Evaluation of cardiology consultations for patients receiving Covid-19 treatment in pandemic wards
Evaluation of cardiology consultations for Covid-19
Authors
Abstract
AimThe aim of this study was to investigate the reasons why cardiology consultation was requested from patients hospitalized to pandemic wards due to COVID-19 and what cardiac findings were obtained.
MethodsFifty-eight consecutive patients over the age of 18 who were treated for COVID-19 in a pandemic ward were included in the observational retrospective study. The demographic features of the patients were recorded. Cardiac biomarkers on consultation such as D-dimer, high sensitive cardiac troponin T (hs-cTn), and N terminal pro B type natriuretic peptide (NT-pro BNP) were recorded. Electrocardiography (ECG) was taken. Pleural effusion and pericardial effusion were determined from thorax computed tomography reports.
ResultsIn this study, we found the following findings in patients. The most common co-morbidity was hypertension (HT), which was detected in 35 (60.30%) patients. The most common reason for requesting consultation was ECG evaluation, which was the reason for cardiology evaluation in 45 (77.58%) patients. The most common ECG finding was atrial fibrillation that was found in 22 (37.90%) patients. The most common laboratory finding was an increase in d D-dimer levels in 44 (75.86%) patients. We detected 6 (10.34%) patients with non-ST segment elevation myocardial infarction (Non-STEMI), and anti-ischemic therapy was initiated. Pulmonary embolism was detected in 1 (1.72%) patient, and anticoagulant therapy was initiated. Four (6.80%) patients had acute pericarditis with pericardial effusion, and colchicine and steroid therapy were initiated.
ConclusionTherefore, COVID-19 patients who were followed in the pandemic ward should be evaluated by the cardiologist to investigate cardiac effects due to COVID-19 infection.
Keywords
Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which causes coronavirus disease 2019 (Covid-19), has resulted in a pandemic in the world. In December 2019, COVID-19 was first described in Wuhan, China, in patients complaining of flulike symptoms. World Health Organization declared COVID-19 as a pandemic on March 11, 2020. The exact effects of COVID-19 on the cardiovascular system are not well determined, but several case reports and reviews have been published. COVID-19 could directly cause cardiac and vascular injuries such as pericarditis, myocarditis, myocardial infarction, heart failure, arrhythmias or thromboembolic events.1 Such cardiac complications are shown both during the course of COVID-19 treatment and after the COVID-19 treatment is completed. The aim of this study was to investigate the reasons why cardiology consultation was requested from patients hospitalized in pandemic wards due to COVID-19 and which cardiac findings were obtained.
Materials and Methods
This study was an observational retrospective study. The Ministry of Health of the Republic of Turkey gave permission for the research. This research was conducted in accordance with the ethical principles of the Declaration of Helsinki and was approved by the local institutional review board, and waived the requirement for informed consent. The protocol was approved by the local ethics committee (approval date: April 8, 2021 approval number: 2021-42). Fifty-eight consecutive patients who were treated for COVID-19 in the pandemic ward in the last month were included in this retrospective study. All clinical, laboratory and outcome data were extracted from electronic medical records using a standardized data collection form and patient’s file from the archive. Demographic features of the patients age, female gender, chronic diseases (diabetes mellitus (DM), hypertension (HT), hyperlipidemia (HL), chronic kidney disease (CKD), chronic obstructive pulmonary disease (COPD), documented coronary artery diseases (CAD), heart failure (HF)) were recorded. Cardiac biomarkers on consultation D-dimer, high-sensitivity cardiac troponin T (hs-cTn), and N terminal pro B type natriuretic peptide (NT-pro BNP) were recorded. Electrocardiography (ECG) was taken. Normal sinus rhythm, atrial fibrillation, tachycardia, bradycardia findings were recorded on the ECG of the patients. Pleural effusion and pericardial effusion were determined from thorax computed tomography reports.
Patients over the age of 18 diagnosed with polymerase chain reaction test (PCR+) COVID-19, treated in the pandemic ward, who had cardiac complaints such as chest pain, shortness of breath, palpitation, back pain with consultation of a cardiologist were included in the study.Patients under 18 years of age and outpatient clinic patients were excluded from the study.
All statistical analyses were performed using IBM SPSS statistics version 26 software. The data were summarized as median (minimum – maximum), mean SD ± or number (percentage %), where appropriate. The Shapiro-Wilk and Kolmogorov-Smirnov tests were used to determine the normality of the variables.
Results
We included 58 patients over the age of 18, diagnosed with PCR-confirmed COVID-19, followed in COVID-19 pandemic ward and who were requested to consult a cardiologist. Thirty-four (58.6%) patients were women and 24 (41.4%) were men. The mean age was 69.57±15.03 years. Accompanying comorbidities in all patients were as follows: DM 18 (31.00%), HT 35 (60.30%), HL 10 (17.20%), CAD 15 (25.90%), COPD 10 (17.20%), HF 4 (6.80%),CKD (glomerular filtration rate lower 60) 18 (31.00%). The basic clinical characteristics of the patients, including age, gender, comorbidities are listed in Table 1.
The most common reason for requesting consultation was an ECG evaluation (45 (77.58%)) (Table 2). Other reasons, in order of frequency, were as follows: elevated D-dimer level (44 (75.86%)), elevated hs-cTn level (39 (67.24%)), elevated NT-pro BNP level (36 (62.06%)), pleural effusion (16 (27.58%)), warfarin dosage adjustment (8 (13.79%)) and pericardial effusion (4 (6.89%)).
Median hs-cTn level was 83.11 (3.3-1260.00) ng/L, median NT-pro BNP level was 6696.37 (15-35000) pg/mL, median D-dimer level was 1.85 (0.20-8.50) μg/ml. The normal hs-cTn level was 0-14 ng/L, the normal NT-pro BNP level was 0-125 pg/mL, the normal D-dimer level was μg/ml in our hospital laboratory. Atrial fibrillation was detected in 22 (37.90%) patients, tachycardia in 6 (10.34%) patients, non-ST segment elevation myocardial infarction (Non-STEMI) in 6 patients, pulmonary embolism in 1 (1.72%) patient and bradycardia in 1 (1.72%) patient. Laboratory, ECG and thorax computed tomography reports findings of patients on examination are shown in Table 3.
Discussion
Patients over the age of 18 who were diagnosed with PCR-confirmed COVID-19 and were followed in the COVID-19 pandemic wards and whose cardiology consultation was requested were included in the study. Most of the patients were women 34 (58.6%); three of them were pregnant. D-dimer levels of all three pregnant women were high. Additionally, one pregnant woman had high hs-cTn and NT-pro BNP levels. There are many unknowns for pregnant women during COVID-19. During the pregnancy period, physiological changes have a significant impact on the immune system, respiratory system, cardiovascular function and coagulation.2 Pregnancy is a hypercoagulable state and increases intravascular inflammation.3
In this study, the most common co-morbidity associated with the patients was HT; 35 patients (60.34%). Zhou F et al reported that the most common comorbidity was hypertension (30 %).4 There is no evidence that the outcomes of COVID-19 are associated with hypertension.
Four (6.80%) patients had acute pericarditis with pericardial effusion. Treatment with colchicine and steroids was initiated. None of the patients had signs of cardiac tamponade. Like other viral infections, COVID-19 may trigger cascades of inflammatory pathways and this may lead to pericarditis and pericardial effusion similar to other viral infections. In a recent case study, researchers showed the presence of COVID-19 in the pericardial fluid using PCR analysis on pericardial fluid.5 Another post-mortem study described histopathological findings and viral tropism in patients who died from severe COVID-19. Full postmortem examinations were done in nine patients with confirmed COVID-19, including sampling of all major organs. Major unexpected findings included acute pericarditis in two out of nine (22%) patients.6 The most common ECG finding associated with the patients was atrial fibrillation (22 (37.9%) patients). But warfarin dosage adjustment was only in 8 (13.79%) patients. Warfarin was initiated after the examination in these patients at an interval of 2 to 3. Patients taking oral anticoagulants due to atrial fibrillation before hospitalization for COVID-19, enoxaparin therapy, or continuing treatment with existing oral anticoagulants have been a matter of debate.
When the laboratory findings were analyzed, elevated D-dimer levels were detected in 44 (75.86%) patients. The severe form of COVID-19 can be complicated by coagulopathy, namely disseminated intravascular coagulation, which is rather prothrombotic in nature with a high risk of venous thromboembolism.7 COVID-19 was associated with hemostatic abnormalities and markedly elevated D-dimer levels.8,9 Pulmonary embolism was detected in one patient (1.72%), and added anticoagulant therapy was initiated.
We detected elevated hs-cTn levels in 39 (67.24%) patients. A total of six patients were diagnosed with non-ST segment elevation myocardial infarction and anti-ischemic therapy was initiated. An increase in hs-cTn may occur without acute myocardial infarction, including myocardial ischemia, increased wall tension and ventricular strain, direct myocyte trauma, excess catecholamines, and possibly impaired renal clearance.10 Therefore, patients with high troponin values should be evaluated along with their clinical findings and ECG.
We detected elevated NT-pro BNP levels in 36 (62.06 %) patients. NTpro BNP levels increase in heart failure,11 chronic kidney disease12 and cirrhosis.13 In our study, 18 (31%) patients had chronic kidney disease, none of the patients had cirrhosis, 4 (6.89%) patients had left ventricular heart failure with a low ejection fraction. It is thought that in patients with extensive lung involvement, patients with preserved ejection fraction may have NT-pro BNP levels increase due to right ventricular strain. Until now, there has been no study in the literature investigating the purposes for which cardiology consultation was requested in patients hospitalized in pandemic wards due to COVID-19, and what cardiac findings were obtained from the consultation.
Limitations
This study has several limitations. Firstly, the study was a single-center and retrospective study. Secondly, the number of patients participating in the study was small. In order to reveal the cardiac effects of COVID-19, studies in larger study groups are needed.
Conclusion
In this study, we found the following findings in patients: the most common comorbidity was HT in 35 (60.30 %) patients, the most common reason for requesting consultation was an ECG evaluation in 45 (77.58 %) patients, the most common ECG finding was atrial fibrillation in 22 (37.90 %) patients, the most common laboratory finding was elevated D-dimer level in 44 (75.86 %) patients. We detected 6 (10.34%) patients with non-ST segment elevation myocardial infarction (Non-STEMI) and anti-ischemic therapy was initiated. Pulmonary embolism was detected in 1 (1.72%) patient, and anticoagulant therapy was initiated. Four (6.80%) patients had acute pericarditis with pericardial effusion and colchicine, and steroid therapy were initiated. Therefore, COVID-19 patients who are followed-up in the pandemic ward should be evaluated by a cardiologist to investigate cardiac effects caused by COVID-19 infection.
Declarations
Animal and Human Rights Statement
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the Declaration of Helsinki and its later amendments.
Informed Consent
Due to the retrospective nature of the study, informed consent was waived.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Conflict of Interest
The author declares no conflict of interest.
Funding
None.
Scientific Responsibility Statement
The author declares that she is responsible for the scientific content of the article, including study design, data collection, analysis and interpretation, manuscript preparation, and approval of the final version of the manuscript.
Abbreviations
CAD: Coronary artery disease
CKD: Chronic kidney disease
COPD: Chronic obstructive pulmonary disease
COVID-19: Coronavirus disease 2019
DM: Diabetes mellitus
ECG: Electrocardiography
HF: Heart failure
HL: Hyperlipidemia
hs-cTn: High-sensitivity cardiac troponin
HT: Hypertension
Non-STEMI: Non-ST segment elevation myocardial infarction
NT-pro BNP: N-terminal pro-B-type natriuretic peptide
PCR: Polymerase chain reaction
SARS-CoV-2: Severe acute respiratory syndrome coronavirus 2
References
-
Su YB, Kuo MJ, Lin TY, et al. Cardiovascular manifestation and treatment in COVID-19. J Chin Med Assoc. 2020;83(8):704-709. doi:10.1097/jcma.0000000000000352
-
Wastnedge EAN, Reynolds RM, van Boeckel SR, et al. Pregnancy and COVID-19. Physiol Rev. 2021;101(1):303-318. doi:10.1152/physrev.00024.2020
-
Di Renzo GC, Giardina I. Coronavirus disease 2019 in pregnancy: consider thromboembolic disorders and thromboprophylaxis. Am J Obstet Gynecol. 2020;223(1):135. doi:10.1016/j.ajog.2020.04.017
-
Zhou F, Yu T, Du R, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395:497-506.
-
Farina A, Uccello G, Spreafico M, Bassanelli G, Savonitto S. SARS-CoV-2 detection in the pericardial fluid of a patient with cardiac tamponade. Eur J Intern Med. 2020;76:100-101. doi:10.1016/j.ejim.2020.04.045
-
Hanley B, Naresh KN, Roufosse C, et al. Histopathological findings and viral tropism in UK patients with severe fatal COVID-19: a postmortem study. Lancet Microbe. 2020;1(6):e245-e253. doi:10.1016/s2666-5247(20)30115-4
-
Zhang L, Long Y, Xiao H, Yang J, Toulon P, Zhang Z. Use of D-dimer in oral anticoagulation therapy. Int J Lab Hematol. 2020;42(suppl 1):48-55.
-
Tang N, Li D, Wang X, Sun Z. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J Thromb Haemost. 2020;18(4):844-847. doi:10.1111/jth.14768
-
Danzi GB, Loffi M, Galeazzi G, Gherbesi E. Acute pulmonary embolism and COVID-19 pneumonia: a random association? Eur Heart J. 2020;41(19):1858. doi:10.1093/eurheartj/ehaa254
-
Giannitsis E, Katus HA. Cardiac troponin level elevations not related to acute coronary syndromes. Nat Rev Cardiol. 2013;10:623-634. doi:10.1038/nrcardio.2013.129
-
Palazzuoli A, Gallotta M, Quatrini I, Nuti R. Natriuretic peptides (BNP and NT-proBNP): measurement and relevance in heart failure. Vasc Health Risk Manag. 2010;6:411-418. doi:10.2147/vhrm.s5789
-
Niizuma S, Iwanaga Y, Washio T, et al. Clinical significance of increased cardiac troponin T in patients with chronic hemodialysis and cardiovascular disease: comparison to B-type natriuretic peptide and A-type natriuretic peptide increase. Kidney Blood Press Res. 2019;44(5):1050-1062. doi:10.1159/000502232
-
Henriksen JH, Gøtze JP, Fuglsang S, Christensen E, Bendtsen F, Møller S. Increased circulating probrain natriuretic peptide (proBNP) and brain natriuretic peptide (BNP) in patients with cirrhosis: relation to cardiovascular dysfunction and severity of disease. Gut. 2003;52(10):1511-1517. doi:10.1136/gut.52.10.1511
Tables
Table 1. The basic clinical characteristics of the patients
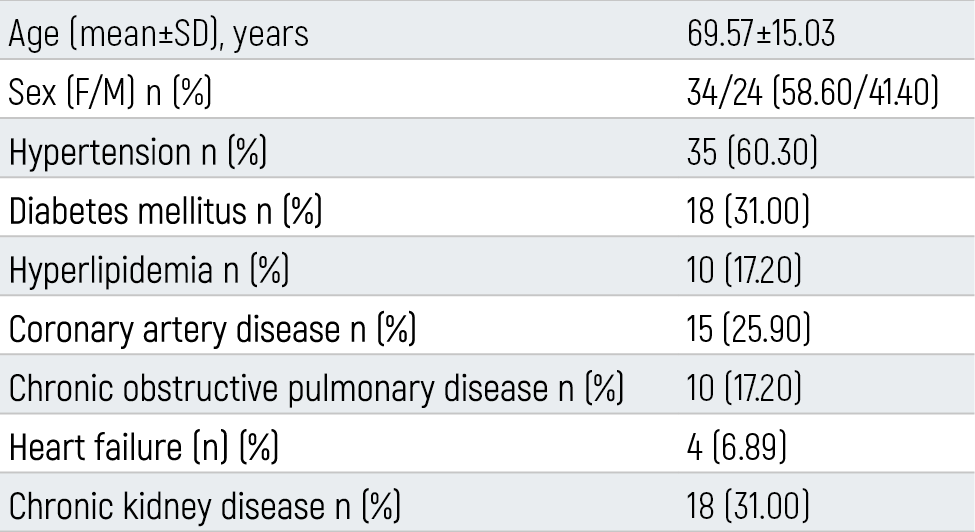
n: number SD: standard deviation M: male F: female
Table 2. Reason for requesting consultation
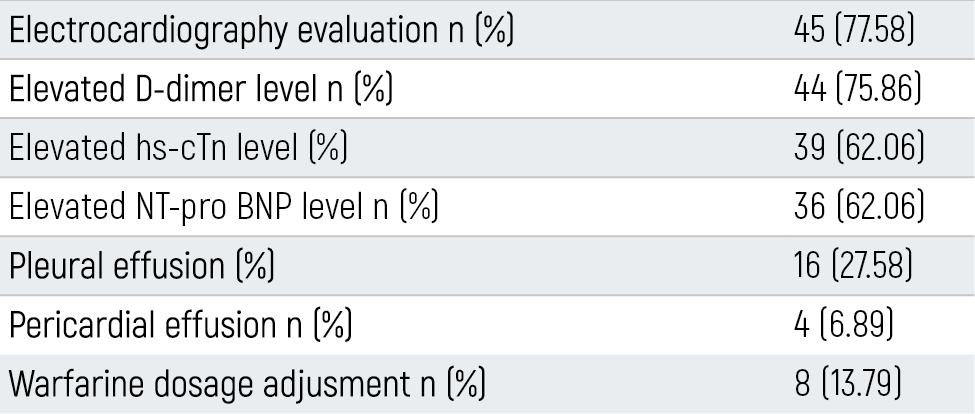
Table 3. Laboratory, ECG and thorax computed tomography reports findings
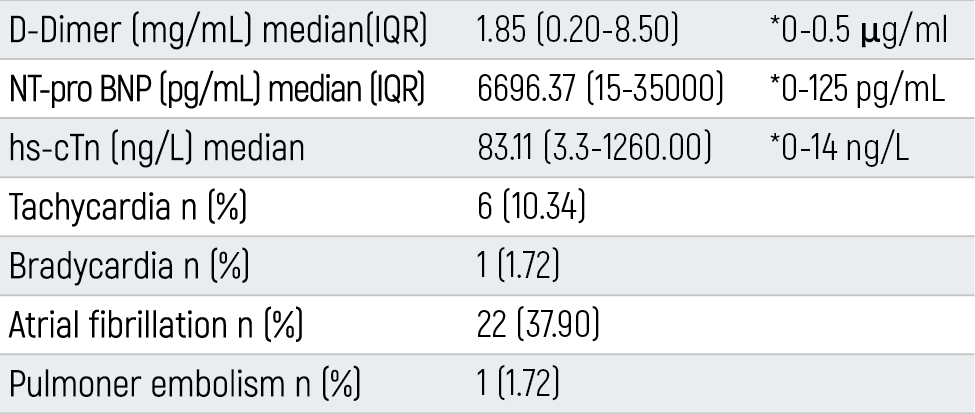
*: Normal refence range
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Gulay Aydın. Evaluation of cardiology consultations for patients receiving Covid-19 treatment in pandemic wards. Eu Clin Anal Med 2021;10(2):9-11. doi:10.4328/ECAM.10030
- Received:
- April 11, 2021
- Accepted:
- May 12, 2021
- Published Online:
- May 27, 2021
- Printed:
- May 1, 2021