A 20-year-old patient with idiopathic non-sustained ventricular tachycardia: A Case Report
A patient with ventricular tachycardia
Authors
Abstract
IntroductionVentricular tachycardia occurring in persons without apparent heart disease is called idiopathic ventricular tachycardia. In this paper, we aimed to report a 20-year-old female subject without overt structural heart disease who presented with non-sustained ventricular tachycardia.
She was admitted to our emergency department with back pain for 16 hours. She gave no history of smoking, alcohol intake, illicit drug use, heavy consumption of caffeinated beverages, or severe bodily exercise.
Case PresentationAn electrocardiogram taken in the emergency department showed short bursts of a broad QRS tachycardia with monomorphic, left bundle branch block morphology complexes and an inferior axis. The patient’s tachycardia spontaneously terminated during the emergency department stay.
With the initial diagnosis of idiopathic ventricular tachycardia, the patient was discharged on metoprolol 50 mg PO after observing that her vital signs were stable and cardiac enzymes were negative.
ConclusionIdiopathic ventricular tachycardia should be considered in the differential diagnosis in cases presenting to the emergency department with palpitations, dizziness, chest or back pain, and syncope.
Keywords
Introduction
Ventricular tachycardia occurring in persons without apparent heart disease is called idiopathic ventricular tachycardia.1 Eighty percent of idiopathic monomorphic ventricular tachycardias originating from outflow tracts arise from the right ventricle, and they are of benign character.2
These arrhythmias are usually present electrocardiographically with broad, monomorphic QRS complexes; their mechanisms include all types of arrhythmia mechanisms, namely reentry, increased automaticity, and triggered activity.3
In this paper, we aimed to report a 20-year-old female subject without overt structural heart disease who presented with non-sustained ventricular tachycardia.
Case Presentation
A 20-year-old woman was admitted to our emergency department with back pain lasting for 16 hours. She had no chest pain or dyspnea. She reported that she occasionally noticed her pulse accelerating, but it did not cause significant discomfort. Her past medical history was remarkable for panic disorder. She denied smoking, alcohol intake, illicit drug use, heavy consumption of caffeinated beverages, or engaging in intense physical exercise. She had normal weight and height. She stated that she was under intense emotional stress due to her examination week.
Her relatives brought previous electrocardiograms and echocardiography performed by another cardiologist for complaints of palpitations. The old electrocardiogram showed normal sinus rhythm, and the old echocardiography demonstrated a floppy mitral valve.
On admission, her vital signs were: arterial blood pressure 142/97 mmHg, body temperature 36.8°C, pulse rate 126 beats per minute, respiration rate 20 breaths/minute, and pulse oxygen saturation 98%. Physical examination revealed a rapid heartbeat, but heart sounds were normal and no murmur was heard.
An electrocardiogram taken in the emergency department showed short bursts of broad QRS tachycardia with monomorphic, left bundle branch block morphology complexes and an inferior axis (Fig. 1). Focused cardiac ultrasonography (FOCUS) revealed mild mitral valve prolapse and first-degree mitral regurgitation.
Laboratory results were as follows: blood urea nitrogen 9 (6–19) mg/dL, creatinine 0.66 (0.5–1.2) mg/dL, sodium 135 (135–146) mmol/L, potassium 4 (3.5–5.2) mmol/L, CK-MB mass 0.6 (0–3.4) ng/mL, high-sensitivity troponin I 0.001 (<0.016) ng/mL, hemoglobin 14 (12–16) g/dL, leukocyte count 7.29 (4.5–11) ×10³/µL, thrombocyte count 326 (150–400) ×10³/µL. Blood gas analysis showed pH 7.43, blood glucose 95 mg/dL (70–110), carboxyhemoglobin 0.9% (0–2.5), lactate 1.2 mmol/L (0.5–1.6), and ionized calcium 1.15 (1.12–1.30) mmol/L.
The patient’s tachycardia spontaneously terminated during her stay in the emergency department. With the initial diagnosis of idiopathic ventricular tachycardia, she was discharged on metoprolol 50 mg PO after confirming stable vital signs and negative cardiac enzymes. She was recommended to follow up at the cardiology clinic.
Discussion
Herein, we report a 20-year-old patient presenting to our emergency department with non-sustained ventricular tachycardia. Her admission ECG showed a wide QRS tachycardia with a left bundle branch block pattern at a rate of 130 beats per minute, dominant R waves in the inferior leads, a QS pattern in V1, and a transition zone at V4. No overt structural heart disease was detected in the initial tests.
As in our patient, individuals with idiopathic ventricular tachycardia of outflow tract origin are typically hemodynamically stable and usually present with symptoms such as dizziness or palpitations. These tachycardias may occur as repetitive monomorphic non-sustained ventricular tachycardia attacks, as in our patient, or as sustained ventricular tachycardia episodes, often triggered by exercise or emotional stress. They are usually seen in individuals between 20 and 40 years of age, consistent with our patient.4
The pathophysiological mechanism underlying outflow tachycardias is thought to be triggered activity. They are also referred to as adenosine-sensitive ventricular tachycardias, although they respond to verapamil and beta blockers (most commonly propranolol, but also other beta blockers). Outflow tachycardias may originate from the right ventricular outflow tract or the left ventricular outflow tract, the latter sometimes involving areas around or within the aortic cusps. These tachyarrhythmias are usually benign, with sudden death being extremely rare. Thus, they are generally not treated aggressively, although life-limiting arrhythmias or syncopal episodes warrant therapy. In severely symptomatic cases, calcium channel blockers (mainly verapamil), beta blockers (mainly propranolol), or other antiarrhythmics (e.g., amiodarone, sotalol, propafenone) can be used, though potentially hazardous antiarrhythmics are rarely needed.5 In recent years, these arrhythmias have increasingly been treated definitively via radiofrequency catheter ablation.
In the emergency department, physicians should first exclude ischemia, electrolyte or acid-base disorders, and thyroid disease, followed by intoxications, particularly with tricyclic antidepressants, antiarrhythmics, digoxin, and some herbal products. Some patients with arrhythmogenic right ventricular dysplasia may present with outflow tachycardias mimicking the idiopathic variety, complicating diagnosis.
We deemed our patient symptomatic due to her emergency department admission, even though her primary complaint at the time was not palpitations. We started metoprolol succinate, given that her tachycardia was consistent with outflow tachycardia and she had minimal mitral valve prolapse. We did not consider urgent cardiology consultation for an electrophysiology study necessary; rather, we discharged the patient with the recommendation to see an electrophysiologist electively.
In conclusion, idiopathic ventricular tachycardia should be considered in the differential diagnosis of patients presenting to the emergency department with palpitations, dizziness, chest or back pain, and syncope. Ischemia, electrolyte and acid-base disorders, thyroid disease, and intoxications should be ruled out in every case, and structural heart disease should be assessed. Asymptomatic cases can be followed without specific therapy, while symptomatic cases may be treated with medical therapy or radiofrequency catheter ablation.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments.
Informed Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the scientific content of the article, including the study design, data collection, analysis and interpretation, manuscript preparation, and approval of the final version of the manuscript.
References
-
Simsek H, Dogan A, Sahin M, Gumrukcuoglu HA. A case of idiopathic ventricular tachycardia in a 14-year-old obese patient due to golden berry fruit extract pills for weight loss. Turk Kardiyol Dern Ars. 2013;41(5):429-432. doi:10.5543/tkda.2013.83548
-
Lerman BB. Outflow tract ventricular arrhythmias: an update. Trends Cardiovasc Med. 2015. doi:10.1016/j.tcm.2015.01.011
-
Aksu T, Guler TE, Golcuk E, Ozcan KS, Erden I. Ablation of idiopathic ventricular tachycardia originating from posterior mitral annulus by using electroanatomical mapping. Int Med Case Rep J. 2015. doi:10.2147/imcrj.s79519
-
Kilicaslan F, Uz O, Tokatli A, Isilak Z. Radiofrequency catheter ablation of idiopathic ventricular tachycardia originating from the mitral annulus. Turk Kardiyol Dern Ars. 2012;40(5):436-439. doi:10.5505/tkda.2012.36974
-
Dogan M, Karagoz T, Celiker A. Radiofrequency catheter ablation in children with idiopathic ventricular tachycardia. Turk Arch Pediatr. 2007;5(3):238-243.
Figures
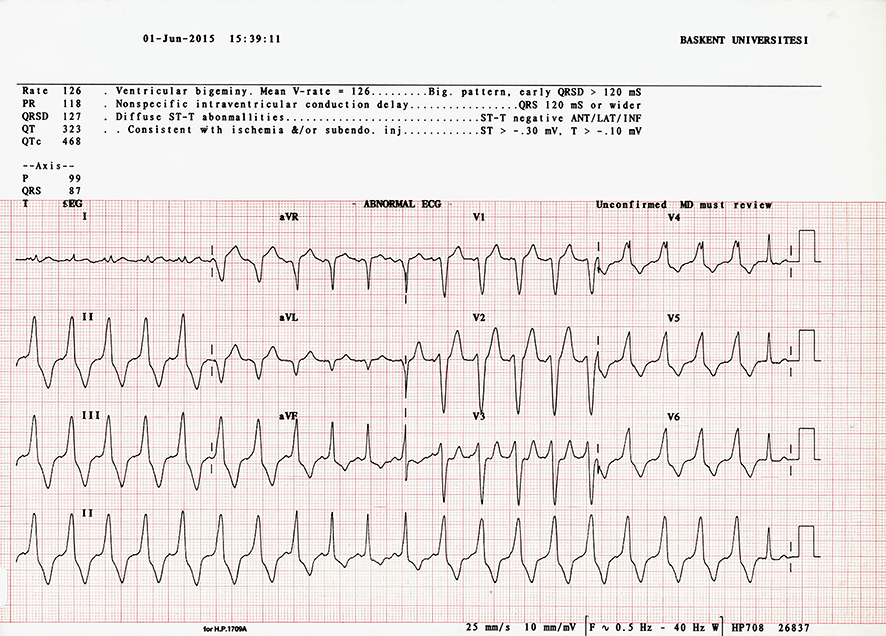
Figure 1. The admission ECG of the patient
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Afsin Emre Kayipmaz, Orcun Ciftci, Cemil Kavalci, Betul Akbuga Ozel, Elif Celikel. A 20-year-old patient with idiopathic non-sustained ventricular tachycardia: A Case Report. Eu Clin Anal Med 2013;3(3):27-29. doi:10.4328/ECAM.56
- Received:
- August 4, 2015
- Accepted:
- August 4, 2015
- Published Online:
- September 1, 2013
- Printed:
- September 1, 2013