Intrathoracic pleural lipomas
Intrathoracic pleural lipomas
Authors
Abstract
AimLipomas are benign tumors composed of adipose tissue. They are usually located in the subcutaneous region, particularly in the upper back, neck, and shoulder. However, they rarely seen in the intrathoracic cavity. The objective of this study is to analyze intrathoracic pleural lipomas.
Methods
We analyzed a retrospective review of the clinicopathological records of 8 patients who had undergone surgical resection for intrathoracic lipomas between 1990 and 2012. The clinical records of all patient was examined with regard to age, sex, body mass index, presenting symptoms, lesion locations and sizes, diagnostic methods, operative procedures,
histopathological features, and prognosis.
Results There were 5 men and 3 female with a mean age 60,1 (range, 29-75 years). Symptoms noticed were chest pain in three, dyspnea in one, neck swelling in one. Four patients had no symptoms, and lesions were found incidentally on chest radiography. Radiographically, the tumors showed well-defined, homogenous, and fatty density lesions. Tumor excision was carried out, 4 right sided and 4 left; video-assisted thoracoscopy in one case, thoracotomy in 7 cases. All lesions were intrathoracic lipomas sourced from parietal pleura. The size of the lesions ranged between 3-12cm, the average was 7.6 cm. Complete resection was achieved in all patients except one. There were no recurrences in postoperative follow-up of patients and mean follow-up was 7.4 years.
Conclusion Intrathoracic lipomas are rare benign lesions. Our series is the largest in the literature. Because lipomas cannot be differentiated from malignant lesions, and they have invasive growth capability, surgery should be performed for the purpose of diagnosis and treatment.
Keywords
Introduction
Lipomas are benign soft tissue tumors arising from mature adipocytes. Although they can be seen almost anywhere in the body, their occurrence in intrathoracic cavity in relation to the pleura is extremely rare.1
Intrathoracic lipomas can originated from the mediastinum, diaphragm, bronchus, lung, or thoracic wall. They are classified as deep-seated lipomas, in contrast to subcutaneous lipomas.2 They are most frequently observed benign tumor in adults. In 1781, Fothergill provided the first description of pleural lipoma.3
Since then, there have been very few data in the literature, mainly as case reports, with the largest series concerning six patients.4 Sakurai et al reported the largest series containing 10 patients with intrathoracic lipomas including endobronchial, mediastinal, and chest wall locations.2 In this study, we report the largest series in the literature which is eight pleural lipoma cases from a single center.
Materials and Methods
Thoracic surgery was performed on 19,236 patients in our clinic between 1990 to 2012. Postoperative pathological results were retrospectively analyzed and in 11 cases the diagnosis of pleural lipoma with intrathoracic extrapulmonary localization was detected.
Only 8 cases were included in the study, file details can not be reached in 3 cases. Endobronchial, intraparenchymal, chest wall located lesions were not included.
The clinical records of all patient was examined with regard to age, sex, body mass index (BMI), presenting symptom, lesion location and size, diagnostic investigation, operative procedures, histopathological features, and prognosis. BMI of more than 25 was considered overweight, more than 30 was considered obese.
Results
The clinical features of all patients are shown in Table 1. Mean age at presentation was 60.1 years. Four patients were asymptomatic and lesions were found incidentally on chest radiography. In past medical histories of the patients, one patient had previous cholecystectomy. Physical examination of a patient revealed minimal swelling on the left supraclavicular area with palpation. None of the patients were obese, and 5 cases were overweight. Laboratory findings were unremarkable in all patients.
Lesions in all patients were evaluated with chest X-ray and thorax computed tomography (CT). Chest X-ray revealed a well-defined, homogenous lesion shadow in 8 patients, in addition to this lesion pleural effusion was present in 1 patient. Thorax CT showed a well-circumscribed tumor with a homogenous fat density, it is compatible with subcutaneous fat between -50 and -150 Hounsfield unit (HU) (Figure 1-4).
The average size of the lesions was 7.6 cm. Increase in the size of the lesion was detected in 2 cases on the radiological follow-up in another center, so the patients was referred our clinic for surgical resection. On radiologically, there was a high suspicion of lipomatous lesion in all patients. In two cases, the radiological whole body scan was performed in another center, and no pathology has been detected. There was exudative pleural effusion in one patient (patient 6), cytological examination result of the fluid was chronic inflammation. Fiberoptic bronchoscopy was performed in all cases, there were no pathology. With the pre-diagnosis of lipomatous lesions, pre-operative pathological diagnosis would not change the treatment plan, so surgery was decided in all cases without a pathological diagnosis.
Surgical exploration showed lesions had smooth surface, some yellow, some white colored, encapsulated lesions except one, pedinculated or broad-based. In one case lesion was unencapsulated, showing intrathoracic extension to the neck area and had been invading subclavian artery (patient 1). Complete resection was not possible in this case and there was residual tumor (R2). In one case, while lesion which was located in supradiafragmatical area had been excised, partial resection of the diaphragm and diaphragmatic plication was performed.
Pleural biopsy and mass excision were performed in the patient with pleural effusion, histopathological examination showed chronic pleuritis. Complete resection was achieved in all patients except one. Postoperative histopathological examinations of the lesions were lipoma without malignant features in all patients.
There was no recurrence in postoperative follow-up of patients and mean follow-up duration was 7.4 years.
Discussion
Lipomas are benign soft tissue tumors derived from mature adipocytes.1 They may occur as a superficial (subcutaneous) or deep-seated.5 Deep-seated lipomas are rare in comparison, and they are often detected at relatively late stage of development and consequently tend to be larger than more superficial lipomas.5 Intrathoracic lipomas are very rare, and about 0.3% of all mediastinal tumors.6 Seen in all ages and both sexes equally, and often between the ages of 40-60.3,5 In our study, the incidence of pleural lipoma was 5.7 in 10,000 during 23 years period.
These slow growing neoplasms are mostly asymptomatic. Rarely they may attain a sufficient size to produce symptoms such as non-productive cough, thoracic tightness sensation, and dyspnea. An asymptomatic pleural lipoma may be incidentally discovered by a chest roentgenogram.1,7 Most lipomas are thought to be common in obese persons.5,7 In the present study, no patient was considered obese.
Thorax CT is very important method to demonstrate pleural origin, quantify and characterize these lesions. They demonstrate homogenous fat attenuation with values of -50 to -150HU.1,8 An invasive growth, inhomogeneous enhancement after intravenous contrast application should suggest the possibility of a malignant lesion.8 However, thorax CT can not accurately differentiate lipomas from well-differentiated liposarcoma.2,8 Magnetic resonance imaging is only useful if there is a doubt in CT scan diagnosis. It occasionally allows a more delicate evaluation of invasion of the lesion. Additionally, it has allowed us to rule out a diaphragmatic hernia and to confirm the strictly intrathoracic location of the pleural lipoma.3 Diaphragmatic lipoma is located predominantly on the left side (ratio 2 to 1) and posterolateral area of the diaphragm. Lobulations, localized eventration slip or hypertrophic diaphragmatic crus may simulate tumors of the diaphragm, and should be kept in mind during evaluation.9 In our study, in all cases radiological findings were consistent with lipoma like lesion.
Deep-seated lipomas are likely to be less well-defined than subcutaneous lipomas, and can occasionally exhibit an infiltration. Regarding the mode of tumor growth of intrathoracic lipomas, the tumors may not only lie entirely within the thoracic cavity but can also extend from the upper mediastinum in to the neck, or subpleural region through the subcutaneous tissue of the chest wall behavior.2,10 In our study, one patient showed infiltrating lipoma. In this case, the lesion had invaded subclavian artery. Preoperative radiological lesion was found extending to the apical region, but structural characteristics of the lesion was not considered malignant.
In case of diagnostic doubt at the scanner, or if there is a metastasis suggestive context, diagnosis can be confirmed by a fine needle aspiration. It has no other indication.3 Yet there were no malignancy histories in the cases, metastatic lesions was not considered. Preoperative biopsy was not performed due to there was not going to be any change in the surgical plan.
The treatment strategy of asymptomatic lipomas remains controversial.4 Some authors recommend radiological follow-up of asymptomatic intrathoracic lipomas,4 and others recommend surgical excision.2,3,9 In our opinion, reasons of surgical exploration are both diagnosis and treatment; when the lesion reaches a large size, it makes organ compression; patients, remain followed-up for a long time, feel stress, and the possibility of malignancy can not be ruled out. In addition, it can be difficult to differentiate lipomas from liposarcomas preoperatively, especially well-differentiated liposarcomas. Some of well-differentiated liposarcomas may transform to dedifferentiated liposarcoma over time.11 As a result, in the light of all of these informations even in the suspicion of lipoma by radiology, surgery is recommended for diagnosis and treatment.
Patients with advanced ages and poor conditions should be followed up. If the case is young and the lesion is small we leave the choice of surgery or follow up to the patient, also it is stated that when they get older risks of comorbid diseases and advanced age would make problem so we also recommend surgery. Current recommendations include complete en-bloc removal of these tumors whenever possible, as this is the only definitive treatment option.12 If pedinculated lipoma is not infiltrating other tissues, the video-assisted thoracoscopic surgery (VATS) is recommended.1,2 We prefer thoracotomy with bigger and broad based lesions.
In histopathological examination, lipomas consist of mostly uniform, mature adipose cells with no mitotic activity.5,11 In our study, all cases were benign lipomas without mitosis.
Lipomas are benign and postoperative outcome well. They may recur locally and following surgical excision the recurrence rate is less than 5% for all lipomatous tumors.5 Deep-seated lipomas have a greater tendency to recur due to the difficulty of complete surgical removal.5 Residual tumor should be followed up. The follow-up should continue if lesion is stable radiologically. Although there has been only one R2 resection case in this study, no recurrence was noted during follow-up of all cases.
Conclusion
Intrathoracic lipomas are rare benign lesions. Our series is the largest in the literature. Because lipomas cannot be differentiated from malignant lesions, and they have invasive growth capability, surgery should be performed for the purpose of diagnosis and treatment.
Declarations
Animal and Human Rights Statement
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was waived due to the retrospective nature of the study.
Conflict of Interest
The authors declare that they have no conflict of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the scientific content of the article, including the study design, data collection, analysis and interpretation, manuscript preparation, and approval of the final version of the manuscript.
References
-
Prasad S, Ramachandra L, Agarwal S, Sharma D. Successful management of pleural lipoma by video-assisted thoracoscopic surgery. J Minim Access Surg. 2012;8:19-20. doi:10.4103/0972-9941.91776
-
Sakurai H, Kaji M, Yamazaki K, Suemasu K. Intrathoracic lipomas: their clinicopathological behaviors are not as straightforward as expected. Ann Thorac Surg. 2008;86:261-265. doi:10.1016/j.athoracsur.2008.03.052
-
Jayle C, Hajj-Chahine J, Allain G, Milin S, Soubiron L, Corbi P. Pleural lipoma: a non-surgical lesion? Interact Cardiovasc Thorac Surg. 2012;14:735-738. doi:10.1093/icvts/ivs052
-
Epler GR, McLoud TC, Munn CS, Colby TV. Pleural lipoma: diagnosis by computed tomography. Chest. 1986;90:265-268. doi:10.1378/chest.90.2.265
-
Weiss SW, Goldblum JR. Benign lipomatous tumors and liposarcoma. In: Weiss SW, Goldblum JR, eds. Enzinger and Weiss’s Soft Tissue Tumors. 4th ed. Mosby; 2001:571-693.
-
Karapolat S, Dost B, Kılıçgün A. An unusual intrathoracic mass: lipoma. J Clin Anal Med.
-
Kara M, Kavukçu Ş, Tunçözgür B, Dikmen E, Erekul S. İntratorasik subplevral lipom olgusu. Ankara Üniv Tıp Fak Mecmuası. 1996;49:173-175.
-
Karlo AC, Stolzmann P, Frauenfelder T, Donati OF, Leschka S. Computed tomography imaging of subpleural lipoma in two men: two case reports. J Med Case Rep. 2010;4:380-381. doi:10.1186/1752-1947-4-380
-
Şen S, Dişçigil B, Badak İ, Gürcün U. Lipoma of the diaphragm: a rare presentation. Ann Thorac Surg. 2007;83:2203-2205. doi:10.1016/j.athoracsur.2007.01.040
-
Fletcher CDM, Unni KK, Mertens F. World Health Organization Classification of Tumours: Pathology and Genetics of Tumours of Soft Tissue and Bone. IARC Press; 2002.
-
Bicakcioglu P, Sak SD, Tastepe AI. Liposarcoma of the chest wall: transformation of dedifferentiated liposarcoma from the recurrent lipoma. Saudi Med J. 2012;33:901-903. doi:10.15537/1658-3175.5606
-
Hagmaier RM, Nelson GA, Daniels LJ, Riker AI. Successful removal of a giant intrathoracic lipoma: a case report and review of the literature. Cases J. 2008;1:87. doi:10.1186/1757-1626-1-87
Figures
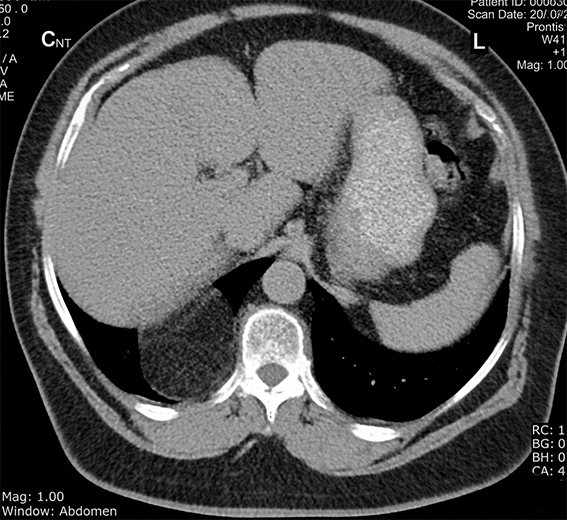
Figure 1. Thorax CT showing supradiaphragmatic lesion in the right hemithorax.
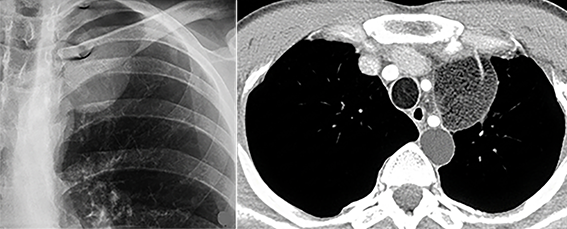
Figure 2. Chest radiography showing a homogenous lesion with smooth borders in the left upper zone (A), Thorax CT appearance of the lesion (B).

Figure 3. Thorax CT reveals broad–based lesion filling most of the left hemithorax.

Figure 4. Thorax CT in lung window showing intrathoracic lesion.
Tables
Table 1. Clinical features of patients with intrathoracic lipoma

Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Pınar Bıçakçıoğlu, Erkmen Gülhan, Ebru Sayılır, Leyla Acar, Funda Demirağ, Şeref Özkara, Sadi Kaya. Intrathoracic pleural lipomas. Eu Clin Anal Med 2013;1(1):10-13. doi:10.4328/ECAM.6
- Received:
- March 17, 2013
- Accepted:
- April 3, 2013
- Published Online:
- April 4, 2013
- Printed:
- April 4, 2013