Protection from renal injury with popliteal artery micro-puncture andminimized radiographic contrast use with critical SFA lesions, low EGFR, and high creatinine levels
Ipsilateral popliteal artery micro-puncture
Authors
Abstract
AimIn recent years endovascular treatment of symptomatic peripheral arterial disease (PAD) provides many advantages like fast application, fast recovery and low cost in many cases. And it is recommended as a primary revascularization strategy in a wide range of many PAD patients rather than surgical treatment of symptomatic peripheral arterial disease (PAD). However optimal methods of catheter-based treatment for renal insufiency patients remain controversial.
MethodsIn Yeditepe University Faculty of Medicine Hospital between 2017-2018, we performed endovascular treatment with ipsilateral popliteal artery puncture of 18 patients. Pre-op creatinin , EGFR and post-operative creatinin levels and puncture area complications were compared.
ResultsPrimary end-point was technical success with popliteal access without any post-operative complications and low dosage contrast usage. Secondary end-point was 3 months follow-up stenosis degree. No punction area complications were notted. None of patients had any hematoma, ecchymosis or pseudoaneurisyms in puncture area. And after procedure none of patients had to have dialisysis treatment despite high level of kreatinin and low EGFR values. In third month control follow-up patients were asymptomatic and no recurren vascular disease was seen in doppler usg.
ConclusionAs a conclusion, balloon angioplasty performed with ipsilateral popliteal artery micro-puncture with manually low dosage opaque use, allows the shortest way to access the target lesion and it protects the kidney from opaque toxication with minimizing the amount of opaque usage for superficial femoral artery lesions. Therefore, renal protection was ensured before and after the operation without dialysis in diabetic patients with low EGFR and borderline high creatinine levels in the study group. Furthermore, the incidence of complications is lower with popliteal artery micro-puncture than femoral artery puncture.
Keywords
Introduction
With endovascular techniques becoming more common in recent years, its use is gradually increasing thanks to its faster and low-cost outcomes although its long-term outcomes compared to peripheral artery surgery are controversial. Similarly, indications for endovascular therapy (EVT) for peripheral vascular disease (PVD) in current clinical approach are expanding to include elderly patients presenting with PVD who often have coexisting renal, cardiac, diabetic, and other comorbidities.1,2 The number of patients with low EGFR and borderline high creatinine levels accompanied by basal diabetes mellitus but who have not received dialysis yet are also increasing day by day at significant levels. In these patients, iodinated contrast may enhance the risk of contrast-induced nephropathy (CIN). CIN is an acute renal injury and may lead to irreversible loss of renal function.3,4 Renal insufficiency is one of the biggest problems for contrast used endovascular therapies. The main reasons for excessive use of radiological contrast agents are the distance between the target lesion and the puncture site and the prolonged operation time due to lesion complexity. Morbidity and mortality increase depending on the use of opaque agents.5 In this case, one must consider the amount of opaque agents when it comes to the contrast agent. Comorbidities such as concurrent Diabetes mellitus and renal failure are frequently seen in the majority of the PAD population.6,7 Another consideration for renal failure patients is the coagulopathy due to chronical renal failure (CRF). Pseudoaneurysm, hematoma, ecchymosis, infections, and thus surgical interventions are frequently observed, particularly in the femoral puncture site after the operation due to coagulopathy.8,9 Disorders in platelet functions in CRF patients increase the tendency to bleed. The reduction in the expression of glycoprotein Ib and glycoprotein Iib/IIIa in platelets and inhibition of the binding of fibrinogens to glycoprotein IIb/IIIa receptors by uremic toxins cause disruptions in the adhesion and aggregation of platelets. In addition, one can claim that preventing blood loss after peripheral vascular access is quite challenging given the common use of aspirin and clopidogrel in cardiovascular patients.10,11 Most of the time, these patients may experience post-operative complications such as pseudoaneurysm and hematoma and may even require surgical interventions.12 Here, we present the results of our retrospective study with popliteal artery micro-puncture for sited near the target lesion above-the-knee (ATK) arterial disease to use low dose contrast media to escape from CIN. And also this popliteal micro puncture provides more secure puncture site area to avoid bleeding complications conducted to evaluate the technical success and combined with drug coated balloon (Extender, Invamed, Ankara, Turkey) above-the-knee (ATK) arterial disease.
Materials and Methods
Ethical approval was obtained from Yeditepe University Clinical Trials Ethical Committee (No:967, 13/02/2019). Informed consent information was taken from all patients. We assigned 18 diabetic patients (15 were insulin depended, 3 were Oral Anti Diabetic usage) who had severe claudication or chronic limb ischemia due to critical stenosis or occlusion of the superficial femoral artery and additional chronic renal disease (CRD) without any dialysis treatment. Restenosis and clinical outcomes were assessed at 3 months. Invasive vascular radiology lab. of 18 patients who had DM and CRD with mean creatinin levels of 1.42. All patients were diabetic and CRD without dialysis treatment at Yeditepe University Faculty of Medicine Hospital between 2017-2018 with a popliteal puncture retrograde technique (12 males, 6 females; mean age: 64). PAD assessed as Rutherford class 2 to 5. The mean (±SD) length of the treated segment was 114±32 mm. Treated diseased femoro-popliteal arterial segments with diameter of 2.4-mm. Mean pre-op creatinin levels were 1.42(1.31-1.93) (Table 1). The operation started in the peripheral vascular interventional lab. after sterile staining and covering of the patient in reverse position. Popliteal artery puncture was performed with micro-puncture under Doppler USG. Then, 4F or 5French sheaths were introduced via the introducer. Opaque agent was manually given to the patients. All patients had stenoses of 70% to 100% from SFA to the Hunter’s channel (Figure 1). After the guidewire passed through the target lesion, the guidewire was advanced to the aorta level using NaviCross and Wiggman 0.14 MM Needle Catheters. Medicated balloon dilation was applied; each balloon was inflated at 10 to 12 atm for at least two minutes. After dilation of the entire target segment, biplane angiograms were obtained. Self-expanding nitinol stents (Dynalink or Absolute, Guidant) with a nominal diameter of 6mm were used in 4 of treatment patients. Biplane angiography was performed after the intervention in both groups, with the use of the same angles and magnifications used in the baseline angiograms. 100% patency was seen in DSA (Figure 2-5). In cases with a suboptimal primary result, which was defined as a residual stenosis of more than 30 percent or the presence of a flow-limiting dissection in the worst angiographic view, a second prolonged (more than two minutes) balloon dilation of the target segment was performed. In patients with a persistently suboptimal result after the second balloon dilation, secondary stenting was performed.
Medical TherapyAll patients received aspirin (100 mg daily) indefinitely and clopidogrel (75 mg daily) for three months after the intervention. Most patients started taking clopidogrel at least two days before the intervention; for those who did not, a loading dose of 300 mg of clopidogrel was given during the intervention.
Statistics AnalysisNo statistical tests were used. Data was expressed as mean ± standard deviation. Continuous variables were reported as mean standard deviation and median.
Results
Patients were assessed at post-operative day-1 and 3 month in the early post-operative period and following discharge. Primary end-point was technical success with popliteal access without any post-operative complications and low dosage opaque usage. Secondary end-point was 3 months follow-up stenosis degree. Postoperative creatinine values were acceptably increased, and the patients did not need dialysis treatment after the operation. A patency close to 100% was ensured. Dramatic response was obtained in the feet ulcer of 4 patients.
Discussion
Prevalence of peripheral arterial occlusive disease, among patients with renal failure and diabetes mellitus, is higher than the general population. Superficial femoral arteries (SFA) are often affected by atherosclerotic disease. But the optimal treatment strategy for femoro-popliteal occlusive disease remains controversial. Long-term patency has been poor following endovascular treatment of the SFA in diabetic patients, with 1-year patency rates as low as 22%. Angiography is part of those patients work-up. Contrast induced nephropathy (CIN) is a major concern in peripheral angiography.13 Prevention of CIN is of importance among these patients. Especially for diabetic patients post-anjiographic CIN occurs very often and it is a frightening complication after procedure. Post-contrast nephropathy is associated with a mortality of up to 34%. Also it causes consistenly dialysis treatment and a candidate for renal transplantion.14 The most important effective preventive strategy for CIN is reduction in contrast media volume. Besides there are some medications used before and after the procedure. Most of the publications focus on methods to reduce the incidence of CIN. Periprocedural hydration said to be protective.15 There are several other pharmacological therapies which have included N- acetyl sistein (NAC), calcium channel blockade, angiotensin-converting enzyme (ACE) inhibition, and dopamine and prostaglandin E1 administration. Statins have established benefits in the peripheral arterial disease (PAD).16,17 The increasing rate of known risk factors such as hypertension and diabetes in the population also increases the number of CRF patients. While the risk of cardiovascular disease doubles in the early stages of CRF, those who require dialysis are 30-50 times more at risk, and the main reason of mortality in these patients is cardiovascular disease.18,19 However, in cases where contralateral femoral puncture is used, which is frequently utilized, the relatively small vessel lumen in conjunction with a high plaque burden, slow flow, and a high frequency of primary occlusions contribute to a considerable rate of acute technical failures.20 Popliteal artery puncture both facilitates the manipulation in this region, where the retrograde approach is technically challenging, and minimizes the before mentioned complications of contralateral femoral puncture. Also, it protects the patient from CIN thanks to low radiopaque contrast use as it is closer to the lesion.21,22,23 Restenosis occurs in 40 to 60 percent of treated segments after one year.24,25 The use of angioplasty to treat extensive disease of the superficial femoral artery has particularly poor results: at one year, the rates of restenosis exceed 70 percent for lesions longer than 100 mm. Drug-coated balloon angioplasty (DCBA) was shown to be superior to standard balloon angioplasty (POBA) in terms of restenosis prevention for de novo superficial femoral artery disease.26,27
Conclusion
Optimal endovascular technique is still not well established. Patients have their own specilities that changes the strategy of the endovascular treatment. Each treatment modality should be associated with good technical success, effectiveness in reducing PAD symptoms. There are varying degrees of adverse events for endovascular treatments including distal embolization, arterial dissection, perforation, embolism and/or thrombosis, and restenosis. Therefore, these limitations of current devices warrant the development of new and better techniques and devices. Balloon angioplasty performed with ipsilateral popliteal artery micro-puncture manually results in low opaque use and allows the shortest way to access the target lesion in addition to minimizing the amount of opaque used for superficial femoral artery lesions. Therefore, renal protection was ensured before and after the operation without dialysis in diabetic patients with low EGFR and borderline high creatinine levels in the study group. Furthermore, complications that may occur in the femoral artery puncture site due to the micro-puncture into the popliteal artery such as pseudoaneurysm, dissection, and plaque rupture were prevented.
Declarations
Animal and Human Rights Statement
All procedures performed in this study involving human participants were in accordance with institutional and national ethical standards and the Declaration of Helsinki.
Informed Consent
Written informed consent was obtained from all participants prior to the procedure.
Conflict of Interest
The authors declare no conflict of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the scientific content of the article, including study design, data collection, analysis and interpretation, manuscript preparation, and approval of the final version of the manuscript.
References
-
Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FG, et al. Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II). J Vasc Surg. 2007;45(suppl S):S5-S67. doi:10.1016/j.jvs.2006.12.037
-
Wheatley B, Mansour A, Grossman PM, Munir KA, Cali RF, Gorsuch JM, et al. Complication rates for percutaneous lower extremity arterial antegrade access. Arch Surg. 2011;146:432-435. doi:10.1001/archsurg.2011.47
-
Kara KA, Hafız E, Deniz H, Arı M, Polat M, Güzel G. Successfully surgical repair of giant unruptured aneurysm of the sinus of Valsalva. J Clin Case Rep. 7:985.
-
Hu H, Zhang H, He Y, Jin W, Tian L, Chen X, et al. Endovascular nitinol stenting for long occlusive disease of the superficial femoral artery in critical limb ischemia: a single-center, mid-term result. Ann Vasc Surg. 2011;25:210-216. doi:10.1016/j.avsg.2010.09.013
-
Schillinger M, Mlekusch W, Haumer M, Sabeti S, Ahmadi R, Minar E. Angioplasty and elective stenting of de novo versus recurrent femoropopliteal lesions: 1-year follow-up. J Endovasc Ther. 2003;10:288-297. doi:10.1177/152660280301000219
-
De Jager DJ, Grootendorst DC, Jager KJ, van Dijk PC, Tomas LM, Ansell D, et al. Cardiovascular and noncardiovascular mortality among patients starting dialysis. JAMA. 2009;302:1782-1789. doi:10.1001/jama.2009.1488
-
Dearing DD, Patel KR, Compoginis JM, Kamel MA, Weaver FA, Katz SG. Primary stenting of the superficial femoral and popliteal artery. J Vasc Surg. 2009;50:542-548. doi:10.1016/j.jvs.2009.04.019
-
Solmaz FA, Karabacak P, Kara KA, Gülmen Ş, Okutan H. Effect of preoperative preparation for early extubation and discharge of intensive care unit. J Clin Anal Med. 2015;6(6):746-749.
-
McQuade K, Gable D, Hohman S, Pearl G, Theune B. Randomized comparison of ePTFE/nitinol self-expanding stent graft vs prosthetic femoral-popliteal bypass in the treatment of superficial femoral artery occlusive disease. J Vasc Surg. 2009;49:109-116. doi:10.1016/j.jvs.2008.08.041
-
Kara KA, Diliçıkık U, Sarıkaya B, Gülmen Ş. Treatment of Paget-Schroetter syndrome with a new anticoagulant therapy in young sportsman. EJCM. 2017. doi:10.15511/ejcm.17.00358
-
Sabeti S, Czerwenka-Wenkstetten A, Dick P, Schlager O, Amighi J, Mlekusch I, et al. Quality of life after balloon angioplasty versus stent implantation in the superficial femoral artery: findings from a randomized controlled trial. J Endovasc Ther. 2007;14:431-437. doi:10.1177/152660280701400401
-
Dippel E, Shammas N, Takes V, Coyne L, Lemke J. Twelve-month results of percutaneous endovascular reconstruction for chronically occluded superficial femoral arteries: a quality-of-life assessment. J Invasive Cardiol. 2006;18:316-321.
-
Kara KA. Bilateral semi-skeletonized IMA: less thermal injury, easier to harvest, early postoperative comparison with single IMA patients after CABG. Am J Clin Exp Med. 2018;6:107-112.
-
Lindholt JS. Radiocontrast-induced nephropathy. Eur J Vasc Endovasc Surg. 2003;25(4):296-304. doi:10.1053/ejvs.2002.1824
-
Solomon R. Contrast medium–induced acute renal failure. Kidney Int. 1998;53(1):230-242. doi:10.1038/sj.ki.4495510
-
Katzberg RW, Haller C. Contrast-induced nephrotoxicity: clinical landscape. Kidney Int Suppl. 2006;(100):3-7. doi:10.1038/sj.ki.5000366
-
Asif A, Epstein M. Prevention of radiocontrast-induced nephropathy. Am J Kidney Dis. 2004;44(1):12-24. doi:10.1053/j.ajkd.2004.04.001
-
Kara KA, Tuna MB, Gudelci T, Argun ÖB, Duygu E, Şener M. Erectile dysfunction severity and SYNTAX score in coronary artery disease. J Anesth Crit Care. 2017;8(5):296. doi:10.1016/j.amjcard.2017.03.119
-
Colak S, Azboy D, Temizturk Z, Atalay H, Dogan OF, Dogan D, et al. Renal outcomes and myocardial performance after on-pump beating heart versus conventional on-pump surgery in patients with preoperative low glomerular filtration rate. World J Cardiovasc Dis. 2016;6:433-445. doi:10.4236/wjcd.2016.611047
-
Youssef F, Gupta P, Seifalian AM, Myint F, Mikhailidis DP, Hamilton G. The effect of short-term treatment with simvastatin on renal function in patients with peripheral arterial disease. Angiology. 2004;55(1):53-62. doi:10.1177/000331970405500108
-
Nash K, Hafeez A, Hou S. Hospital-acquired renal insufficiency. Am J Kidney Dis. 2002;39:930-936. doi:10.1053/ajkd.2002.32766
-
Özkan H, Kiriş İ, Gülmen Ş, Okutan H, Solmaz FA, Kara KA. Incidence of development of aspirin resistance in the early postoperative period after coronary artery bypass surgery and inadequate inhibition of thromboxane A2 production. Turk Gogus Kalp Damar Cerrahisi Derg. 2016;1. doi:10.5606/tgkdc.dergisi.2018.15489
-
Hawkins IF. Carbon dioxide digital subtraction arteriography. AJR Am J Roentgenol. 1982;139:19-24. doi:10.2214/ajr.139.1.19
-
Kara KA. Use of multiple artery grafts to ensure long-term graft patency in coronary bypass surgeries. J Clin Anal Med. 2018.
-
Johnston KW. Femoral and popliteal arteries: reanalysis of results of balloon angioplasty. Radiology. 1992;183:767-771. doi:10.1148/radiology.183.3.1294068
-
Capek P, McLean GK, Berkowitz HD. Femoropopliteal angioplasty: factors influencing long-term success. Circulation. 1991;83(suppl 2):I70-I80.
-
Altinsoy HB, Alatas O, Khalil E, Kara KA, Okten CC, Dogan OF. A very rare cause of lower limb ischemia in young people: popliteal artery entrapment. Open Cardiovasc Med J. 2018;12:3. doi:10.2174/1874192401812010018
Figures
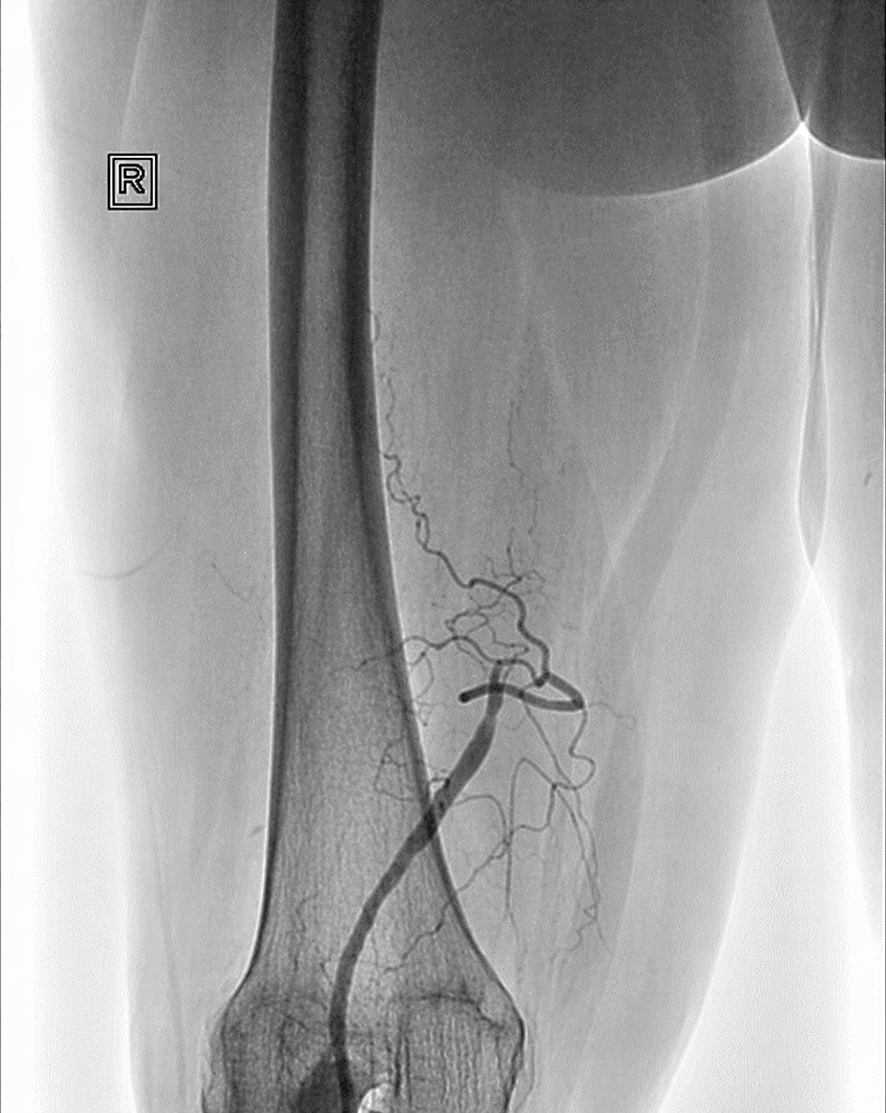
Figure 1. Pre-treatment
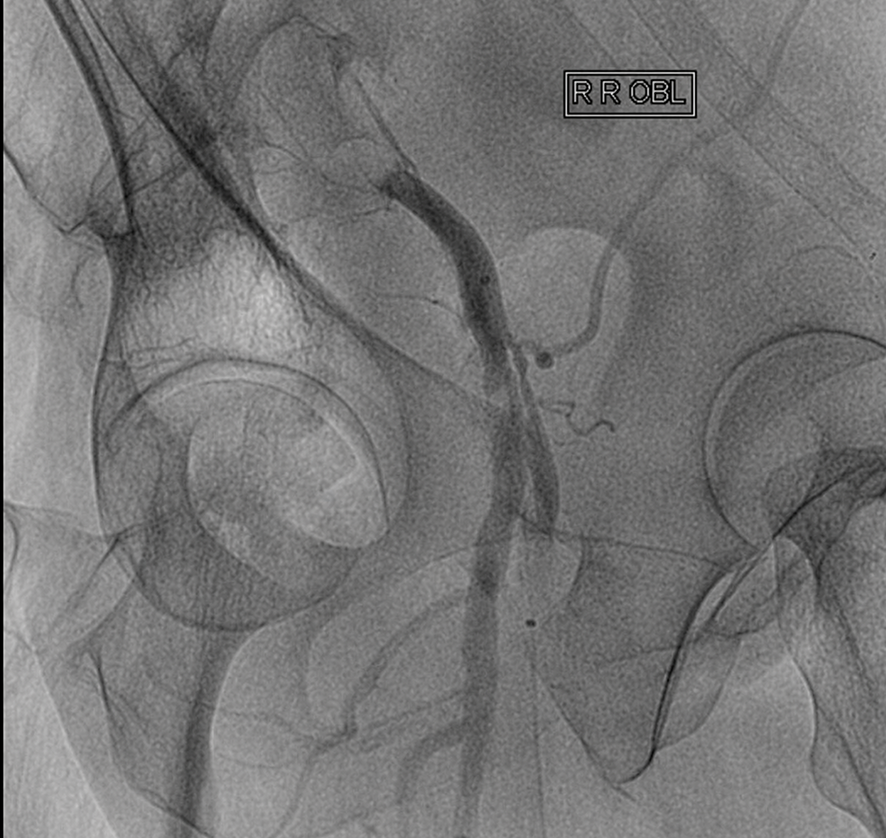
Figure 2. Pre-treatment
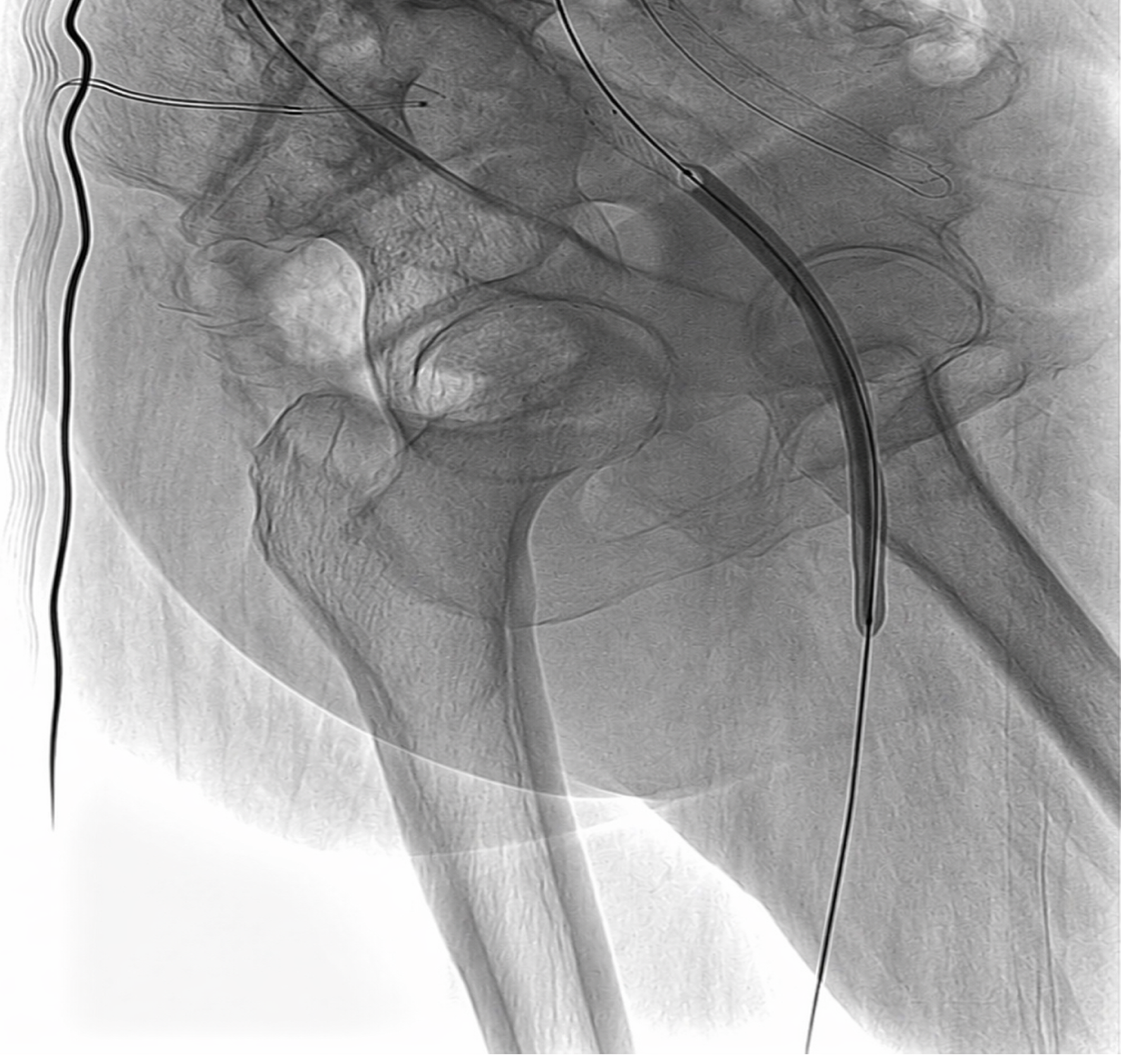
Figure 3. Balloon dilatation

Figure 4. Total occlusion
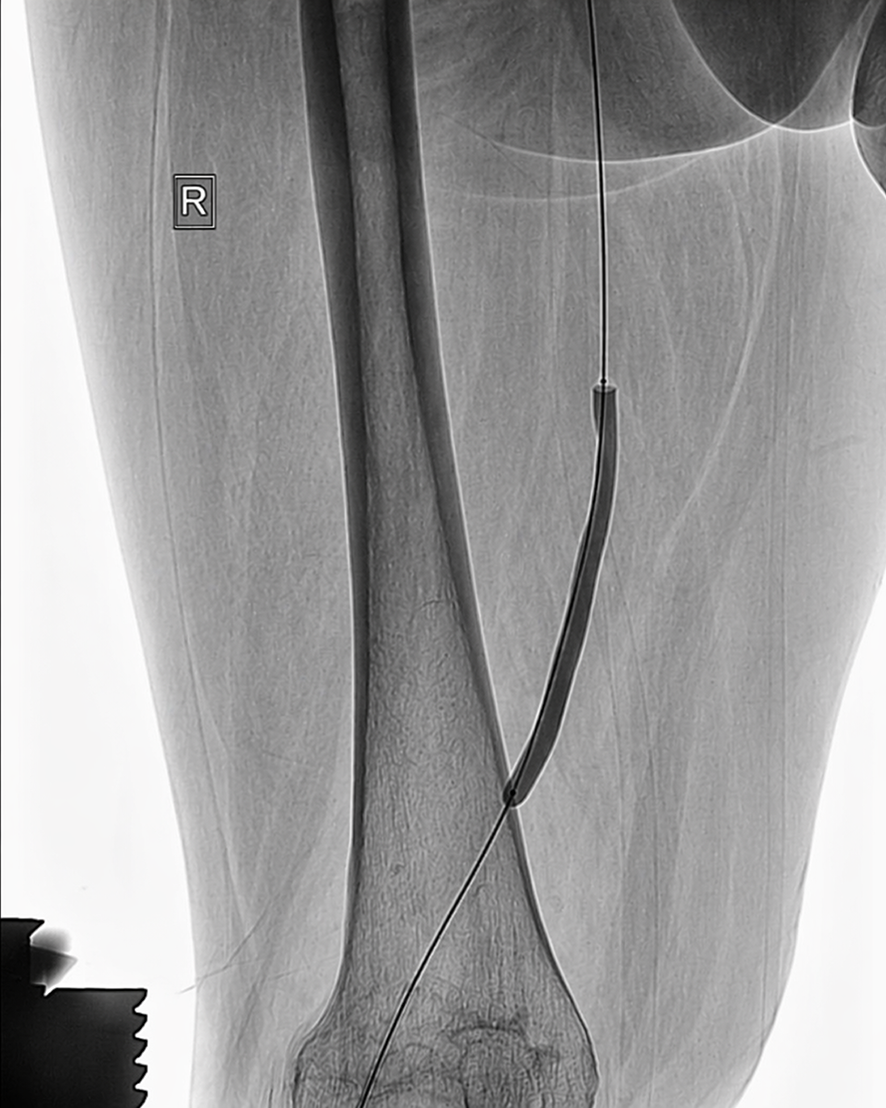
Figure 5. Balloon dilatation
Tables
Table 1. Preoperative demographic characteristics
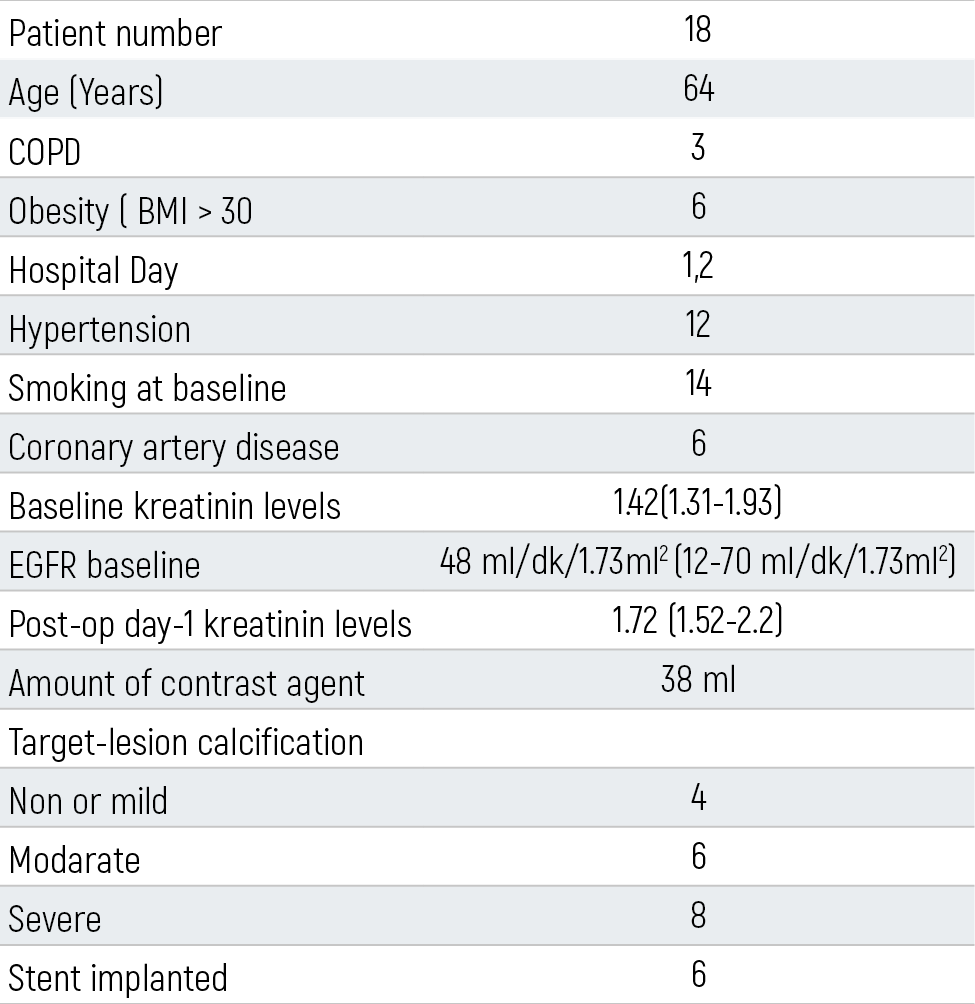
Chronic obstructive pulmonary disease; DM: Diabetes mellitus; BMI: Body mass index; NS: Non-significant.
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Süha Sadullah Özdilek, Fatma Ferda Kartufan, Soner Sanioğlu, Hakan Öntaş, Kayıhan Kara, Halit Yerebakan. Protection from renal injury with popliteal artery micro-puncture andminimized radiographic contrast use with critical SFA lesions, low EGFR, and high creatinine levels. Eu Clin Anal Med 2019;7(2):18-21. doi:10.4328/ECAM.10001
- Received:
- March 19, 2019
- Accepted:
- March 4, 2019
- Published Online:
- April 12, 2019
- Printed:
- May 1, 2019