Relationship between mean platelet volume and syncope
Syncope and MPV
Authors
Abstract
AimSyncope accounts for 1–2% of emergency department admissions and 6% of hospitalizations. Despite comprehensive evaluation, the etiology remains unclear in approximately 40% of cases. In this study, we aimed to investigate the relationship between mean platelet volume (MPV) and the diagnosis of syncope in order to improve future clinical approaches.
MethodsThis retrospective study was conducted using data collected between October 1, 2011 and June 30, 2012. A total of 591 patients with syncope and 523 trauma patients as the control group were included. Demographic and clinical data of the syncope and control groups were compared. A p-value of <0.05 was considered statistically significant.
ResultsWhen the syncope and control groups were compared, mean platelet volume values were found to be significantly higher in the syncope group (p<0.05). Platelet count and hematocrit values did not differ significantly between the two groups (p>0.05).
ConclusionMPV may serve as a useful parameter in the diagnosis of syncope.
Keywords
Introduction
Syncope is defined as a transient loss of consciousness (TLOC) with rapid onset, short duration, and complete recovery. It results from transient global cerebral hypoperfusion, leading to a brief impairment of the reticular activating system located in the brainstem.1,2 Syncope affects approximately 3% of men and 3–5% of women during their lifetime, although some studies suggest that the incidence may be as high as 6% in the elderly population.1
Previous studies have shown that up to one quarter of the population may experience a syncopal episode at some point in their lives.3,4 Syncope accounts for 1–2% of all emergency department admissions and approximately 6% of hospitalizations.3,4 It has a wide range of etiological causes. A subgroup analysis of the Framingham Study, which included 7,814 patients with syncope, reported that 21% had vasovagal syncope, 10% cardiac syncope, 9% orthostatic syncope, and 37% had syncope of unknown origin.5
Cardiac syncope is relatively less common but is of particular importance in emergency settings due to its association with increased morbidity and mortality, especially in relation to sudden cardiac death.6,7,8,9 Because of its potential severity, patients suspected of having cardiac syncope often undergo extensive diagnostic testing in emergency departments. However, Ciftci et al. reported that only 40–50% of patients presenting with syncope receive a definitive diagnosis.10 Other studies have similarly indicated that despite comprehensive evaluations, the cause remains unidentified in approximately 40% of cases.10,11,12 Additionally, limitations in emergency department resources contribute to 50–60% of cases remaining undiagnosed.13,14
Mean platelet volume (MPV) is a parameter routinely measured in a complete blood count but is often overlooked in clinical practice.15 It has been shown to correlate significantly with platelet function15 and has been associated with various conditions such as diabetes mellitus (DM), myocardial infarction (MI), smoking, cerebrovascular accidents (CVA), and renal artery stenosis.16,17
In this study, we aimed to evaluate the role of MPV in the diagnosis of syncope.
Materials and Methods
This retrospective study was conducted at Ankara Numune Training and Research Hospital after obtaining approval from the local ethics committee. A total of 591 patients who presented to the emergency department with syncope between October 1, 2011 and June 30, 2012 were included. Additionally, 523 patients who presented to the emergency department due to trauma during the same period were enrolled as the control group.
Study data were obtained from the hospital automation system. Patients with epilepsy; metabolic disorders such as hypoglycemia, hypoxia, or hypocapnia due to hyperventilation; intoxication; vertebrobasilar transient ischemic attack; cataplexy; drop attacks; falls; psychogenic pseudosyncope; and carotid-origin transient ischemic attack were excluded from the study.
Statistical analysis was performed using SPSS (Statistical Package for Social Sciences) version 13.0 for Windows. Descriptive statistics, including mean ± standard deviation, were calculated for clinical findings at admission and MPV values. Data were also expressed as median and interquartile range where appropriate. The normality of data distribution was assessed using the Kolmogorov-Smirnov test. Intergroup comparisons were performed using the Mann-Whitney U test and the Kruskal-Wallis test. Results were evaluated within a 95% confidence interval, and a p-value of <0.05 was considered statistically significant.
Results
This study included 591 patients with syncope (Group 1) and 523 control subjects (Group 2). The mean age was 48.1±20.6 years in Group 1 and 47.8±20.3 years in Group 2, with no significant difference between the groups (p>0.05). The syncope group consisted of 287 (48.6%) males and 304 (51.4%) females, while the control group included 197 (37.7%) males and 326 (62.3%) females. There was no statistically significant difference between the groups in terms of gender distribution (p>0.05).
Among patients presenting with syncope, 243 (41.1%) had reflex syncope, 66 (11.2%) had orthostatic syncope, 48 (8.1%) had cardiac syncope, 34 (5.8%) had neurological syncope, and 18 (3%) had syncope due to internal diseases. The etiology could not be determined in 182 patients (30.8%).
The relationship between patient age and clinical outcome is shown in Table 1. Syncope was more frequent in individuals under 40 years of age, whereas the rate of hospital admission increased significantly with advancing age. Considering that hospitalized patients generally have more severe clinical conditions, these findings suggest a correlation between increasing age and disease severity. Accordingly, a significant relationship was found between age and hospital admission rate among patients with syncope (p<0.05).
Of the patients presenting with syncope, 543 (91.9%) were discharged after evaluation in the emergency department, 44 (7.5%) were hospitalized, 3 (0.5%) were referred to another institution, and 1 (0.2%) died.
A total of 236 patients (60.1%) underwent computed brain tomography. Of these, 211 (35.7%) had normal findings. Abnormal findings included ischemia in 15 patients (2.5%), parenchymal hematoma in 1 (0.2%), aneurysm in 1 (0.2%), contusion in 1 (0.2%), mass in 1 (0.2%), and subarachnoid hemorrhage in 6 (1%).
Troponin levels were measured in 292 patients (49.4%) who were suspected of having cardiac syncope, and elevated troponin levels were found in 10 patients (1.7%).
The median hematocrit level was 40.4 in Group 1 and 40.2 in Group 2 (p>0.05). The median platelet count was 228,000/μL in Group 1 and 233,000/μL in Group 2 (p>0.05). The median mean platelet volume (MPV) was 9.7 fL in Group 1 and 9.1 fL in Group 2, showing a statistically significant difference (p<0.05) (Table 2).
The relationship between syncope etiology and MPV is presented in Table 3. No statistically significant difference was found between different syncope types in terms of MPV values (p>0.05).
Discussion
It is known that a quarter of the world population experience at least one syncope attack during their lifetime.1. Syncope constitutes 1-2% of all emergency department admissions and 6% of all hospitalizations.1 Baron-Esquivias et al. and Guldner et al. reported that women constituted %51.6 and 50.4% of the study populations, respectively.18,19 The gender distribution of our subjects was in accordance with the literature.
Previous studies have shown that syncope may be encountered in any age group and mortality and morbidity rates progressively increase with increasing age.9,17,18,19,20,21,22,23 The mean age of our study population was 48.1±20.6 years. These results are in agreement with the literature.
In accordance with the literature, our study showed that the most common syncope type was vasovagal syncope while the least common type was syncope owing to internal diseases.3,5,19,24,25. Slight differences between our results and others’ results may be due to the differences between the developmental level of the study centers and to the inter-societal differences.
Baron-Esquivias et al.18 reported that 25% of the subjects presenting with syncope were admitted to various clinics. Ayrik et al. reported that 23.2% of the subjects were hospitalized and 0.64% of them died.26 Our study resulted in a similar literature.
The reason of studying Hct level in our study was to investigate whether there was a difference between syncope cases due to bleeding into third space and the control group. Fouad-Tarazı et al.27 reported a mean Hct level of 39%. The Hct level found in our study (40.4) was in accordance with the levels reported in the literature; our results also suggested that Hct level had no significant role in determining syncope etiology. However, the patients admitted to internal diseases ward, as compared to other patients, had a significantly lower Hct level. This may be due to hemorrhages, mainly the gastrointestinal ones, that were managed by the department of internal disease.
There are no studies yet that specifically sought for a possible relationship between MPV and syncope although there exist some studies exploring MPV in some etiological factors of syncope. Some studies have reported that MPV increased in coronary artery disease, atherosclerosis, DM, neurological events, and gestational hypertension.28,29,30,31 MPV has been reported to be significantly increased in coronary artery disease, especially in acute coronary syndromes.32 MPV is even considered an independent risk factor for MI in persons with known coronary artery disease.33 In stable angina pectoris thrombocyte count remain unchanged but MPV is increased. In unstable angina pectoris, on the other hand, thrombocyte count is decreased but MPV is increased. It has been demonstrated that there was a correlation between MPV level and angiographic restenosis.34 Özdemir et al.35 reported a significantly elevated MPV in anterior MI. It is possible that acute coronary syndromes present with syncope as a result of impaired cardiac perfusion that leads to reduced cardiac output. Syncope may thus be associated with increased MPV level.35 Kodiatte et al.36 and Turgut et al.37, among others38,39, reported that MPV levels increased in DM. Diabetes-induced neuropathy may cause syncope through secondary autonomic impairment. In addition, syncope may ensue in patients with DM as a result of direct changes in peripheral resistance due to impaired vessel structure, and coronary artery disease. Therefore, MPV may be increased in syncope. It has been shown that smoker elderly had elevated MPV.39
Smoking may trigger syncope via cough or GIS stimulation that stimulate vasovagal reflexes. Thus, smoking may be associated with syncope and thus MPV may be increased. Short-term exercise may transiently increase thrombocyte count although MPV remains stable. In prolonged exercise, on the other hand, MPV is decreased.24 It is well known that exercise can give rise to syncope. Syncope during exertion suggest a cardiac origin while post-exercise syncope is suggestive of reflex (situational) syncope. As a result, syncope may be associated with elevated MPV.
Despite a lack of similar studies in the literature, it is well possible that platelets may increase their size to boost their function. Nevertheless, thrombocyte count may remain normal because there may be no new platelets in the peripheral circulation or there may be no sufficient time for new platelet formation. In our study MPV was increased in patients experiencing a syncopal episode. A search of the literature revealed no previous study exploring the relationship between syncope etiology and MPV. Our study found no difference between the various syncope types with regard to MPV. It is evident that brain hypoperfusion is the ultimate endpoint irrespective of the etiology of syncope. It may be speculated that syncope etiology may thus be irrelevant when it comes to MPV elevation.
Conclusion
Syncope is the common endpoint of many different pathologic conditions. Hence, it should be managed in a multidisciplinary manner. MPV should also be evaluated during syncope workup.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments.
Informed Consent
Informed consent was obtained from all participants.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the scientific content of the article, including the study design, data collection, analysis and interpretation, manuscript preparation, and approval of the final version of the manuscript.
References
-
Moya A, Sutton R, et al. Guidelines for the diagnosis and management of syncope (version 2009). Eur Heart J. 2009;30(21):2631-2671. doi:10.1093/eurheartj/ehp298
-
Ünver K, Ünver E, Çakır P. Syncope in childhood: analysis of 121 cases. J Clin Anal Med. 2013.
-
Blanc JJ, L’Her C, Touiza A, et al. Prospective evaluation and outcome of patients admitted for syncope over a 1 year period. Eur Heart J. 2002;23(10):815-820. doi:10.1053/euhj.2001.2975
-
Quinn JV, Stiell IG, McDermott DA, et al. Derivation of the San Francisco syncope rule to predict patients with short-term serious outcomes. Ann Emerg Med. 2004;43(2):224-232. doi:10.1016/s0196-0644(03)00823-0
-
Soteriades ES, Evans JC, Larson MG, et al. Incidence and prognosis of syncope. N Engl J Med. 2002;347(12):878-885. doi:10.1056/nejmoa012407
-
Zhang Q, Du J, Wang C, et al. The diagnostic protocol in children and adolescents with syncope: a multicentre prospective study. Acta Paediatr. 2009;98(5):379-384. doi:10.1111/j.1651-2227.2008.01195.x
-
Colman N, Nahn K, Ganzeboom KS, et al. Epidemiology of reflex syncope. Clin Auton Res. 2004;14(Suppl 1):S9-S17. doi:10.1007/s10286-004-1003-3
-
DiMario FJ Jr, Wheeler Castillo CS. Clinical categorization of childhood syncope. J Child Neurol. 2011;26(5):548-551. doi:10.1177/0883073810384864
-
Moya-I-Mitjans A, Rivas-Gandara N, Sarrias-Merce A, et al. Syncope. Rev Esp Cardiol. 2012;65(8):755-765.
-
Ciftci O, Kavalci C, Durukan P. Approach to patients with syncope in the emergency department: an evidence-based review. JAEM. 2014;13(2):82-91. doi:10.5152/jaem.2013.040
-
Kapoor WN. Evaluation and outcome of patients with syncope. Medicine (Baltimore). 1990;69(3):160-175. doi:10.1097/00005792-199005000-00004
-
Kapoor WN, Karpf M, Wieand S, et al. A prospective evaluation and follow-up of patients with syncope. N Engl J Med. 1983;309(4):197-204. doi:10.1056/nejm198307283090401
-
Hori S. Diagnosis of patients with syncope in emergency medicine. Keio J Med. 1994;43(4):185-191. doi:10.2302/kjm.43.185
-
Gilman JK. Syncope in the emergency department: a cardiologist’s perspective. Emerg Med Clin North Am. 1995;13(4):955-971. doi:10.1016/s0733-8627(20)30596-4
-
Bilici S, Sekmenli T, Göksu M, et al. Mean platelet volume in diagnosis of acute appendicitis in children. Afr Health Sci. 2011;11(3):427-432.
-
Güldiken B, Özkan H, Kabayel L. Akut iskemik inmede ortalama trombosit hacmi ve periferik kan hücre sayısı yanıtı. Trakya Univ Tip Fak Derg. 2008;25(2):130-135.
-
Tamer D, Fevzi Y, Deniz AE, et al. The value of serum mean platelet volume in ischemic stroke patients. J Pak Med Assoc. 2013;63(12):1509-1510.
-
Baron-Esquivias G, Martínez-Alday J, Martín A, et al. Epidemiological characteristics and diagnostic approach in patients admitted to the emergency room for transient loss of consciousness: GESINUR study. Europace. 2010;12(6):869-876. doi:10.1093/europace/euq018
-
Güldner S, Langada V, Popp S, et al. Patients with syncope in a German emergency department: description of patients and processes. Dtsch Arztebl Int. 2012;109(4):58-65. doi:10.3238/arztebl.2012.0058
-
Sarasin FP, Louis-Simonet M, Carballo D, et al. Prospective evaluation of patients with syncope: a population-based study. Am J Med. 2001;111(3):177-184. doi:10.1016/s0002-9343(01)00797-5
-
Kapoor WN. Syncope in older persons. J Am Geriatr Soc. 1994;42(4):426-436. doi:10.1111/j.1532-5415.1994.tb07493.x
-
Serletis A, Rose S, Sheldon AG, et al. Vasovagal syncope in medical students and their first-degree relatives. Eur Heart J. 2006;27(16):1965-1970. doi:10.1093/eurheartj/ehl147
-
Gracie J, Baker C, Freeston MH, et al. The role of psychological factors in the etiology and treatment of vasovagal syncope. Indian Pacing Electrophysiol J. 2004;4(2):79-84.
-
Disertori M, Brignole M, Menozzi C, et al. Management of patients with syncope referred urgently to general hospitals. Europace. 2003;5(3):283-291. doi:10.1016/s1099-5129(03)00049-7
-
Dow RB. The clinical and laboratory utility of platelet volume parameters. J Med Sci. 1994;15(2):1-15.
-
Ayrık C, Karcıoğlu Ö, Ersoy G, et al. Utilization of laboratory analyses in the workup of patients with syncope in the emergency department. Cerrahpasa Tip Derg. 2000;31(2):82-88.
-
Fouad-Tarazi F, Calcatti J, Christian R, et al. Blood volume measurement as a tool in syncope. Am J Med Sci. 2007;334(1):53-56. doi:10.1097/maj.0b013e318063c6f7
-
Park Y, Schoene N, Harris W. Mean platelet volume as an indicator of platelet activation: methodological issues. Platelets. 2002;13(5-6):301-306. doi:10.1080/095371002220148332
-
Papanas N, Symeonidis G, Maltezos E, et al. Mean platelet volume in patients with type 2 diabetes mellitus. Platelets. 2004;15(8):475-478. doi:10.1080/0953710042000267707
-
Henning BF, Zidek W, Linder B, et al. Mean platelet volume and coronary heart disease in hemodialysis patients. Kidney Blood Press Res. 2002;25(2):103-108. doi:10.1159/000063516
-
Çoban E, Ozdogan M, Yazicioglu G, et al. The mean platelet volume in patients with obesity. Int J Clin Pract. 2005;59(8):981-982.
-
Pizzulli L, Yang A, Martin JF, et al. Changes in platelet size and count in unstable angina compared to stable angina or noncardiac chest pain. Eur Heart J. 1998;19(1):80-84. doi:10.1053/euhj.1997.0747
-
Li D, Turner A, Sinclair AJ. Relationship between platelet phospholipid and mean platelet volume in healthy men. Lipids. 2002;37(9):901-906. doi:10.1007/s11745-002-0977-0
-
Smyth DW, Martin JF, Michalis L, et al. Influence of platelet size before coronary angioplasty on subsequent restenosis. Eur J Clin Invest. 1993;23(6):361-367. doi:10.1111/j.1365-2362.1993.tb02037.x
-
Ozdemir O, Soylu M, Alyan O, et al. Association between mean platelet volume and autonomic nervous system functions: increased mean platelet volume reflects sympathetic overactivity. Exp Clin Cardiol. 2004;9(4):243-247.
-
Kodiatte TA, Manikyam UK, Rao SB, et al. Mean platelet volume in type 2 diabetes mellitus. J Lab Physicians. 2012;4(1):5-9. doi:10.4103/0974-2727.98662
-
Turgut O, Zorlu A, Kilicli F, et al. Atrial fibrillation is associated with increased mean platelet volume in patients with type 2 diabetes mellitus. Platelets. 2012;24(6):493-497.
-
Davì G, Averna M, Catalano I, et al. Platelet function in patients with type 2 diabetes mellitus: the effect of glycaemic control. N Engl J Med. 1990;322:1769-1774. doi:10.1056/nejm199006213222503
-
Keating FK, Sobel BE, Schneider DJ. Effects of increased concentrations of glucose on platelet reactivity in healthy subjects and in patients with and without diabetes mellitus. Am J Cardiol. 2003;92(11):1362-1365. doi:10.1016/j.amjcard.2003.08.033
Tables
Table 1. The correlation between patient age and outcome
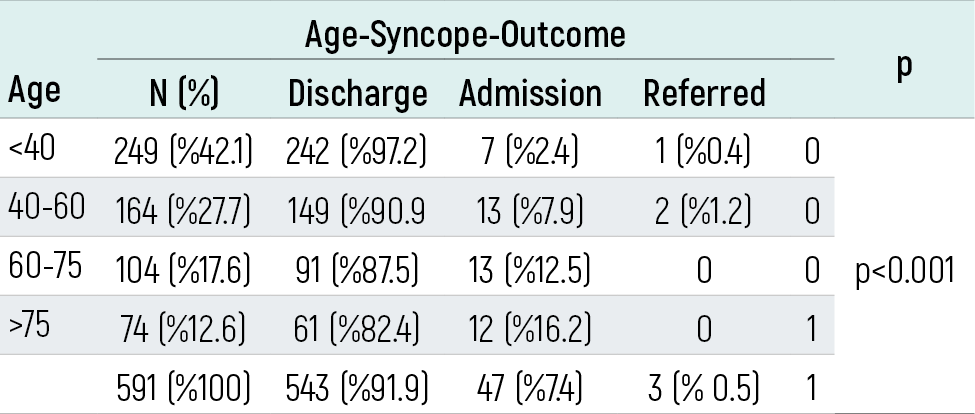
Table 2. Comparison of the groups with respect to Htc, Plt, and MPV
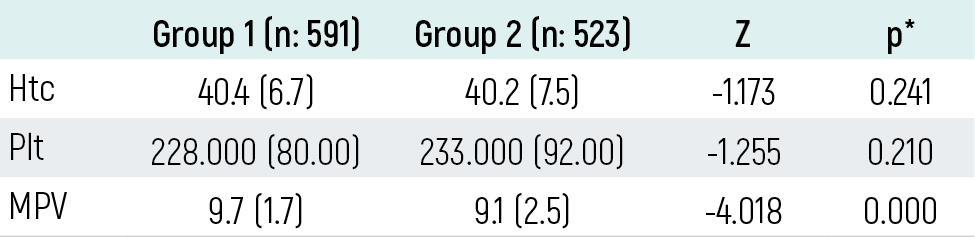
*Mann-Whitney U
Table 3. MPV levels in different syncope types
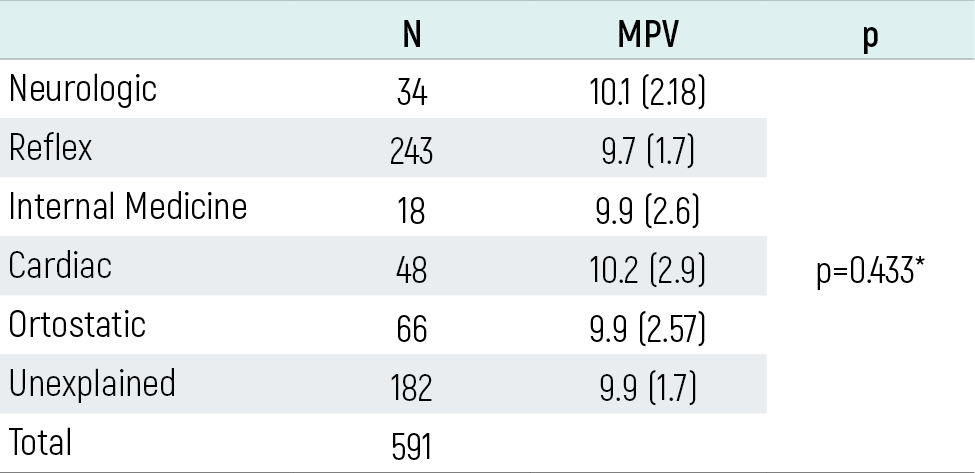
*Kruskall-Wallis test
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Metin Ozkan, Cemil Kavalci, Fevzi Yilmaz, M. Evvah Karakılıç, Bedriye Müge Sönmez, Turan Turhan, Cihat Yel, Ali Demir. Relationship between mean platelet volume and syncope. Eu Clin Anal Med 2015;3(1):1-4. doi:10.4328/ECAM.46
- Received:
- January 8, 2015
- Accepted:
- January 22, 2015
- Published Online:
- January 22, 2015
- Printed:
- January 22, 2015