Analysis of 54 patients who underwent thoracoscopic sympathectomy
Analysis of 54 sympathectomy performed patients
Authors
Abstract
AimThoracoscopic sympathectomy is performed with a high success rate and low morbidity for the treatment of primary hyperhidrosis. However, compensatory sweating remains the most commonly reported side effect. In this study, we aimed to present our experience with thoracoscopic sympathectomy in 54 patients who were operated at various levels of the sympathetic trunk.
MethodsMedical records of 61 patients who underwent thoracoscopic sympathectomy for primary hyperhidrosis were analyzed retrospectively. Seven patients were excluded because of one-sided operations. Variables such as age, sex, indications for surgery, level of resection, type of resection, number of ports, complications, and hospitalization time were recorded. We contacted all patients except four via telephone.
ResultsA total of 54 patients were treated between January 2006 and December 2008. There were 44 males and 10 females. The median age was 24.3 years (range 17–37). All 54 patients with primary symptoms of palmar and axillary hyperhidrosis reported excellent satisfaction (100%).
Compensatory sweating was reported in:6 (100%) of the T3-4-5 group16 (53%) of the T2-3 group3 (21%)** of the T2 group
The mean hospitalization time was 2.7 days (range 2-8). Compensatory sweating was significantly higher when the sympathetic trunk resection was longer.
ConclusionThoracoscopic sympathectomy is the cornerstone of treatment for primary hyperhidrosis, offering low morbidity and a high satisfaction rate. However, serial studies are needed to further evaluate the relationship between compensatory sweating and the specific resection level of the sympathetic trunk.
Keywords
Introduction
Thoracoscopic sympathectomy (TS) is performed with a high success rate in the treatment of palmar hyperhidrosis. Currently, this procedure is commonly performed by thoracic surgeons. The success rate of this minimally invasive approach is significantly high; however, compensatory hyperhidrosis (CH) remains the most commonly reported side effect with severe and debilitating symptoms.1,2
There are many literature findings about how to decrease the rate of CH. The incidence of CH varies in sympathetic ganglia resected patients when searched in the literature. The discussion is focused on the level and size of resection of the thoracic sympathetic chain, but unfortunately, no consensus has been achieved about this subject up until now.
In this study, we aimed to present our patients, who were treated with TS for hyperhidrosis, along with the literature findings.
Materials and Methods
A total of 61 patients were analyzed retrospectively who were treated in our institution for hyperhidrosis between January 2006 and December 2008. Seven patients were excluded because of one-sided operations. Four patients, who were treated via axillary thoracotomy on one side and via VATS (Video-Assisted Thoracoscopic Surgery) on the other, were included in the study because the aim was to investigate the long-term effects of sympathectomy.
The variables such as age, sex, indications, level and size of resection, type of resection, number of ports, complications, and hospitalization time were recorded. We contacted all patients except four via telephone. We interviewed them regarding recurrence, compensatory hyperhidrosis (CH), and if CH occurred, how it affected their quality of life. At the end of the interview, we asked if they would still have accepted the operation knowing the side effects they are experiencing now. All answers were recorded.
Results
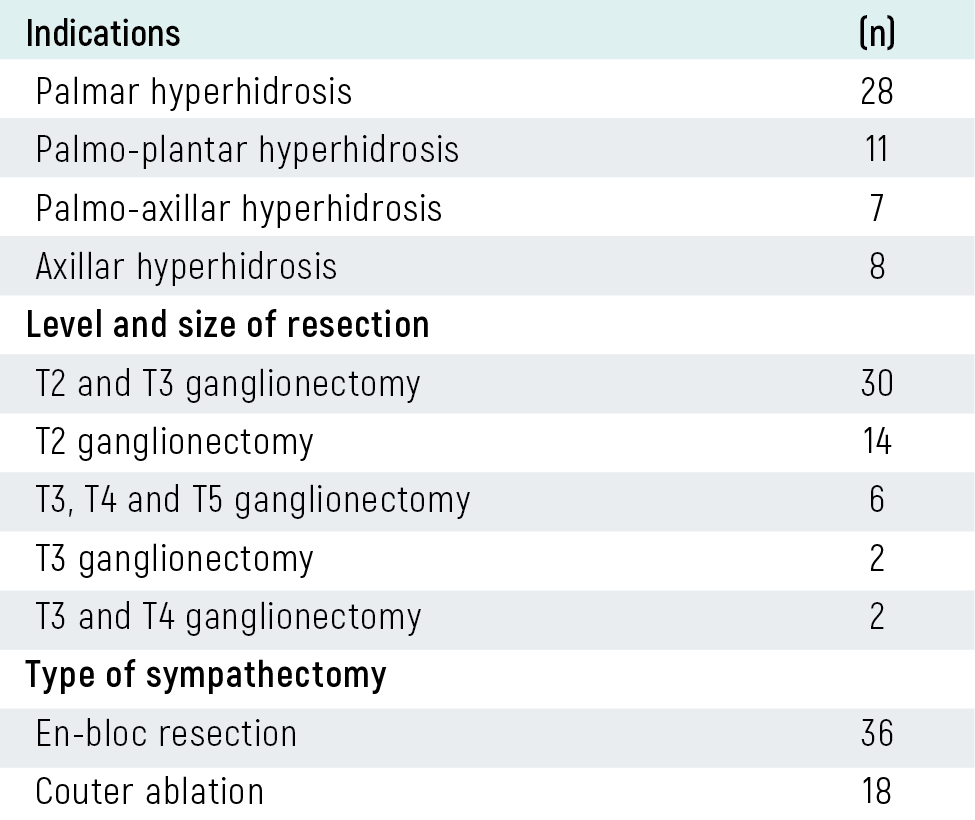
There were 44 male and 10 female patients in our study. The mean age was 24.3 years (range 17–37). Palmar hyperhidrosis was the most common indication, and all the other indications were summarized in Table 1. T3 ganglionectomy was the most common level of resection; the other levels and types of the resections were also summarized in Table 1.
En-bloc resection for the thoracic nerve and ganglia was performed in 36 patients, and cautery ablation was performed in 16 patients. Surgery via VATS through one port was performed in 10 patients, two ports in 31 patients, and three ports in 9 patients; four patients underwent axillary thoracotomy from one side and VATS from the other side.
Early postoperative complications were prolonged air leak in one patient, mild ptosis in two patients, hemorrhage in one patient, and recurrence in two patients. Hemorrhage and recurrence were treated during the same hospitalization period. The mean hospitalization time was 2.7 days (range 2–8). We performed two-staged operations in 3 patients; the reason for the two-staged operation was a decrease in the heart rate below 45 beats per minute.
Fifty of the 54 patients who were contacted via telephone reported that hyperhidrosis had ceased. We found that the success rate of TS for hyperhidrosis is 100%. Compensatory hyperhidrosis (CH) was determined in about 46.3% (n=25) of all patients. The localizations of CH include the chest, back, and face. Primary symptoms of palmar and axillary hyperhidrosis reported excellent satisfaction.
Compensatory sweating was reported in 6 (100%) of the T3-4-5 group, 16 (53%) of the T2-3 group, and 3 (21%) of the T2 group. CH was determined to cause a decrease in the quality of life in all of the T3-4-5 group and in 7 of the T2-3 group. We also determined that CH was significantly higher when we resected the sympathetic trunk longer.
Discussion
Thoracoscopic sympathectomy, which is regarded as the most effective therapy for idiopathic or primary hyperhidrosis, has gone through different stages regarding the placement and number of ports, as well as the resection level of the sympathetic trunk. The position of the patient, multiple incisions, resection of the T2, T3, and T4 ganglions, and the insertion of chest tubes were the main discussion points in the treatment of primary hyperhidrosis twenty years ago. At that time, the effectiveness and complication rates of treatment were compared according to supraclavicular, posterior, anterior, and axillary approaches.3 Currently, the treatment of primary hyperhidrosis is achieved with one-port microthoracoscopic sympathectomy, and patients are often discharged on the same day4ƒ The most common and serious side effect remains compensatory hyperhidrosis (CH). Many efforts to reduce CH and determine its contributing factors have been undertaken during surgical procedures.
Compensatory hyperhidrosis is an important side effect with a wide range of occurrence in the literature. In a study by Licht and Pilegaard, and another study by Reisfeld et al., CH was found in 89% and 83% of cases, respectively.5,6 Sugimura et al. reported the outcomes of 727 patients who underwent T2 ganglionectomy (399 patients), T2+3 ganglionectomy (55 patients), and T3+4 ganglionectomy (273 patients). Severe compensatory hyperhidrosis was reported in 15% of the T2 group, 24% of the T2+3 group, and 8% of the T3+4 group.7 Liu et al. reported the results of 141 consecutive patients with primary hyperhidrosis divided into two therapeutic groups: T3 sympathicotomy and T4 sympathicotomy. Both are effective for the treatment of primary hyperhidrosis, but T4 sympathicotomy decreases side effects without compromising the therapeutic effect. They recommended T4 sympathicotomy as the method of choice.8 In our series, we performed two redo operations due to the non-cessation of sweating in the early postoperative period. Palmar sweating improved in all patients contacted via telephone, resulting in a success rate of 100% (n=50 patients). We believe the results of different level sympathectomies on symptoms are nearly equal, but CH is the most common and annoying side effect that should be the focus of hyperhidrosis treatment.
Cardiac arrest is a rarely seen and frightening complication, with three case reports existing in the literature. One occurred intraoperatively, another occurred two years after bilateral sympathectomy, and the last occurred 24 hours after a left thoracic sympathectomy; permanent atrial pacing was required for two of them.9 It is emphasized that surgeons must be careful when performing bilateral thoracic sympathectomy on patients with a history of vagal syncope. Additionally, a decrease in heart rate of approximately 12% has been noted after bilateral procedures.10
In our cases, only 3 patients underwent sympathectomy on the right side first and then the other side at a different time. The reason for this delayed surgery was a decrease in heart rate below 50 bpm after the initial right-sided sympathectomy. Görür and co-workers performed bilateral sympathectomy in 42 of 368 patients; the others underwent one-sided thoracic sympathectomy followed by the other side after evaluating the results of the first.11 However, we believe it is unnecessary to place additional psychological stress on patients undergoing surgery for aesthetic reasons. Horner’s syndrome is a clinical entity consisting of miosis, ptosis, and anhidrosis, which occurs when the T1 ganglion (which constitutes the stellate ganglion) is damaged. It is an extremely annoying complication seen in 5% of cases after sympathectomy. In our series, we observed 2 cases of Horner’s syndrome which subsequently regressed. In these two cases, while performing en-bloc resection without electrocautery, hemorrhage from intercostal veins occurred. We believe that excessive use of electrocautery to control bleeding is the main cause of T1 involvement.
Conclusion
Thoracoscopic sympathectomy is an effective treatment and has high success rates in the treatment of hyperhidrosis. There is a need for clinical trials discussing long-term results for compensatory hyperhidrosis and the level of resections.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments.
Informed Consent
Informed consent was obtained from all participants.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the scientific content of the article, including the study design, data collection, analysis and interpretation, manuscript preparation, and approval of the final version of the manuscript.
References
-
Arnold SW, Daniel TM. Thoracoscopic sympathectomy. In: General thoracic surgery. 2006:698-707.
-
Dumont P, Denoyer A, Robin P. Long-term results of thoracoscopic sympathectomy for hyperhidrosis. Ann Thorac Surg. 2004;78:1801-1807. doi:10.1016/j.athoracsur.2004.03.012
-
Kopelman D, Hashmonai M. Upper thoracic sympathetic surgery: open surgical techniques. Clin Auton Res. 2003;13:10-15.
-
Miller DL, Force SD. Outpatient microthoracoscopic sympathectomy for palmar hyperhidrosis. Ann Thorac Surg. 2007;83:1850-1853. doi:10.1016/j.athoracsur.2006.11.030
-
Licht PB, Pilegaard HK. Severity of compensatory sweating after thoracoscopic sympathectomy. Ann Thorac Surg. 2004;78(2):427-431. doi:10.1016/j.athoracsur.2004.02.087
-
Reisfeld R, Nguyen R, Pnini A. Endoscopic thoracic sympathectomy for hyperhidrosis: experience with both cauterization and clamping methods. Surg Laparosc Endosc Percutan Tech. 2002;12(4):255-267. doi:10.1097/00129689-200208000-00011
-
Sugimura H, Spratt EH, Compeau CG, et al. Thoracoscopic sympathetic clipping for hyperhidrosis: long-term results and reversibility. J Thorac Cardiovasc Surg. 2009;137:1370-1376. doi:10.1016/j.jtcvs.2009.01.008
-
Liu Y, Yang J, Yang F, et al. Surgical treatment of primary hyperhidrozis: a prospective randomized study comparing T3 and T4 sympathicotomy. Eur J Cardiothorac Surg. 2009;35:398-402. doi:10.1016/j.ejcts.2008.10.048
-
O’Connor K, Molina F, Poirier P, Vaillancourt R. Cardiac arrest as a major complication of bilateral cervico-dorsal sympathectomy. Interact Cardiovasc Thorac Surg. 2009;8:238-239.
-
Drott C, Claes G, Gothberg G, Paszkowski P. Cardiac effects of endoscopic electrocautery of the upper thoracic sympathetic chain. Eur J Surg Suppl. 1994:65-70.
-
Görür R, Yıldızhan A, Türüt H, et al. El terlemesi nedeniyle uygulanan 530 sempatektomi ameliyatı ve uzun dönem sonuçların değerlendirilmesi. Turk Gogus Kalp Damar Cerrahisi Derg. 2009;17:28-32.
Tables
Table 1. The indications, level of resections and type of sympathectomy of the TS performed patients
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Sezai Çubuk, Orhan Yücel, Okan Karataş, Kuthan Kavaklı, Hasan Çaylak, Sedat Gürkök, Ersin Sapmaz, Hakan Işık, Alper Gözübüyük, Onur Genç. Analysis of 54 patients who underwent thoracoscopic sympathectomy. Eu Clin Anal Med 2013;1(1):1-3. doi:10.4328/ECAM.4
- Received:
- February 6, 2013
- Accepted:
- March 7, 2013
- Published Online:
- March 11, 2013
- Printed:
- March 11, 2013