Intrathoracic osteolipoma: A Case Report
Intrathoracic osteolipoma
Authors
Abstract
IntroductionLipomas are the most common benign soft tissue tumors. Although lipomas often appear in subcutaneous locations, they may develop in any part of the body. Case PresentationIntrathoracic osteolipomas and the malignant degeneration of osteolipomas are very rare. However, surgical resection is required for the diagnosis and treatment of lipomas. In this paper, we present a literature review and a rare intrathoracic osteolipoma case for which we performed a surgical resection. ConclusionComplete resection is the only definitive treatment and the only way of preventing relapse.
Keywords
Introduction
Lipomas are the most common benign soft tissue tumors. Although lipomas often appear in subcutaneous locations, they may develop in any part of the body. Intrathoracic lipomas are rare lesions that Fothergill first described in 1783. Intrathoracic osteolipomas are very rare.1,2,3 The literature we reviewed included a few reports of intrathoracic osteolipoma cases. In this paper, we present a literature review and a rare intrathoracic osteolipoma case for which we performed a surgical resection.
Case Presentation
A 30-year-old male patient without any active complaint underwent amputation above his right knee 16 years ago after a diagnosis of osteosarcoma. He did not receive postoperative chemotherapy or radiotherapy. During his follow-up visit, a mass showing progression on the right hemithorax, which appeared to be comparable to calcification within itself, was detected in his posteroanterior chest radiography (Figure 1a). Chest computed tomography (CT) showed a mass lesion with irregular margins containing widespread calcifications of 104x80x103mm extending posteriorly to the perihilar area of the right upper lobe (Figure 1b). Positron emission tomography (PET-CT) detected a mass with pleural-based widespread calcifications of 71x151mm with low-SUV involvement beginning at the right lung’s upper lobe posterior segment and extending to the middle lobe, he was then referred to our hospital for diagnosis and treatment. Physical examination of the patient showed that his right leg was amputated above the knee and he had diminished breathing sounds in the right hemithorax. His routine hemogram biochemical tests were normal. The mass contained calcified sections, so it was not deemed appropriate to perform a transthoracic needle aspiration biopsy. A right posterolateral thoracotomy was performed on the patient for diagnostic and therapeutic purposes.
During exploration, a well-circumscribed, encapsulated, solid mass was observed; this mass was located in a major fissure, compressed on the lower lobe, filled about one-third of the right hemithorax and did not show invasion to the surrounding tissue (Figure 2a). The mass was hard, so a frozen section could not be performed. The mass was completely excised, and lymph node sampling was performed. Macroscopy of the resected mass showed a cross-section with a hard consistency, which was partly consistent with fat tissue (Figure 2b,c). During the histopathological examination, benign lamellar bone spicules embedded in mature fat tissue were observed (Figure 2d). In line with these histopathological findings, the mass was reported to be osteolipoma. Lymph nodes 4 and 7 had a reactive, anthracotic appearance. Our patient was discharged on postoperative day 7 with no problems. The patient had no active complaints at his one-year follow-up visit, and no recurrence was detected.
Discussion
Lipomas are benign mesenchymal tumors.1 Heuer divided thoracic lipomas into three groups:
1) Dumbbell tumors, which are lesions with part of the intrathoracic mass linked to the mass in the extrathoracic region;
2) Lesions directly extending from the neck to the anterior superior mediastinum; and 3) Purely intrathoracic lesions, which have no link with any bone tissue.4 Our case belongs to the third group.
Intrathoracic lipomas develop from submesothelial adipose tissue in the parietal pleura, diaphragm, mediastinum, and extrapericardial area.5 Histologically, lipomas are composed of mature fat cells. However, they may also contain mesenchymal elements, including bone, cartilage, smooth muscle, or fibrous tissue. Depending on which elements are found, lipomas are referred to as osteolipomas, chondrolipomas, myelolipomas, fibrolipomas, or angiolipomas. Osteolipomas contain mature bone spicules and are rare histologic variants of lipomas.6,7
The pathogenesis of osteolipoma is unclear; however, two theories have been suggested. In the first theory, multipotent mesenchymal cells are considered similar to osteolipomas. In the second theory, repetitive trauma, metabolic changes, or ischemia are thought to lead to the metaplasia of fibrous elements contained in lipomas and the development of osteoblasts.6
Lipomas are encapsulated and grow slowly; therefore, they usually do not lead to symptoms. Symptoms vary depending on the location and size of the mass. They may compress the bronchial system, esophagus, vagus nerve, phrenic nerve, or other tissues within the thorax. Accordingly, symptoms such as shortness of breath, dry cough, orthopnea, dysphagia, chest pain, and cardiac arrhythmia may occur1,3. Jack et al. reported a case of left ventricular dysfunction that developed due to compression from an intrathoracic extrapericardial lipoma. The patient refused surgery, and cardiac arrest developed because of the mass.8 Our patient did not have any active complaints.
Lipomas can reach enormous sizes because they grow slowly. Yang et al. presented a case of the largest intrathoracic osteolipoma in the literature, measuring 26 × 19 × 12 cm, which was accidentally detected when the patient presented with complaints of dry cough and chest pain.3 The mass we excised measured 8 × 16 cm.
Intrathoracic lipomas are often asymptomatic, so they are usually detected incidentally in a posteroanterior chest radiograph. CT and magnetic resonance imaging (MRI) are used to make a diagnosis.1,5 Our patient had a history of above-knee amputation due to osteosarcoma, so he was followed using chest CT. Upon detection of mass growth during his follow-up visit, he was referred to our hospital for diagnosis and treatment.
Malignant degeneration of osteolipomas is very rare. Surgical resection is required for the diagnosis and treatment of lipomas. Complete resection is the only definitive treatment and the only way to prevent relapse.1,3 Accordingly, we performed a complete resection of the intrathoracic mass. Local recurrence is very rare in resected intrathoracic lipomas.1,3,6 The patient had no active complaints at his one-year follow-up visit, and no recurrence was detected.
In conclusion, osteolipomas are lipomas containing mature bone tissue. They show slow growth without any symptoms. Complete surgical resection is the only treatment. Intrathoracic osteolipomas are rare benign lesions. Only a few cases have been reported worldwide in this location, and none have been reported in the Turkish literature. The aim of this paper is to report the first intrathoracic osteolipoma in Turkish literature, according to our knowledge, and to review its clinical features and treatment.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments.
Informed Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the scientific content of the article, including the study design, data collection, analysis and interpretation, manuscript preparation, and approval of the final version of the manuscript.
References
-
Chen M, Yang J, Zhu L, Zhao H. Intrathoracic giant pleural lipoma: case report and review of the literature. J Cardiothorac Surg. 2013;8(1):196. doi:10.1186/1749-8090-8-196
-
Sulzer MA, Goei R, Bollen EC, Theunissen PH, Maesen FP. Lipoma of the external thoracic wall. Eur Respir J. 1994;7(1):207-209. doi:10.1183/09031936.94.07010207
-
Yang J, Li S, Kang A, et al. A giant intrathoracic osteolipoma: a case report and review of the literature. Int J Surg Case Rep. 2012;3(7):290-292. doi:10.1016/j.ijscr.2012.03.008
-
Heuer GJ. The thoracic lipomas. Ann Surg. 1933;98(5):801-819. doi:10.1097/00000658-193311000-00001
-
Gaerte SC, Meyer CA, Winer-Muram HT, Tarver RD, Conces DJ Jr. Fat-containing lesions of the chest. Radiographics. 2002;22(1):61-78. doi:10.1148/radiographics.22.suppl_1.g02oc08s61
-
Demiralp B, Alderete JF, Kose O, et al. Osteolipoma independent of bone tissue: a case report. Cases J. 2009;2:8711. doi:10.4076/1757-1626-2-8711
-
Saghafi S, Mellati E, Sohrabi M, et al. Osteolipoma of the oral and pharyngeal region: report of a case and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;105(6):e30-e34. doi:10.1016/j.tripleo.2008.02.018
-
Jack AI, Blohm ME, Lye M. An intrathoracic lipoma impairing left ventricular function. Br Heart J. 1995;74(1):95. doi:10.1136/hrt.74.1.95
Figures
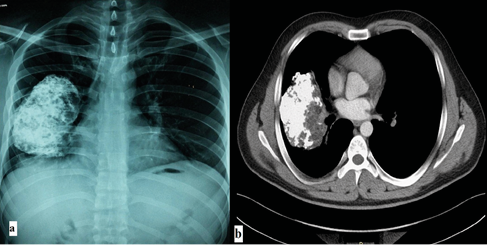
Figure 1. PA chest x-ray: Mass containing calcification in the right hemithorax(a), Chest CT: Mass containing calcification extending to the right perihilar area in the mediastinal window(b).
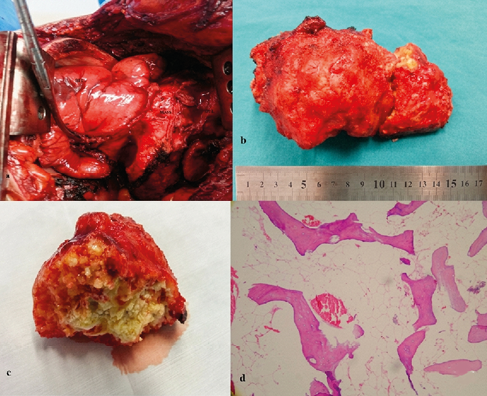
Figure 2. Intraoperative view of the mass(a); the excised mass(b); macroscopic view of the mass(c); microscopic view of the mass(d); lamellae consisting of bone spicules located in the fat tissue (HEX200).
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Leyla Nesrin Acar, Erkmen Gülhan, Pınar Bıçakçıoğlu, Arzu Ertürk, Funda Demirağ. Intrathoracic osteolipoma: A Case Report. Eu Clin Anal Med 2015;3(1):10-12. doi:10.4328/ECAM.43
- Received:
- December 3, 2014
- Accepted:
- January 24, 2015
- Published Online:
- January 24, 2015
- Printed:
- January 24, 2015