Diagnostic performance of point of care ultrasonography for acute epiploic appendagitis in the emergency department
Point of care ultrasonography for acute epiploic appendagitis
Authors
Abstract
AimPrimary epiploic appendagitis (EA) is an uncommon cause of abdominal pain and is often overlooked in the Emergency Department (ED). Computed tomography (CT) is the gold standard imaging method in diagnosis. However, CT can cause adverse effects due to high ionizing radiation exposure. This study aimed to determine the sensitivity and specificity of Point of Care Ultrasonography (PoCUS) in the diagnosis of EA to overcome the exposure to ionizing radiation of these cases in unnecessary CT examinations.
MethodsPatients who presented at ED with peritoneal pain localized in the lower quadrant were grouped according to the PoCUS examination results as EA-positive and EA-negative. Accepting the abdominal CT findings of these cases as the gold standard, the sensitivity and specificity of PoCUS were statistically analyzed with respect to EA diagnosis.
ResultsForty-six patients were assessed. The 13 patients diagnosed with EA comprised 11 (84.6%) males and 2 (15.4%) females with a mean age of 38.07±13.11 years. The mean WBC value was significantly higher in the patients diagnosed with EA than in those not diagnosed (p=0.003). No significant difference was determined between the groups with respect to neutrophil % and CRP values (p=0.496, p=0.127, respectively). In the diagnosis of EA, PoCUS was found to have 92.3% sensitivity, 100% specificity, PPV 100%, and NPV 97.1%.
Conclusion With high sensitivity and specificity rates, PoCUS can be safely used in the diagnostic process of EA cases in ED.
Keywords
Introduction
Primary Epiploic Appendagitis (EA) is an uncommon inflammatory pathology due to the colonic epiploic appendix revolving around itself, subsequent ischemia, drainage vein obstruction, and hemorrhagic infarct.1 In patients presenting to the Emergency Department (ED) with acute or subacute lower quadrant abdominal pain, primary EA; NOT PEA is generally diagnosed incidentally with diagnostic imaging methods.2,3 The clinical presentation of EA, usually in the right lower quadrant, resembles acute appendicitis (AA), and acute diverticulitis (AD) if on the left side, because of the location characteristics. Therefore, the pre or first diagnosis of almost all EA cases with peritoneal pain that can typically be extremely well localized is known to be incorrect.4 In the management of patients with painful acute abdomen, computed tomography (CT) is accepted as extremely sensitive in the characterization of abdominal surgical pathologies but can cause adverse effects due to high ionizing radiation exposure and intravenous injection of contrast material. While CT reveals the diagnostic findings for EA, which is currently treated conservatively, it is also effective in discounting other intra-abdominal pathologies.5 However, due to insufficient awareness and the probable reporting of EA cases at much lower rates than there are in reality, up to 64% are overlooked, including in CT reports.5 Nevertheless, it has been reported by centers experienced in gastrointestinal imaging that ultrasonography (US) could be a reserve diagnostic method before CT examination or in the presence of CT findings that are suspicious in respect of EA.6
The aim of this study was to determine the sensitivity and specificity of Point of Care Ultrasonography (PoCUS), which is currently becoming more widespread in different areas of use, in the diagnosis of acute EA, to be able to overcome unnecessary CT examinations when managing these cases, the majority of which are overlooked in ED, and to raise awareness of the necessity to include EA in the differential diagnosis of patients with painful acute abdomen.
Materials and Methods
The study included patients aged >18 years who presented at ED with complaints of isolated, unilateral lower quadrant pain, which could be well localized by finger indication, and who provided informed consent for participation in the study. The presence of additional diseases such as coronary artery disease (CAD), hypertension (HT), and Diabetes Mellitus (DM) was recorded as comorbid status. Patients were excluded from the study if they had a history of abdominal surgery, described nonlocalised abdominal pain, or had additional or typical symptoms of other acute abdomen causes. For the patients included in the study, a biochemistry panel including at least C-reactive protein (CRP) and laboratory tests from the complete blood count were included in the patient management algorithm routinely followed in ED practice for patients presenting with abdominal pain.
The cases were then grouped according to the PoCUS examination findings as EA-positive or EA-negative. The basic study group comprised the PoCUS-positive cases and those who were PoCUS-negative but had indications for abdominal CT to discount AA or AD following clinical evaluation. Accepting the abdominal CT findings of these cases as the gold standard, the sensitivity and specificity of PoCUS were statistically analyzed with respect to EA diagnosis.
The PoCUS examination was performed by an emergency medicine specialist who has a PoCUS usage certificate in the emergency department, has 15 years of emergency service experience, and has been actively applying PoCUS for 10 years. The PoCUS examination was performed by the same emergency medicine specialist for all patients included in the study and it was performed using an Affiniti 70 US device (Philips Healthcare, Amsterdam, Netherlands) with L12-3 and L18-5 high-frequency linear probes. The examinations were made with the patient in the supine position. The patients were evaluated at the target points where they felt the most pain or sensitivity. In the PoCUS examination, the presence of a hyperechoic lesion, adjacent to the course of the colon, adhering to the abdominal wall, and not compressed, was accepted as EA-positive (Figure 1; a, b, c). Abdominal CT images were acquired using a 128-slice, Optima CT660 CT device (General Electric Medical Systems, Milwaukee, WI, USA). The injection protocol consisted of 100 ml non-ionic iodinated contrast agents (iohexol, Opaxol Intravenous/Intraarterial/intrathecal 300 mg of iodine per milliliter; Türkiye). The abdominal CT images were evaluated by radiologists in our hospital. The presence on CT of an oval-shaped, lipid-density lesion showing surrounding striations, adjacent to the colon, with a central hypodense and peripheral rim hyperdense appearance was accepted as diagnostic with respect to EA (Figure 1; d, e, f).
Ethical ApprovalThe study was approved by the Ethics Committee of Hitit University (Date: 28.02.2023, Decision No: 2023-01).
Statistical AnalysisThe data obtained were analyzed statistically using SPSS version 22.0 software (SPSS Inc., Chicago, IL, USA). Conformity of the data to normal distribution was assessed with the Shapiro-Wilk test. Descriptive statistics were presented as mean ± standard deviation values for normally distributed numerical data and as median (min-max) values for non-normally distributed numerical data. Descriptive statistics of categorical variables were presented as number (n) and percentage (%). Ratio comparisons between two independent groups were performed with either the Chi-square test or Fisher’s Exact test, depending on the sample sizes in the crosstab cells. The assumption of homogeneity of variances was tested with the Levene test. Comparisons of numerical data between two independent groups were performed with the Student’s t-test for normally distributed data and the Mann-Whitney U-test for data not showing normal distribution. Sensitivity, specificity, accuracy, positive predictive value (PPV), and negative predictive value (NPV) values were used to evaluate the success of the PoCUS in predicting CT diagnoses. The level of statistical significance was accepted as p<0.05.
Reporting GuidelinesThe study was reported in accordance with STROBE guidelines.
Results
Statistical analysis was carried out of the data of 46 patients, comprising 23 (50%) males and 23 (50%) females with a mean age of 46.8 ± 17.99 years (range, 21-87 years). Comorbidities were recorded as CAD in 4 (8.7%) patients, HT in 1 (2.2%), DM in 1 (2.2%) and no comorbidity was present in 40 (87%). The WBC value was determined as 8.06±2.05 (min-max: 4.19 – 13.1), neutrophil % as 61.42±9.09 (min-max: 38.8 – 77.1), and CRP value as 7.87±6.65 (min-max: 3.13 – 42.7).
According to the PoCUS results, the patients were grouped as 13 EA-positive and 33 EA-negative. No alternative diagnosis was detected in the EA-negative group. According to the CT results, which were accepted as the gold standard to determine the success of diagnosing EA, the sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of PoCUS are shown in Table 1.
Of the 13 patients diagnosed with EA on CT, 12 were PoCUS-positive and 1 was negative (sensitivity: 92.3%, 95% CI: 62% – 99.5%) (Figure 2).
Of the 33 patients not diagnosed with EA on CT, all were PoCUS-negative (specificity:100%, 95% CI: 87% – 100%). In the diagnosis of EA, PoCUS was found to have a PPV of 100% (69.8 – 100) and NPV of 97.1% (82.9 – 99.8).
The statistical comparisons of the sociodemographic and clinical characteristics of the patients diagnosed or not with EA according to the CT findings are shown in Table 2.
The patients diagnosed with EA comprised 2 (15.4%) females and 11 (84.6%) males, and the patients not diagnosed with EA comprised 21 (63.6%) females and 12 (36.4%) males. The difference in gender distribution between the groups was statistically significant (p=0.003). The mean age was determined to be 38.07±13.11 years in the patients diagnosed with EA and was statistically significantly higher than 50.24±18.64 years in the patients not diagnosed with EA (p=0.037). The distribution of the rates of comorbidities was similar in both groups (p=0.075, p=0.526, respectively).
The mean WBC value was statistically significantly higher in the patients diagnosed with EA than in those where EA was discounted (p=0.03) (Table 2). No significant difference was determined between the groups with respect to neutrophil % and CRP values (p=0.496, p=0.127, respectively).
Discussion
EA is an uncommon cause of acute abdomen, constituting 1.1-1.3% of patients who present at ED with abdominal pain.7 EA cases are often overlooked and are usually confused with the frequently seen causes of acute abdomen.8 Although EA was accepted as a condition that required surgery in the past, it is now seen as a pathology that can be treated conservatively.9 In addition to the absence of pathognomonic clinical findings, because of the insufficient level of awareness of clinicians about EA, diagnosis is extremely difficult other than with imaging methods.8
The current widespread use of CT, especially in emergency diagnosis centers, and the elimination to a great extent of hesitation at the stage of differential diagnosis of patients presenting at ED with complaints of abdominal pain has led to the more frequent diagnosis of EA cases.10 This means that over time, the frequency of PEA will increase compared to the rates reported in the literature.11 It will also mean that EA cases will be identified more often in ED and avoid unnecessary surgery or diagnostic procedures. However, because of the exposure to ionizing radiation from CT and the negative effects of intravenous contrast material used in the CT protocols, which is used to determine the causes of acute abdomen, non-invasive diagnostic methods should be prioritized in these cases, which are candidates for conservative treatment. The ultrasonographic findings of EA have been defined in the literature and thus the use of US has been recommended for EA diagnosis in conditions where CT is contra-indicated, such as pregnancy.12
PoCUS has become extremely widespread and now occupies an important place in emergency medicine practice.13 Although CT is still the first preferred imaging method in the USA for patients with abdominal pain, more clinicians are starting to use PoCUS, which is continuously developing.14 There are studies in the literature that have researched the value of PoCUS in AD diagnosis, which is the pathology most often confused with EA, but there is no study that has examined the diagnostic success of PoCUS for EA.15
It has been reported in the literature that acute EA is seen 4-fold more in males than in females and it has been determined to be weighted in the 20-50 years age range.16 In the current study, 84.6% of the patients diagnosed with EA were male and the mean age was 38.07±13.11 years, which was consistent with the literature.
Although it has been reported that symptoms such as fever, nausea, vomiting, and diarrhea, albeit rare, could be associated with EA, these symptoms were not present in the current study of patients with a pre-diagnosis of EA.12 In a retrospective study of 30 patients with acute EA, it was reported that in the clinical evaluation, all the patients had sensitivity localized in the abdomen and the pain was in the right lower quadrant (41.9%) or the left lower quadrant (41.9%).11 In all the patients included in the current study, as has been reported in many studies, other than sensitivity on palpation in a specific localization described with the patient’s finger, which did not move and had acute onset, there were no other findings in the physical examination.17
EA can emerge at any level along the course of the colon but is most often seen in the sigmoid (50%) and the descending colon (26%).4 The frequency of EA seen in the ascending colon and the cecum has been reported to be 22%, and at the rate of 2% in the transverse colon.18 All the patients in the current study had sensitivity localized in the left lower quadrant. consistent with the findings in the literature.
The abnormality is not generally determined in the laboratory findings of acute EA cases.12 It has been reported that there could be a slight increase in WBC and CRP associated with the inflammatory response developing secondary to ischaemic fat necrosis in a small proportion of patients.19,20 There are also studies stating that this inflammatory response can manifest in cases with mild leukocytosis only.4,21 In the cases diagnosed with EA in the current study, the WBC value was determined to be significantly higher than that of the cases not diagnosed with EA. For the CRP level and other laboratory markers, there was no significant variability between the groups. This was consistent with the non-specific laboratory variability indicated in the literature for EA.
No study could be found in the literature that has examined the success of PoCUS in the diagnosis of EA. However, there are studies of PoCUS diagnosis of AA and AD, which are the most common causes of pain in both lower quadrants.15,22 In a meta-analysis examining the diagnostic performance of PoCUS in AA cases, sensitivity and specificity for AA in adults were reported to be 84% and 91%, respectively.22 Even in children, sensitivity and specificity were reported to reach 95%.22 In another study, sensitivity was reported as 92.3% and specificity as 95.8%.23 Another study that investigated the efficacy of PoCUS in AD diagnosis determined these rates as 92.7%, 90.9%, 92.7%, and 90.9%, respectively.24 In the current study, the sensitivity, specificity, PPV, and NPV values of PoCUS in the diagnosis of EA were determined to be 92.3%, 100%, 100%, and 97.1%, respectively. These values were similar and higher than the rates reported in the literature for the diagnostic success of PoCUS in the diagnosis of AA and AD. This demonstrates that PoCUS can be safely used in ED for the diagnosis of EA. The diagnostic efficacy values reported in the literature for PoCUS in the diagnosis of AA and AD have also been evaluated as PEA not being a diagnosis of exclusion. In other words, it is thought that unnecessary CT imaging to discount AA and AD in the differential diagnosis will be reduced in cases evaluated as EA-negative on PoCUS, and the diagnostic process will be able to be completed with first look PoCUS.
Limitations
As this was a pilot study, the patients were selected from patients who presented at ED with isolated symptoms which could be typical of EA. All the cases presented with complaints in the left lower quadrant. Therefore, further studies with larger patient groups of cases with different clinical presentations additional symptoms, and different intra-abdominal pathologies, which should be included in the differential diagnosis will be able to contribute to the most reliable use of PoCUS.
Conclusion
PoCUS can be safely used in ED in the diagnostic process of EA cases as it has high sensitivity and specificity rates. Thus, in addition to protecting EA cases, who are candidates for conservative treatment, from ionizing radiation exposure in unnecessary CT examinations, a significant reduction will be able to be obtained in the time spent in ED. Nevertheless, for more widespread use of the method and to be able to use it in more complex presentations there is a need for further studies with larger varied cohorts.
Declarations
Ethics Declarations
The authors declare that all procedures performed in this study were conducted in accordance with institutional, national, and international ethical standards.
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Written informed consent was obtained from all participants.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
None of the authors received any type of financial support that could be considered potential conflict of interest regarding the manuscript or its submission.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content including study design, data collection, analysis and interpretation, writing, some of the main line, or all of the preparation and scientific review of the contents and approval of the final version of the article.
Abbreviations
AA: Acute appendicitis
AD: Acute diverticulitis
CAD: Coronary artery disease
CRP: C-reactive protein
CT: Computed tomography
DM: Diabetes mellitus
EA: Epiploic appendagitis
ED: Emergency department
HT: Hypertension
NPV: Negative predictive value
PEA: Primary epiploic appendagitis
PoCUS: Point-of-care ultrasonography
PPV: Positive predictive value
US: Ultrasonography
WBC: White blood cell
References
-
Almeida RR, Singh AK, Mansouri M, Spilberg G, Alkasab T, Lev MH. Impact of radiology report wording on care of patients with acute epiploic appendagitis. AJR Am J Roentgenol. 2019;212(6):1265-1270. doi:10.2214/ajr.18.20747
-
Eberhardt SC, Strickland CD, Epstein KN. Radiology of epiploic appendages: acute appendagitis, post-infarcted appendages, and imaging natural history. Abdom Radiol (NY). 2016;41(8):1653-1665. doi:10.1007/s00261-016-0757-0
-
Hwang JA, Kim SM, Song HJ, et al. Differential diagnosis of left-sided abdominal pain: primary epiploic appendagitis vs colonic diverticulitis. World J Gastroenterol. 2013;19(40):6842-6848. doi:10.3748/wjg.v19.i40.6842
-
Chen JH, Wu CC, Wu PH. Epiploic appendagitis: an uncommon and easily misdiagnosed disease. J Dig Dis. 2011;12(6):448-452. doi:10.1111/j.1751-2980.2011.00543.x
-
Zadeh ES, Kindermann J, Dietrich CF, et al. Clinical awareness and acceptance of sonographically diagnosed epiploic appendagitis: a retrospective analysis of EA in a single tertiary academic referral center. Ultrasound Int Open. 2020;6(3):E87-E93.
-
Dietrich CF, Hollerweger A, Dirks K, et al. EFSUMB gastrointestinal ultrasound task force group: celiac sprue and other rare gastrointestinal diseases ultrasound features. Med Ultrason. 2019;21(3):299-315. doi:10.11152/mu-2162
-
Kefala MA, Tepelenis K, Stefanou CK, et al. Primary epiploic appendagitis mimicking acute appendicitis: a case report and narrative review of the literature. Korean J Gastroenterol. 2020;76(2):88-93. doi:10.4166/kjg.2020.76.2.88
-
Giannis D, Matenoglou E, Sidiropoulou MS, et al. Epiploic appendagitis: pathogenesis, clinical findings and imaging clues of a misdiagnosed mimicker. Ann Transl Med. 2019;7(24):814. doi:10.21037/atm.2019.12.74
-
Schnedl WJ, Krause R, Tafeit E, Tillich M, Lipp RW, Wallner-Liebmann SJ. Insights into epiploic appendagitis. Nat Rev Gastroenterol Hepatol. 2011;8(1):45-49. doi:10.1038/nrgastro.2010.189
-
Singh AK, Gervais DA, Hahn PF, Sagar P, Mueller PR, Novelline RA. Acute epiploic appendagitis and its mimics. Radiographics. 2005;25(6):1521-1534. doi:10.1148/rg.256055030
-
Choi YU, Choi PW, Park YH, et al. Clinical characteristics of primary epiploic appendagitis. J Korean Soc Coloproctol. 2011;27(3):114-121. doi:10.3393/jksc.2011.27.3.114
-
Nadida D, Amal A, Ines M, et al. Acute epiploic appendagitis: radiologic and clinical features of 12 patients. Int J Surg Case Rep. 2016;28:219-222. doi:10.1016/j.ijscr.2016.09.015
-
Liao SF, Chen PJ, Chaou CH, Lee CH. Top-cited publications on point-of-care ultrasound: the evolution of research trends. Am J Emerg Med. 2018;36(8):1429-1438. doi:10.1016/j.ajem.2018.01.002
-
Rodgers PM, Verma R. Transabdominal ultrasound for bowel evaluation. Radiol Clin North Am. 2013;51(1):133-148. doi:10.1016/j.rcl.2012.09.008
-
Shokoohi H, Nasser S, Pyle M, Earls JP, Liteplo A, Boniface K. Utility of point-of-care ultrasound in patients with suspected diverticulitis in the emergency department. J Clin Ultrasound. 2020;48(6):337-342. doi:10.1002/jcu.22857
-
Trovato P, Simonetti I, Verde F, et al. Acute epiploic appendagitis: ultrasound and computed tomography findings of a rare case of acute abdominal pain and the role of other imaging techniques. Pol J Radiol. 2020;85:e178-e182. doi:10.5114/pjr.2020.94335
-
Ortega-Cruz HD, Martínez-Souss J, Acosta-Pumarejo E, Toro DH. Epiploic appendagitis, an uncommon cause of abdominal pain: a case series and review of the literature. P R Health Sci J. 2015;34(4):219-221.
-
Singh AK, Gervais DA, Hahn PF, Rhea J, Mueller PR. CT appearance of acute appendagitis. AJR Am J Roentgenol. 2004;183(5):1303-1307. doi:10.2214/ajr.183.5.1831303
-
Akinosoglou K, Kraniotis P, Thomopoulos K, Assimakopoulos SF. Epiploic appendagitis: a non-surgical cause of acute abdomen. Ann Gastroenterol. 2015;28(2):296-298.
-
Gourgiotis S, Oikonomou C, Veloudis G, Lardou I, Pittaras G, Villias C. The diagnostic dilemma of primary epiploic appendagitis and how to establish a diagnosis. Oman Med J. 2016;31(3):235-237. doi:10.5001/omj.2016.45
-
Ozdemir S, Gulpinar K, Leventoglu S, et al. Torsion of the primary epiploic appendagitis: a case series and review of the literature. Am J Surg. 2010;199(4):453-458. doi:10.1016/j.amjsurg.2009.02.004
-
Lee SH, Yun SJ. Diagnostic performance of emergency physician-performed point-of-care ultrasonography for acute appendicitis: a meta-analysis. Am J Emerg Med. 2019;37(4):696-705. doi:10.1016/j.ajem.2018.07.025
-
Gungor F, Kilic T, Akyol KC, et al. Diagnostic value and effect of bedside ultrasound in acute appendicitis in the emergency department. Acad Emerg Med. 2017;24(5):578-586. doi:10.1111/acem.13169
-
Nazerian P, Gigli C, Donnarumma E, et al. Diagnostic accuracy of point-of-care ultrasound integrated into clinical examination for acute diverticulitis: a prospective multicenter study. Ultraschall Med. 2021;42(6):614-622. doi:10.1055/a-1161-0780
Figures
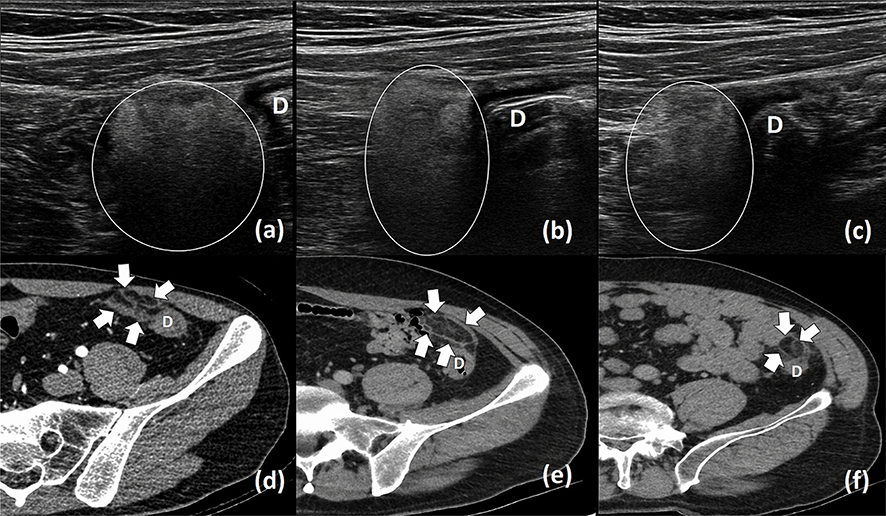
Figure 1. US samples from cases considered PoCUS positive for EA (a, b, c). Echoic nodular lesions consistent with EA are shown in the ring in PoCUS images. Abdominal CT sections of the same cases (d, e, f). Typical lesions for EA are indicated by arrows. (D: Descendant colon)
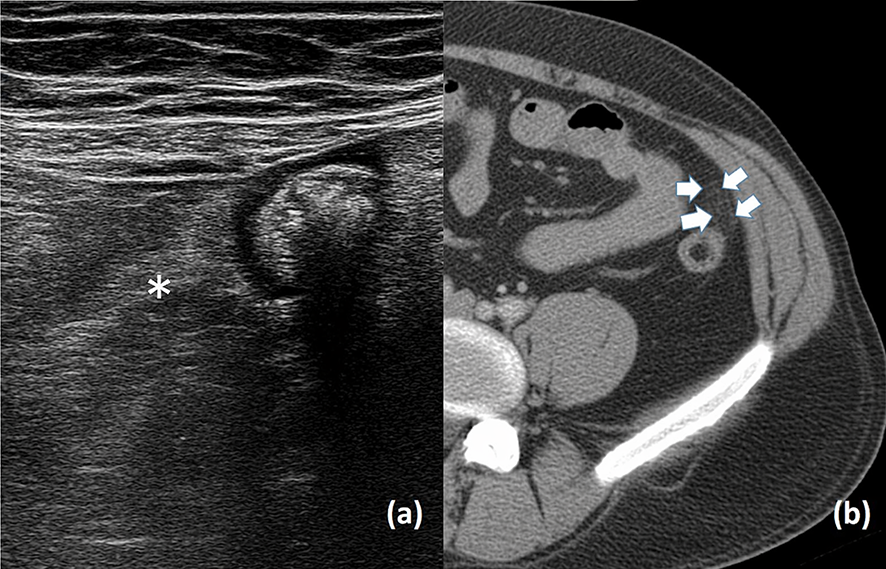
Figure 2. US (a) and CT (b) images of the only case with a false negative diagnosis with PoCUS. a; Typical echogenic nodule could not be demarcated in PoCUS (asteriks). b; EA lesion barely distinguishable on CT (arrows). (D: Descendant colon)
Tables
Table 1. Success of PoCUS in the diagnosis of Acute Epiploic Appendagitis

PoCUS: Point of care ultrasonography CT: Computed tomography PPV: Positive Predictive Value NPV: Negative Predictive Value
Table 2. Statistical findings regarding the comparison of socio-demographic and clinical characteristics of patients between research groups
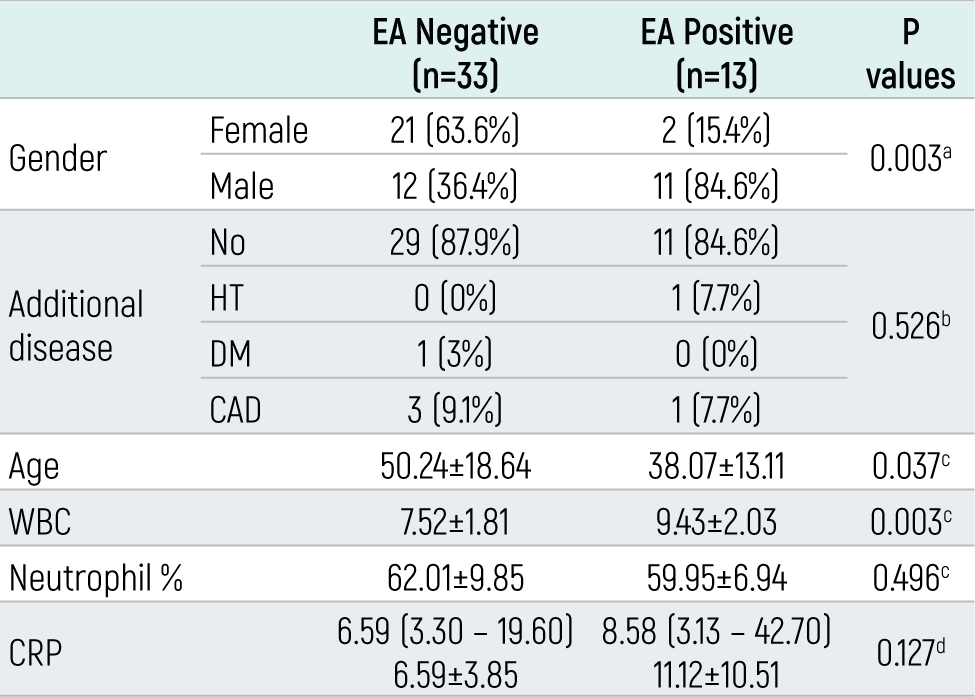
aChi-square test bFisher exact test cStudent’s t-test with mean±standard deviation dMann-Whitney U test with median (min-max) and mean ± standard deviation WBC: white blood cell, CRP: C-reactive protein, CAD: coronary artery disease, DM: diabetes mellitus, HT: hypertension
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Seval Komut. Diagnostic performance of point of care ultrasonography for acute epiploic appendagitis in the emergency department. Eu Clin Anal Med 2023;11(Suppl 1):S9-13. doi:10.4328/ECAM.10060
- Received:
- August 29, 2023
- Accepted:
- October 12, 2023
- Published Online:
- October 14, 2023
- Printed:
- October 15, 2023