killian and Foreman (2001) studied bilateral sural and DS nerve conduction antidromically in 70 patients with PNP of non-diabetic origin (alcoholic, autoimmune, arteritis, or drug-induced) who had sensory symptoms and one or more clinical signs, and in 38 controls. They found that sural sensory action potentials could not be detected or were reduced in 77% of patients, while 23% had normal sural sensory action potentials. Bilateral dorsal sural amplitudes were not detectable in 97% of the 70 patients. They demonstrated that DS nerve may be affected before pathology emerges in the sural nerve.10
Kökoğlu et al. detected a slowing in DS NCV in the patient group compared to the control group in early-stage diabetic neuropathy.11 Uluç et al. found significantly lower amplitudes and conduction velocities of DS and MP sensory nerve responses in patients with diabetic sensory neuropathy and normal routine electrophysiological studies.12 Our results were in agreement with these findings, although our patients had no symptoms suggestive of sensory neuropathy.
Our study revealed a mean MP NCV of 55.64±4.09 m/s with a lower limit of 44 m/s. Of the 35 patients with diabetes, 14 had an MP NCV less than 44 m/s. Thus, 40% of the diabetes group could be neurophysiologically diagnosed with PNP despite normal conventional nerve conduction studies.
In our study, the control group had a mean MDC NCV of 43.92±1.49 m/s with a lower limit of 40 m/s. Of the 35 patients with diabetes, 14 patients had a DS NCV less than 40 m/s. Thus, 40% of the diabetes group could be neurophysiologically diagnosed with PNP despite normal conventional nerve conduction studies.
In another study, Altun et al. compared DS and MDC nerve conduction in patients diagnosed with diabetic PNP and reported that DS nerve conduction was more sensitive.13
We neurophysiologically detected asymptomatic PNP in diabetic patients by studying nerve conduction properties of the three most distally located nerves (MP, DS, MDC) in addition to classical nerve conduction studies in patients with newly diagnosed diabetes and no neurological symptoms. While the results of classical nerve conduction studies were normal in early-stage diabetes, the earliest signs of polyneuropathy were observed as slowing of sensory conduction velocities and slight reduction in amplitudes of sensory action potentials in the MP, MDC, and DS nerves.
Among these three nerve conductions, MP and DS sensory nerve conduction velocities were significantly lower than those of MDC. Furthermore, the measurement of MDC nerve conduction is technically more demanding, and its conduction may not be detected physiologically even in normal individuals at advanced age, suggesting that MP and DS nerve conductions are more sensitive and reliable. However, we were able to obtain MP, DS, and MDC nerve conduction responses in both the..control group and the diabetic patients, which emphasizes the importance of these nerves in diagnosing early-stage PNP.
In conclusion, it may be possible to detect pathology neurophysiologically in asymptomatic diabetic PNP at an early stage by studying MP and DS sensory nerve conduction properties in addition to the nerve conduction parameters included in a standard PNP protocol at the ENMG laboratory. Detecting PNP during the asymptomatic period using these methods may help implement measures to prevent progression into symptomatic PNP.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments.
Informed Consent
Informed consent was obtained from all participants.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the scientific content of the article, including the study design, data collection, analysis and interpretation, manuscript preparation, and approval of the final version of the manuscript.
References
-
Tan E. Nöropatik ağrı. 2nd ed. Pfizer; 2009:119.
-
Diabetes Control and Complications Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993;329:977-986. doi:10.1056/nejm199309303291401
-
Bennett GJ. Neuropathic pain. In: Melzack R, Wall PD, eds. Textbook of pain. 3rd ed. Churchill Livingstone; 1994:201-224.
-
Pastore C, Izura V, Geijo-Barrientos E, Dominguez JR. A comparison of electrophysiological tests for the early diagnosis of diabetic neuropathy. Muscle Nerve. 1999;22:1667-1673. doi:10.1002/(sici)1097-4598(199912)22:123.0.co;2-w
-
Ertekin C. Diyabetik nöropatiler. In: Santral ve periferik EMG anatomi-fizyoloji-klinik. 2006:211-228.
-
Vinik A, Mehrabyan A. Diabetic neuropathies. Med Clin North Am. 2004;88:947-999. doi:10.1016/j.mcna.2004.04.009
-
Zochodne DW. Diabetes mellitus and the peripheral nervous system: manifestations and mechanisms. Muscle Nerve. 2007;36:144-166. doi:10.1002/mus.20785
-
Burke D, Skuse NF, Lethlean AK. Sensory conduction of the sural nerve in polyneuropathy. J Neurol Neurosurg Psychiatry. 1974;37:647-652. doi:10.1136/jnnp.37.6.647
-
Leventoğlu A, Oğuz AK, Ünaldı MZ. Erken dönem tip II diabetes mellituslu hastalarda fasial ve dorsal sural sinir iletim çalışmalarının klinik değeri. J Neurol Sci (Turk). 2009;26(1):1-7.
-
Killian JM, Foreman PJ. Clinical utility of dorsal sural nerve conduction studies. Muscle Nerve. 2001;24:817-820. doi:10.1002/mus.1074
-
Kökoğlu F, Leventoğlu A, Erdemoğlu AK. Dorsal sural nerve conduction study in early diabetic polyneuropathy patients and relationship of adiponectin and high sensitive C-reactive protein levels. J Neurol Sci (Turk). 2009;26(4):404-415.
-
Uluc K, Isak B, Borucu D, et al. Medial plantar and dorsal sural nerve conduction studies increase the sensitivity in the detection of neuropathy in diabetic patients. Clin Neurophysiol. 2008;119:880-885. doi:10.1016/j.clinph.2008.01.001
-
Altun Y, Demirkol A, Tumay Y, Ekmekci K, Unsal I, et al. The medial plantar and medial peroneal cutaneous nerve conduction studies for diabetic polyneuropathy. Neurol Sci. 2011;32(5):849-854. doi:10.1007/s10072-011-0669-2
Figures
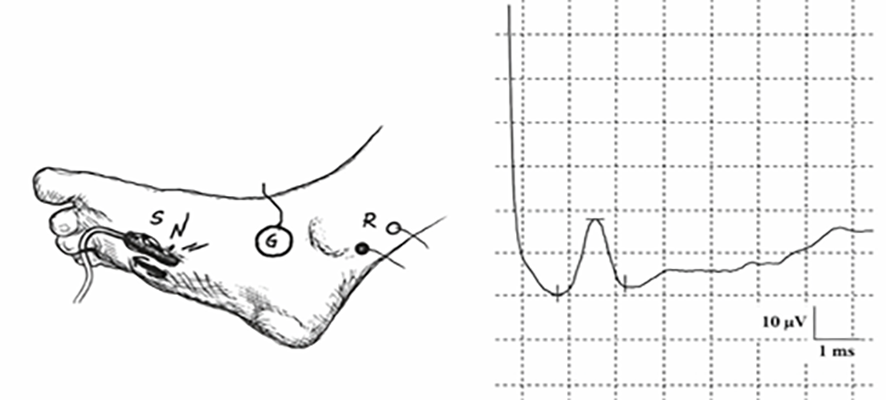
Figure 1. Medial plantar nerve conduction technique and a medial plantar nerve SNAP recording from a control subject (S, stimulating electrode; R, recording electrode; G, ground electrode)

Figure 2. Medial dorsal cutaneous nerve conduction technique and a medial dorsal cutaneous nerve SNAP recording from a control subject (S, stimulating electrode; R, recording electrode; G, ground electrode)
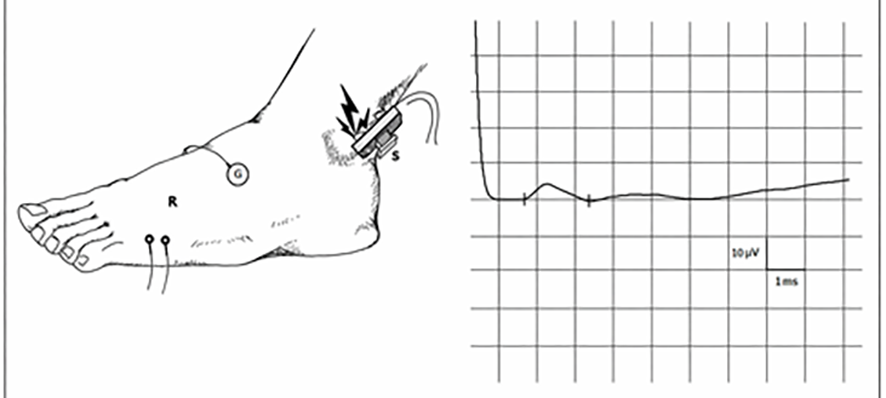
Figure 3. Dorsal sural nerve conduction technique and a dorsal sural nerve SNAP recording from a control subject (S, stimulating electrode; R, recording electrode; G, ground electrode)
Tables
Table 1. Comparison of nerve conduction data belonging to patient and control groups
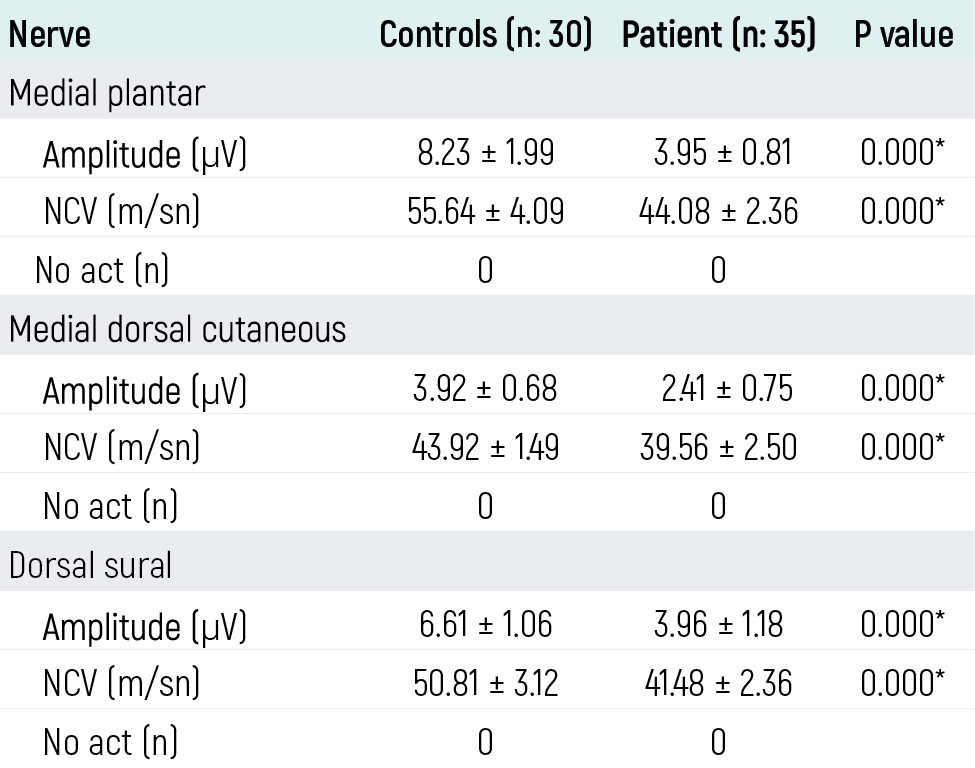
NCV nerve conduction velocity. * p<0.001(Mann Whitney U)
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Halil Ay, Yılmaz İnanç, Suna Sarıkaya Ay, Yaşar Altun, Bahar Pehlivan, Yusuf İnanç. A study of distal sensory nerves in patients with newly diagnosed asymptomatic type 2 DM. Eu Clin Anal Med 2016;4(2):32-34. doi:10.4328/ECAM.86
- Received:
- April 13, 2016
- Accepted:
- April 18, 2016
- Published Online:
- May 1, 2016
- Printed:
- May 1, 2016