Succesful surgical treatment of a right atrial myxoma associatedwith pulmonary embolism: A Case Report
Surgical treatment of a right atrial myxoma
Authors
Abstract
IntroductionIn all of the tumors seen in humans, cardiac tumors have a very low incidence of approximately 0.2%. These tumors are mainly metastatic in origin, with only a small percentage being primary tumors.
Case PresentationWe present the case of a 30-year-old male patient with a right atrial mass who presented with an acute pulmonary embolism. The patient underwent a right atrial mass resection with concomitant pulmonary thrombectomy. Pathological examination revealed a right atrial myxoma.
ConclusionIn this case report, we discuss this rare tumor using preoperative and perioperative imaging obtained via transthoracic and transesophageal echocardiography.
Keywords
Introduction
Cardiac tumors can be primary, secondary, or metastatic, and they represent only 0.2% of all tumors seen in humans.1 Primary intracardiac tumors are rarely found; approximately 75% are benign, and of those, 50% are myxomas.
Myxomas derive from multipotent mesenchymal cells of the subendocardium.1,2 While they are most commonly seen in the left atrium, they can arise in other locations, such as the right atrium (RA), in 15 to 20% of cases.3
Depending on the mobility, size, and location of the tumor, symptoms are often atypical and highly variable, which can lead to diagnostic confusion and a significant delay in diagnosis. When located in the RA, a myxoma can rarely manifest as a pulmonary embolism, as seen in our case.
Case Presentation
A 30-year-old man presented with a sudden episode of dyspnea, palpitation, and atypical chest pain. He had also suffered from weight loss and intermittent feeling faint for the past one year.
Physical examination was unremarkable. Chest X-ray showed moderate enlargement of the cardiac silhouette with normal pulmonary fields. Standard electrocardiogram showed sinus tachycardia with a heart rate of 120 bpm and incomplete right bundle branch block. D-dimer value was in the normal range (192 ng/ml).
Contrast-enhanced computed tomography (CT) revealed partial obstruction of the right pulmonary artery, while the main pulmonary artery was free of lesion. Venous Doppler study of the lower extremity showed normally functioning deep veins with no sign of acute or chronic deep vein thrombosis.
After the completion of these tests, the clinic of chest diseases hospitalized the patient and initiated anticoagulant and antiaggregant therapy for PE. The D-dimer values stayed constant and the complaints of the patient did not decrease. They consulted the patient to us, and a transthoracic echocardiogram (TTE) was planned.
TTE revealed a 30x24 mm moving mass attached to the interatrial septum of the right atrium and slightly reduced right ventricular function, but it could not differentiate whether the mass was a tumor or a thrombus.
Thus, a transesophageal echocardiography (TEE) was conducted. It revealed a 40x27 mm mobile mass with multilobular heterogeneous echogenicity attached to the interatrial septum of the right atrium, which was prolapsing through the leaflets of the tricuspid valve during diastole and not affecting the blood flow in the superior or inferior vena cava. In light of these findings, we admitted the patient to our clinic.
After taking written informed consent, open-heart surgery was arranged. A standard midline sternotomy incision was performed. Following full systemic heparinization, ascending aortic and bicaval selective cannulation—using two standard 28-Fr venous return cannulas to avoid tumor embolization—established cardiopulmonary bypass. Myocardial protection was provided by antegrade cold crystalloid cardioplegia and moderate systemic hypothermia (28°C). The right atrium was opened, and a large pedunculated tumor originating from the atrial septum was removed with a cuff of normal adjacent septum tissue. The resected mass was sent for histological assessment. The iatrogenic atrial septal defect was repaired using a pericardial patch.
After that, the main pulmonary artery was opened under intermittent total circulatory arrest (7 min in total), and a 1-cm-diameter tumor fragmentation was removed from the right pulmonary artery. Arteriotomy of the pulmonary artery was closed and the procedure was concluded. Perioperative TEE confirmed normal function of the tricuspid valve and the absence of residual masses.
The patient was transferred to the intensive care unit with 5-μg/kg/min dobutamine infusion. The postoperative course was uncomplicated, and the patient was discharged on the postoperative 7th day. The histopathologic examination confirmed the tumor etiology as a myxoma.
Ten days after discharge, the patient was admitted to our clinic suffering from atrial fibrillation with rapid ventricular response. Normal sinus rhythm was established by intravenous amiodarone. Follow-up TTE revealed a normally functioning tricuspid valve and a pulmonary artery pressure of 27 mmHg with no sign of residual mass.
Discussion
Myxoma is the most prevalent primary cardiac tumor. The incidence of RA localization is low. Yu and colleagues retrospectively reviewed 33108 patients who underwent open-heart surgery and reported 234 cases with a confirmed diagnosis of primary heart tumor (0.71%). Among 184 patients with myxoma, RA localization was found only in 12 (6.5%) cases.4 RA myxomas generally originate in the fossaovalis or base of the interatrial septum.5 In regard to the macroscopic aspect, 83% of myxomas are polypoid and pedunculated tumors with a predominant brownish color, as in our case.3
Myxomas usually present themselves insidiously resulting in a delay in their diagnostic and surgical management. They may appear with obstruction symptoms due to blood flow blockade or with symptoms due to embolism, arrythmia and constitutional symptoms due to tumor embolization and /or complement activation from circulating antibody tumor antigen complexes.6
Embolization from a thrombotic material from deep veins, right heart chambers or catheter tips are the most common reasons of pulmonary embolism. D-dimer levels are usually elevated in plasma in the presence of acute trombosis, because of simultaneous activation of coagulation and fibrinolysis. The negative predictive value of D-dimer testing is high and a normal D-dimer level renders acute PE or deep vein thrombosis. Furthermore, cancer or inflammation can produce fibrin also. According to the 2014 ESC Guideline on the diagnosis and management of acute PE, if there is suspected PE without shock or hypotension and if the D-dimer is negative, no treatment is suggested.7 Embolism occurs in approximately 10% cases of RA myxoma, and even pulmonary embolism of tumor fragments or thrombus from the tumor surface can occur, as in our case.
However, as depicted in our case, although the patient has non-spesific symptoms and D-dimer is normal, TTE evaluation should be planned in every patient with pulmonary embolism. In our case, TTE revealed a 30x24 mm moving mass attached to the interatrial septum of the right atrium and slightly reduced right ventricular function. In our experience, TEE should be considered in patients with RA masses which were demonstrated with TTE because its sensitivity is better than TTE, computed tomography or magnetic resonance imaging.8 Also we strongly recommend to use TEE during surgery because it provides useful information to secondary valve damage caused by the tumor or to diagnose rare biatrial or multilocular myxomas.
Complete removal of the tumor and its implantation base with a good safety margin is important for maintaining contractibility, preventing pulmonary embolism and recurrence and restoring dilatation functions of bilateral atria. In this case, the tumor was located in fossaovalis of RA and removed with a cuff of normal adjacent septum tissue. Pulmonary embolectomy is a surgical procedure that evolved in the last 20 years. The procedure should be considered in cases of myxoma associated with PE in order to prevent right ventricule dysfunction and to improve patient symptoms.
Conclusion
RA is an unusual loaction for myxoma and it has a potential of pulmonary embolism. Although the patient has non-spesific symptoms and D-dimer is normal, TTE evaluation should be planned in every patient with pulmonary embolism. TEE is a sufficient and reliable technique for diagnosis and evaluation of shape, size and the origin of the myxoma. It is also an adequate guide to surgical treatment. RA myxoma associated with pulmonary embolism should urgently be treated with surgical removal and pulmonary embolectomy.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments.
Informed Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the scientific content of the article, including the study design, data collection, analysis and interpretation, manuscript preparation, and approval of the final version of the manuscript.
References
-
Arruda MV, Braile DM, Joaquim MR, Soares MJ, Alves RH. Resection of left ventricular myxoma after embolic stroke. Rev Bras Cir Cardiovasc. 2008;23(4):578-580.
-
Jang KH, Shin DH, Lee C, Jang JK, Cheong S, Yoo SY. Left atrial mass with stalk: thrombus or myxoma? J Cardiovasc Ultrasound. 2010;18(4):154-156. doi:10.4250/jcu.2010.18.4.154
-
Nina VJS, Silva NAC, Gaspar SFD, et al. Atypical size and location of a right atrial myxoma: a case report. J Med Case Rep. 2012;6:26. doi:10.1186/1752-1947-6-26
-
Yu K, Liu Y, Wang H, Hu S, Long C. Epidemiological and pathological characteristics of cardiac tumors: a clinical study of 242 cases. Interact Cardiovasc Thorac Surg. 2007;6:636-639. doi:10.1510/icvts.2007.156554
-
Stolf NA, Benicio A, Moreira LF, Rossi E. Right atrial myxoma originating from the inferior vena cava: an unusual location with therapeutic and diagnostic implications. Rev Bras Cir Cardiovasc. 2000;15:255-258.
-
Canale LS, Colafranceschi AS, Botelho ESL, Monteiro AJO. Surgical treatment of right atrial myxoma complicated with pulmonary embolism. Interact Cardiovasc Thorac Surg. 2009;9(3):535-536. doi:10.1510/icvts.2009.206318
-
European Society of Cardiology. ESC guidelines on the diagnosis and management of acute pulmonary embolism. Eur Heart J. 2014. doi:10.15829/1560-4071-2015-8-67-110
-
Leibowitz G, Keller NM, Daniel WG, et al. Transesophageal versus transthoracic echocardiography in the evaluation of right atrial tumors. Am Heart J. 1995;130(6):1224-1227. doi:10.1016/0002-8703(95)90146-9
Figures
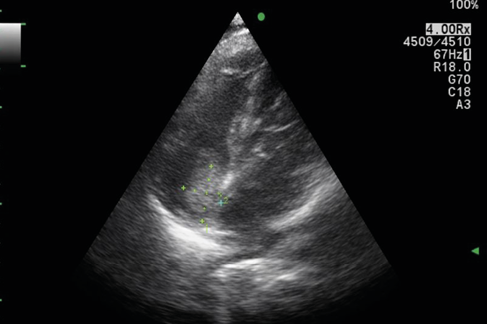
Figure 1. Preoperative TTE image of right atrial myxoma
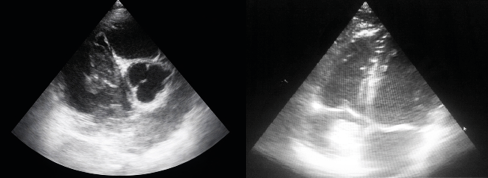
Figure 2. Preoperative TEE image of right atrial myxoma video1 and video 2. preoperative moving TEE image of right atrial myxoma
transesophageal echocardiography image of right atrial myxoma

Figure 3. Perioperative image of right atrial myxoma

Figure 4. Perioperative TEE image after from right atrial myxoma Video 3. perioperative moving TEE image after from right aright atrial myxoma
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Kemal Korkmaz, Ali Baran Budak, Serhat Bahadır Genç, Hikmet Selçuk Gedik, Kerim Çağlı. Succesful surgical treatment of a right atrial myxoma associatedwith pulmonary embolism: A Case Report. Eu Clin Anal Med 2014;2(2):12-14. doi:10.4328/ECAM.37
- Received:
- September 14, 2014
- Accepted:
- September 14, 2014
- Published Online:
- September 16, 2014
- Printed:
- September 16, 2014