Late posttraumatic tricuspid valve insufficiency repaired by artificial cordae: A Case Report
Posttraumatic tricuspid insufficiency repaired by artificial cordae
Authors
Abstract
IntroductionWe report the case of a 45-year-old female who was referred to our clinic with dyspnea and palpitation.
Case PresentationWe learned from the patient history that she had sustained a car accident 15 years ago. Transthoracic echocardiography revealed rupture of the anterior tricuspid leaflet and prolapse of the mitral valve, causing severe tricuspid and moderate mitral valve regurgitation.
The mitral valve was repaired with artificial chordae replacement and ring annuloplasty. The tricuspid valve was also repaired with anterior tricuspid leaflet triangular plication and ring annuloplasty after artificial chordae implantation. The longitudinal right atrial incision was sutured vertically, and the right atrium size was reduced with plication.
ConclusionFirst and sixth-month echocardiographic follow-ups showed trivial tricuspid insufficiency without any complaints.
Keywords
Introduction
Posttraumatic tricuspid insufficiency (TI) due to rupture of the chordal structure of the tricuspid valve (TV) is a very rare entity and mostly caused by blunt chest trauma. Clinical symptoms are generally mild and the hemodynamic consequences are often well-tolerated, so most of the cases have been diagnosed and treated several years after initial trauma.1
Posttraumatic TI can be caused by several reasons such as annular detachment of leaflets, anterior leaflet chordae rupture and papillary muscle rupture.2,3,4
Here we present the surgical repair of tricuspid and mitral valve regurgitation which was caused by blunt chest trauma 15 years ago.
Case Presentation
A 45-year-old female patient was referred to our hospital with complaints of progressive dyspnea and palpitation. She did not have any reported medical problem; however, we learned that she had suffered from blunt chest trauma 15 years ago because of a car accident.
A detailed physical examination revealed a grade 3-4/6 pansystolic murmur along the left lateral sternal border. Chest X-ray revealed an enlarged cardiac silhouette. Transthoracic echocardiography (TTE) showed severe (4+) TI with severe right ventricular dilatation, right atrial dilatation (8.9x9.0 cm), rupture of the chordae of the anterior tricuspid valve leaflet and moderate (2+) mitral insufficiency due to mitral valve prolapse. Right ventricular ejection fraction was 56%.
Further investigations with cardiac catheterization and coronary angiography revealed normal coronary arteries. Magnetic resonance imaging (MRI) was planned for the patient, and MRI confirmed right ventricular dilatation with a major axis of 8.9 cm and a minor axis of 5.5 cm. On the basis of these findings, medical treatment was established with b-blockers and diuretics, and surgery was planned (Figure 1).
OperationA standard midline sternotomy incision was performed. After pericardiotomy, a giant right atrium was observed. After full systemic heparinization, cardiopulmonary bypass was established by aortic and bicaval cannulation. Myocardial protection was provided by antegrade/retrograde cold crystalloid cardioplegia, topical cooling, and moderate systemic hypothermia.
The right atrium was opened with a horizontal incision. The mitral valve was evaluated via the atrial septum (transseptal approach), and anterior mitral valve prolapse was observed. Prolapse of the anterior leaflet of the mitral valve was repaired with artificial chordal replacement. The loop technique, which uses the Hegar dilator to prepare loops of artificial neo-chordae, was previously described.12
Mitral valve repair was completed by the application of a flexible mitral ring, and the iatrogenic atrial septal defect was primarily sutured. A saline injection test was made to control the coaptation.
After completion of mitral valve repair, the tricuspid valve was examined. There was a flail anterior tricuspid leaflet due to ruptured chordae (Figure 2, a). Furthermore, secondary chordae were tethering and restraining the motion of the anterior leaflet. Tethering secondary chordae were cut to improve the motion of the anterior leaflet.
The same artificial chordal loop technique was used for the corrective repair, which was completed by flexible ring annuloplasty (Figure 2 b, c, d). Triangular resection and plication were performed (Figure 2, e). A saline injection test was made to control the coaptation (Figure 2, f).
After completion of the mitral and tricuspid valve repair, the horizontal right atrial incision was plicated vertically (Figure 2 g). A two-chambered atrium, consisting of a caval part and a functional right atrium, was created to reduce the size (Figure 2 h). Following declamping, normal sinus rhythm was obtained, and decannulation was performed without any hemodynamic problem.
The postoperative period was uneventful, and the patient was discharged on the postoperative 7th day. Follow-up transthoracic echocardiographic studies, performed at the 1st and 6th months postoperatively, revealed normally functioning valves (Movie 1).
Discussion
Blunt chest-wall trauma is common during traffic accidents. Traumatic cardiac injuries include myocardial contusion, pericardial effusion, injuries of great vessels or coronary arteries and valvular disruptions. Among valvular injuries, the aortic valve is the most frequently affected valve.2,5,6
A sudden antero-posterior compression generates a severe tension and a regurgitant jet that can result in the rupture of papillary muscle and/or chordae tendinae, especially during the end-diastolic phase. Furthermore, valvular disruption can occur over time because of inflammation, necrosis or contusion of the papillary muscles or chordae tendineae.1,7
There is an ongoing debate in the use of echocardiography as a screening tool in patients who are suffering from blunt chest wall trauma. Furthermore, both TTE and transesophageal echocardiography (TEE) have their limitations, though the diagnostic value of TEE is 56% and upon TTE, the yield is lower.6 We suggest repeat examinations or the application of other imaging methods if clinical suspicion exists.
Traumatic TI is a very rare condition but the true frequency of this disease is probably underestimated because of a possible long asymptomatic phase.8,9 Patients become symptomatic following dilatation of right cardiac chambers and the annular dilatation. Mitral valve involvement contributes to the progressive dilatation resulting in right ventricular failure.
Functional TI is more amenable for repair to preserve the right ventricular function. Right atrial dilatation over 8 cm and right ventricular dilatation over 5.5 cm is a challenging situation. However, tricuspid valve repair is superior with lower mortality and freedom from reoperation rates.10,11
Precise measurement of artificial chordae length and adequate plication of the leaflet without reducing the valve area and increasing the coaptation zone were the key pitfalls in this successful repair. Short-term results show this method can be used even in delayed cases of posttraumatic TI with ventricular and atrial dilatation.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments.
Informed Consent
Informed consent was obtained from all participants.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the scientific content of the article, including the study design, data collection, analysis and interpretation, manuscript preparation, and approval of the final version of the manuscript.
References
-
Bortolotti U, Scioti G, Milano A, Guglielmi C, Benedetti M, Tartarini G, et al. Post-traumatic tricuspid valve insufficiency: 2 cases of delayed clinical manifestation. Tex Heart Inst J. 1997;24(3):223-225.
-
Correia PM, Coutinho GF, Antunes MJ. Severe tricuspid regurgitation after traumatic papillary muscle rupture. Eur J Cardiothorac Surg. 2012;41(5):128. doi:10.1093/ejcts/ezs095
-
Lin SJ, Chen CW, Chou CJ, Liu KT, Su HM, Lin TH, et al. Traumatic tricuspid insufficiency with chordae tendinae rupture: a case report and literature review. Kaohsiung J Med Sci. 2006;22(12):626-629. doi:10.1016/s1607-551x(09)70363-8
-
Mehrotra D, Dalley P, Mahon B. Tricuspid valve avulsion after blunt chest trauma. Tex Heart Inst J. 2012;39(5):668-670.
-
Bernabeu E, Mestres CA, Lama-Osorio P, Josa M. Acute aortic and mitral valve regurgitation following blunt chest trauma. Interact Cardiovasc Thorac Surg. 2004;3(1):198-200. doi:10.1016/s1569-9293(03)00267-6
-
Ismailov RM, Weiss HB, Ness RB, Lawrence BA, Miller TR. Blunt cardiac injury associated with cardiac valve insufficiency: trauma links to chronic disease? Injury. 2005;36(9):1022-1028. doi:10.1016/j.injury.2005.05.028
-
Kulik A, Al-Saigh M, Yelle JD, Rubens FD. Subacute tricuspid valve rupture after traumatic cardiac and pulmonary contusions. Ann Thorac Surg. 2006;81(3):1111-1112. doi:10.1016/j.athoracsur.2004.12.027
-
Emmert MY, Pretre R, Suendermann S, Weber B, Bettex DA, Hoerstrup SP, et al. Severe traumatic tricuspid insufficiency detected 10 years after blunt chest trauma. Clin Res Cardiol. 2011;100(2):177-179. doi:10.1007/s00392-010-0219-6
-
Furukawa N, Hakim-Meibodi K, Gummert J. Isolated latent tricuspid regurgitation caused by blunt trauma. Thorac Cardiovasc Surg. 2011;59(8):497-499. doi:10.1055/s-0030-1250723
-
Said SM, Burkhart HM, Schaff HV, Johnson JN, Connolly HM, Dearani JA. When should a mechanical tricuspid valve replacement be considered? J Thorac Cardiovasc Surg. 2014;148(2):603-608. doi:10.1016/j.jtcvs.2013.09.043
-
Mestres CA, Fita G, Parra VM, Pomar JL, Bernal JM. Tricuspid valve surgery. HSR Proc Intensive Care Cardiovasc Anesth. 2012;4(4):261-267.
-
Cagli K. A simple method of making artificial chordal loops for mitral valve repair. Ann Thorac Surg. 2010. doi:10.1016/j.athoracsur.2009.11.055
Figures
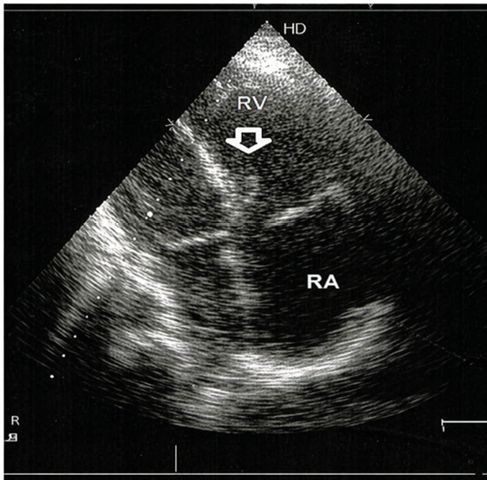
Figure 1. Tricuspid valve, flail anterior leaflet (arrow). (RA right atrium, RV right ventricle)
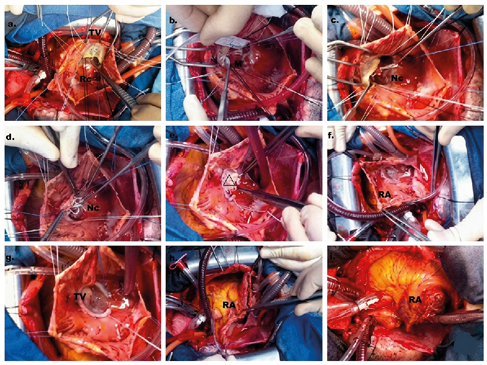
Figure 2. Tricuspid valve repair; [a: Ruptured cordae (Rc), b: Edge to moderator band (M) measure of neo-cordae, c: Implantation of neo-chordae loops stem to moderator band (M), d: Neo-chordae attachments to TV edges, e: Triangular plication of prolabe tricuspid valve (TV), f: Right atrial (RA) view after valvuloplasty, g: Coaptation test, h: Right atrial closure technique, i: New double chambered right atrium. ] Movie 1. Tricuspid Valve, Postoperative Doppler Echocardiography
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Kemal Korkmaz, Serhat Bahadır Genç, Ali Baran Budak, Hikmet Selçuk Gedik, Kerim Çağlı. Late posttraumatic tricuspid valve insufficiency repaired by artificial cordae: A Case Report. Eu Clin Anal Med 2014;2(3):23-25. doi:10.4328/ECAM.36
- Received:
- September 13, 2014
- Accepted:
- September 17, 2014
- Published Online:
- September 19, 2014
- Printed:
- September 19, 2014