Platelet-lymphocyte ratio as a potential marker in minor head traumas in emergency department admissions
Platelet-lymphocyte ratio in minor head traumas
Authors
Abstract
AimNeutrophil-Lymphocyte Ratio (NLR) and Platelet-Lymphocyte Ratio (PLR) are the blood biomarkers that are the indicators of the systemic inflammatory response. In this study, the utility of PLR, as a simple and effective blood biomarker that can be used in rapid diagnosis and treatment decision-making in patients that applied to emergency services with minor head trauma, was studied.
MethodsThe relationship between PLR and intracranial injury in patients who applied to the emergency department of our university hospital with a minor head trauma between January 01, 2018 and December 31, 2018, with the approval of the local ethics committee of our university, was retrospectively studied. Within this scope, tomography reports and laboratory results were retrospectively analyzed by scanning patient files through the hospital information management system. Computed tomography findings, age, application type, blood values were obtained and analyzed through the system. The data were analyzed using the SPSS program.
ResultsOf the 200 patients studied, 99 (49.5%) were women and 101 (50.5%) were men, and the mean age was 60.47±23.8 years. Ischemic infarction was detected in 11 (5.5%) patients, subarachnoid hemorrhage in 8 (4%), subdural hematoma in 6 (3%), intra parenchymal hematoma in 4 (2%), and epidural hematoma in 1 (0.5%) patient. When the patients with and without intracranial pathology after trauma were compared, when comparing the mean NLR and PLR (p=0.055), no statistically significant difference was found.
ConclusionEven though NLR and PLR have a field of use in the follow-up and treatment of progressive diseases, the results are still controversial. There is no significant relationship for the use of NLR and PLR as a biomarker in deciding the diagnosis and treatment of patients with severe head trauma with minor or intracranial pathology.
Keywords
Introduction
According to statistics, a head trauma occurs every 15 seconds, and death occurs every 12 minutes due to a serious head trauma.1,2 Admission to the emergency department after a minor head trauma is one of the most common injuries. Minor head traumas characterized by Glasgow Coma Score (GCS) 15 points, loss of consciousness less than 20 minutes, and no neurological deficits constitute 80% of all head traumas in emergency service admissions.3 It has been suggested in clinical studies that NLR and PLR can be used as prognostic markers in diseases such as intracerebral hemorrhage, cerebral ischemia, and myocardial infarction.4 It was stated, in a study published by Baskent University Faculty of Medicine within the framework of the search for new biomarkers that cost-effective tests that could provide rapid results to emergency physicians would be beneficial in renal transplant patients, and red blood cell distribution width (RDW) was suggested as a candidate in this regard.5 PLR is one of the parameters of the complete blood count just like RDW, and is calculated by a physician by dividing the platelet and lymphocyte counts obtained during the complete blood count by each other. NLR is calculated by dividing the absolute neutrophil count by the absolute lymphocyte count, and PLR is expressed as multiplying the platelet count by the absolute lymphocyte count. NLR ≥ 5 and PLR ≥ 250 values are considered high levels.6 As of 08.07.2020, a search made with the keywords “platelet lymphocyte ratio (PLR)” on Pubmed, the official website of the United States National Library of Medicine, yielded 3,262 results. According to Pubmed, it has been reported that PLR, which has been studied since 2008, can be used as a predictor in various cancers, acute inflammatory demyelinating polyradiculoneuropathy, attention deficit, and hyperactivity disorder, and erectile dysfunction.7,8,9,10,11,12 Lymphocytes and platelets, as members of the systemic inflammatory response family, have been noted to be positively associated with carcinogenesis and tumor progression.13,14 Although NLR and PLR are blood biomarkers that are indicators of a systemic inflammatory response, the clinical significance of the combinations of these biomarkers is unclear.15 While there is a negative correlation with PLR values above the cut-off value in terms of survival in ovarian cancers and cervical cancers, there is no scientific connection in endometrial cancers. PLR is scientifically higher in progressive diseases than in non-progressive diseases.16 In a study related to cardiovascular diseases, when the NLR ratio was evaluated in terms of atherosclerosis progression, when patients with atherosclerosis progression were compared with the patients without progression, it was observed that the scientifically increased NLR ratio in patients with progressive atherosclerosis was found to be significant.17 Rui Guo et al. evaluated 171 patients and found in a study conducted in 2019 that NLR was high in patients hospitalized for 90 days in patients with a history of head trauma and diagnosed with intraparenchymal hemorrhage according to Computed Tomography (CT) results. Although the distribution of unconsciousness and low GCS is more common in the patient group with high NLR, it can be used as a biomarker for severe strokes.18 High NLR mean is also significant in terms of forensic traumatology, as a new parameter to suggest that the injury is not mild. Although an increase in the PLR environments was observed in groups with or without life-threatening injuries, which may and may not be resolved by simple medical intervention, with and without traumatic change detected , with and without fracture, in terms of determining the severity of the injury, no statistically significant difference was found between these variables.19 It was demonstrated in another study, conducted by Muratoğlu Murat et al. and included 326 patients who claim that PLR is an acceptable biomarker in showing the presence of infection, although it does not provide as excellent results as C-Reactive Protein (CRP), which is accepted as the gold standard in the study.20 In this study, it was aimed to show whether PLR was useful in detecting intracranial injury in patients applying to the emergency department with minor head trauma. There are indications for the use of computed tomography (CT) for patients applying to the emergency department with head trauma and GCS; however, this decision and CT imaging can be difficult due to overcrowded emergency rooms or exaggerated patient complaints. Patients who applied to our emergency department with minor head traumas were evaluated, and it was aimed to investigate the relationship between brain pathology on CT and hematological biomarkers in order to find markers that helped us define brain pathology in patients with GCS 15.
Materials and Methods
In this retrospective study, the relationship between PLR and intracranial injury in patients who applied to the emergency department of our university hospital with minor head traumas between January 01, 2018 and December 31, 2018, with the approval of the local ethics committee of our university, was retrospectively investigated. Within this scope, tomography reports and laboratory results were retrospectively analyzed by scanning patient files through the hospital information management system. The age, gender, whether there was an intracranial injury in tomography images related to head trauma, complete blood count values (leukocytes, erythrocytes, thrombocytes, neutrophils, lymphocytes, MPV, RDW), GCSs at the time of admission were obtained in this way. The results of examinations of the patients who applied to our emergency department with minor head traumas between January 01, 2018 and December 31, 2018 as a control group and did not have intracranial injuries were evaluated. Thus, it was tried to show whether there was a difference between the results of comparison and complete blood count parameters in patients with and without intracranial injury who applied to the emergency department due to minor head trauma. A total of 200 people with GCS=15 who applied to our emergency department with minor head trauma were included in the study. The case group consisted of 30 patients who underwent CT scan and found pathology, and the control group consisted of 170 patients whose CT scans were evaluated within normal limits. While the patient files were being reviewed, a detailed neurological examination in the patient’s history, causes of trauma (non-vehicle traffic accident, in-vehicle traffic accident, headache, beating, falling, work accident, seizure, syncope, suicide), and patients’ complaints (headache, nausea, vomiting, loss of consciousness and seizure duration) were recorded. The results of routine complete blood count and biochemical tests taken from these patients, CT scan results, whether the patient was hospitalized, the treatment received, and the final status of the patients were recorded. CT scan was performed with Siemens Somatom Force Computed Tomography device (384 sections ) within 30-60 minutes of admission to the emergency department. Subdural hemorrhage, subarachnoid hemorrhage, epidural hemorrhage, intraparenchymal hemorrhage, and ischemic infarction were considered as pathologies when CT scan was evaluated. Patients with GCS below 15, patients with multiple traumas, chest pain, comorbidities such as anemia, or chronic kidney failure that affected blood parameters were excluded from the study. The blood test results were reviewed at the first admission of the patients to the emergency department of our hospital. Blood samples were collected in tubes containing sodium citrate, blood samples for troponin T were collected in pure, red-capped tubes and analyzed at room temperature in the biochemistry laboratory using the Pentra DF Nexus, Hariba medical device, and troponin T was analyzed with the Roche Hitachi Cobas E 601 device. Patients’ WBC (White Blood Cell) 4.5-11.0 × 103 / µL, Hb (Hemoglobin) 13.5-16.0 g / dL, NEU (Neutrophil) 2-12 K / mL, LYM (Lymphocyte)1 -4.9 K/mL, MCV (mean corpuscular volume) 80–100 fL, RDW (Red Cell Distribution) 11.8-14.3%, MPV *(Mean Platelet Volume) 6.910.8 fL, PLT (Platelet count) 156–373 × 103/µL and troponin T 14–100 pg/mL were considered normal limits.
Ethics ApprovalEthics committee approval was obtained before conducting the study.
Statistical AnalysisWe analyzed all data with the "SPSS 17.0 for Windows" program. The demographic, clinical, and laboratory data of the patients were shown as mean ± standard deviation, median (interquartile range (IQR), and percent (%). The Chi-square test was used for the comparison of categorical data. The distribution of continuous data was evaluated with the Kolmogorov-Smirnov Test. The results of this test revealed that none of the data were normally distributed. Therefore, the MannWhitney U test was applied, which is a non-parametric test, in the analysis of the data. The “receiver operating characteristic” (ROC) curve was plotted to determine the sensitivity and specificity of the PLR and CRP, which is considered the gold standard in indicating an infection. For those below the ROC curve, values above 0.9 were determined as excellent, values between 0.8-0.9 as very good, and between 0.7-0.8 as acceptable values. The data were analyzed in the 95% confidence interval, and the p<0.05 value was considered statistically significant.
Reporting GuidelinesThe study was reported in accordance with STROBE guidelines.
Results
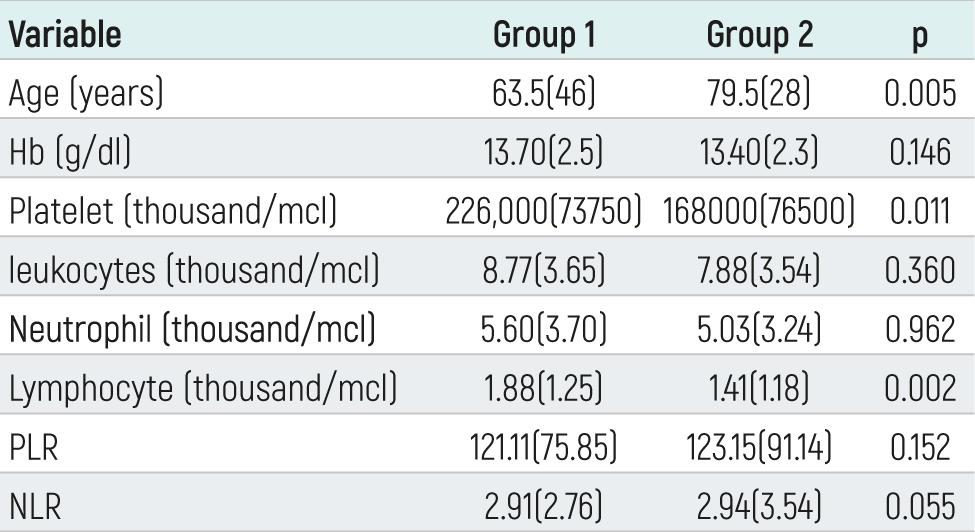
Of the 200 examined cases, 99 (49.5%) were women and 101 (50.5%) were men, and the mean age was 60.47±23.8 years (Table 1). Of the cases, 5 (2.5) were pedestrians, 12 (6%) in-vehicle traffic accidents, 14 (7%) assaults, 130 (65%) falls, and 39 (19.5%) applied to the emergency service due to other reasons. The number of patients with GCS 13 was 8 (4%), 14 was 4 (2%), and 15 was 188 (94%). One hundred seventy (85%) patients had no pathological findings when CT images were examined. Ischemic infarction was detected in 11 (5.5%), subarachnoid hemorrhage in 8 (4%), subdural hematoma in 6 (3%), intraparenchymal hematoma in 4 (2%), and epidural hematoma in 1 (0.5%). A statistically significant correlation was found for the platelet area under the curve 0.354 CI (0.245-0.463) (p=0.011)(Figure 1). The sensitivity was 73% and the specificity was 12% for the platelet 160.500 value. The area under the curve for lymphocytes was 0.324 CI (0.207-0.465) (p=0.002), a statistically significant difference was found. The sensitivity was calculated as 83%, the specificity as 5.3% for the lymphocyte value of 0.90. No statistically significant difference was found when the NLR averages were compared (p=0.055). Similarly, no statistically significant difference was found in PLR averages (p=0.152).
Discussion
This study aims to determine the use of NLR and PLR as alternatives in determining the severity of head trauma in patients presenting to the emergency department with minor head traumas, the intensity of the emergency department, and in small centers that do not have the opportunity for further examination and treatment such as CT. The fact that the ratios of neutrophils, lymphocytes, and platelets, which are among the parameters of complete blood count, to each other are both cost-effective and rapid-resulting biomarkers, alternatively, it may be effective and useful in decision-making. In our study, it was found that NLR and PLR were not scientifically significant in patients who applied with head traumas and had pathology on CT. The results we determined in both the case group and the control group did not show a correlation for NLR (p=0.055) and PLR (p=0.152). In the literature, there are scientific studies and articles stating that NLR and PLR values are correlated in the follow-up of progressive diseases such as infection, various cancers, and cardiac atherosclerotic diseases, which are accepted as indicators of systemic inflammatory response. In our study, it was intended to determine whether this correlation was significant, especially in patients with minor head traumas. A systemic inflammatory response occurs in traumatic or non-traumatic intracranial events, but since organic pathology does not occur in minor head traumas or because the time required for the inflammatory response to occur at the first admission is short, this response may not have occurred, and it can be concluded that both systemic and temporal factors act.
Even though lymphocytes are part of the systemic inflammatory response and there is a positive association between platelets and cancers, the scientific significance of these biomarkers is still unclear.13,14,15 In addition to parameters, which are the gold standard in determining the follow-up and treatment, such as CRP, which is one of the members of the systemic response in infections, inflammation, cancers, and chronic diseases, it shows an increase and decrease in neutrophils and lymphocytes. In this context, although the ratio of these parameters to each other is not the gold standard as an additional biomarker in follow-up and treatment, there are articles supporting its usability. On the other hand, publications that support its usability in the follow-up and treatment of progressive diseases in studies and articles made and published for PLR or reporting that there is a correlation are rare. In our study, both NLR (p=0.055) and PLR (p=0.152) did not show a scientifically significant correlation in patients who applied to our emergency department with minor head traumas and had intracranial pathologies on CT images. Although the change processes of blood parameters, which occur within a certain period, while the systemic inflammatory response occurs, and whose values change according to the severity of the disease and the response to treatment, are accepted as an indicator, the fact that this process has not yet started or is not completed in cases such as acute and rapidly developing head trauma limits the use of NLR and PLR values in diagnosis and treatment. However, it has been reported that NLR is high during hospitalization in patients with post-traumatic intracranial hemorrhage.18 The difference between the correlation in this study and the lack of correlation in our study is that the follow-up of the systemic inflammatory response with the patients who applied to the emergency department after the event and followed up for 90 days and their progression was observed. Likewise, no statistically significant difference was found in cases with traumatic changes in terms of forensic medicine.19 The reason why this correlation did not occur in forensic cases can be thought of as the systemic inflammatory response process not being activated or completed yet. In a study published by Acar E. et al., a significant increase was found in MPV, NLR, and troponin T levels of patients with pathologies on CT who applied to the emergency department with minor head traumas.20 In the same study, no significant difference was found for NLR and PLR in patients with skull fracture and intracranial hemorrhage. Although some blood parameters such as neutrophils and lymphocytes may be expected to increase due to the systemic inflammatory response, it is not clear whether their ratios correlate to each other in pathologies that following head trauma. This may be significant in patients undergoing surgery, which may again be due to the systemic response after post-surgery. In this case, it is imperative to make sense of whether the correlation of NLR and PLR is due to trauma or as a response to the surgical procedure. Since neutrophil and lymphocyte values vary in chronic diseases, cancers, and many other diseases that cause a systemic inflammatory response, their averages or ratios to each other may also vary, so an increase in isolated head trauma can be expected, it will be a very optimistic approach to establish a specific correlation or evaluate it as a pathognomonic biomarker.21
Conclusion
Although NLR and PLR can be used as inflammatory biomarkers in response to the follow-up and treatment in progressive diseases, their specific use as a biomarker in decision-making, especially in acute events such as minor head trauma, is not appropriate alone. Similarly, its use as a biomarker is not evident in patients with intracranial pathology.
Declarations
Ethics Declarations
The authors declare that all procedures performed in this study were conducted in accordance with institutional, national, and international ethical standards.
Animal and Human Rights Statement
All procedures performed in this study involving human participants were conducted in accordance with the ethical standards of the institutional and national research committee and with the Declaration of Helsinki and its later amendments.
Informed Consent
Due to the retrospective nature of the study, informed consent was waived.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Conflict of Interest
The authors declare no conflict of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the scientific content of the article, including study design, data collection, analysis and interpretation, manuscript preparation, and approval of the final version of the manuscript.
Abbreviations
CRP: C-reactive protein
CT: Computed tomography
GCS: Glasgow Coma Scale
IQR: Interquartile range
MPV: Mean platelet volume
NLR: Neutrophil-lymphocyte ratio
PLR: Platelet-lymphocyte ratio
RDW: Red cell distribution width
ROC: Receiver operating characteristic
SPSS: Statistical Package for the Social Sciences
WBC: White blood cell
References
-
Dalbayrak S, Gumustas S, Bal A, Akansel G. Early and delayed CT findings in patients with mild-to-moderate head trauma. Turk Neurosurg. 2011;21(4):591-598. doi:10.5137/1019-5149.jtn.3570-10.2
-
Gentry LR. Imaging of closed head injury. Radiology. 1994;191(1):1-17. doi:10.1148/radiology.191.1.8134551
-
Boran BO, Barut N, Akgün C, Çelikoğlu E, Bozbuğa M. Indications for computed tomography in patients with mild head injuries. Ulus Travma Acil Cerrahi Derg. 2005;11:218-223
-
Giede-Jeppe A, Bobinger T, Gerner ST, Sembill JA, Sprügel MI, Beuscher VD, et al. Neutrophil-to-lymphocyte ratio is an independent predictor for in-hospital mortality in spontaneous intracerebral hemorrhage. Cerebrovasc Dis. 2017;44(1-2):26-34
-
Kayipmaz AE, Findik M, Kavalci C, Akdur A, Moray G, Haberal M. Red blood cell distribution width increases during infection in renal and liver graft recipients. Exp Clin Transplant. 2017;15(1):61-64. doi:10.6002/ect.2015.0167
-
Proctor MJ, Morrison DS, Talwar D, Balmer SM, Fletcher CD, O’Reilly DS, et al. A comparison of inflammation-based prognostic scores in patients with cancer: a Glasgow Inflammation Outcome Study. Eur J Cancer. 2011;47(17):2633-2641. doi:10.1016/j.ejca.2011.03.028
-
Kutlucan L, Kutlucan A, Basaran B, Dagli M, Basturk A, Kozanhan B, et al. The predictive effect of initial complete blood count of intensive care unit patients on mortality, length of hospitalization, and nosocomial infections. Eur Rev Med Pharmacol Sci. 2016;20(8):1467-1473. doi:10.5505/actamedica.2016.98159
-
Sasaki H, Nagano S, Komiya S, Taniguchi N, Setoguchi T. Validation of different nutritional assessment tools in predicting prognosis of patients with soft tissue spindle-cell sarcomas. Nutrients. 2018;10(6). doi:10.3390/nu10060765
-
Tao Z, Li SX, Cui X, Huang Y, Zhu S, Wang Y, et al. The prognostic value of preoperative inflammatory indexes in gallbladder carcinoma with hepatic involvement. Cancer Biomark. 2018. doi:10.3233/CBM-181230
-
Zhu M, Feng M, He F, Han B, Ma K, Zeng X, et al. Pretreatment neutrophil-lymphocyte ratio and platelet-lymphocyte ratio predict clinical outcome and prognosis for cervical cancer. Clin Chim Acta. 2018;483:296-302. doi:10.1016/j.cca.2018.05.025
-
Ozdemir HH. Analysis of the albumin level, neutrophil-lymphocyte ratio, and platelet-lymphocyte ratio in Guillain-Barré syndrome. Arq Neuropsiquiatr. 2016;74(9):718-722. doi:10.1590/0004-282X20160132
-
Avcil S. Evaluation of the neutrophil/lymphocyte ratio, platelet/lymphocyte ratio, and mean platelet volume as inflammatory markers in children with attention-deficit hyperactivity disorder. Psychiatry Clin Neurosci. 2018. doi:10.1111/pcn.12659
-
DeNardo DG, Coussens LM. Inflammation and breast cancer: balancing immune response: crosstalk between adaptive and innate immune cells during breast cancer progression. Breast Cancer Res. 2007;9(4):212. doi:10.1186/bcr1746
-
Lal I, Dittus K, Holmes CE. Platelets, coagulation and fibrinolysis in breast cancer progression. Breast Cancer Res. 2013;15(4):207. doi:10.1186/bcr3425
-
Hirahara T, Arigami T, Yanagita S, Matsushita D, Uchikado Y, Kita Y, et al. Combined neutrophil-lymphocyte ratio and platelet-lymphocyte ratio predicts chemotherapy response and prognosis in patients with advanced gastric cancer. BMC Cancer. 2019;19(1):672. doi:10.1186/s12885-019-5903-y
-
Shanshan J, Jiandong L, Xiangyi C, Xinfei Z, Junhao R, Aihua Y, et al. Platelet-lymphocyte ratio as a potential prognostic factor in gynecologic cancers: a meta-analysis. Arch Gynecol Obstet. 2019;300(4):829-839
-
Kalay N, Dogdu O, Koc F, Yarlioglues M, Ardic I, Akpek M, et al. Hematologic parameters and angiographic progression of coronary atherosclerosis. Angiology. 2012;63(3):213-217. doi:10.1177/0003319711412763
-
Guo R, Wu Y, Chen R, Yu Z, You C, Ma L, et al. Clinical value of neutrophil-to-lymphocyte ratio in primary intraventricular hemorrhage. World Neurosurg. 2019. doi:10.1016/j.wneu.2019.04.040
-
Kalkan E, Çakır D, Türkön H, Gül A. Adli travmatolojik açıdan yaralanmanın ağırlığını belirlemede nötrofil-lenfosit oranı ve trombosit-lenfosit oranının rolü [The role of neutrophil-lymphocyte ratio and platelet-lymphocyte ratio in determining the severity of injury in forensic traumatology]. Bozok Med J. 2018. doi:10.16919/bozoktip.427319
-
Acar E, Demir A, Alatas ÖD, Beydilli H, Yıldırım B, Kırlı U, et al. Evaluation of hematological markers in minor head trauma in the emergency room. Eur J Trauma Emerg Surg. 2016;42(5):611-616. doi:10.1007/s00068-015-0579-8
-
Muratoglu M, Kayipmaz AE, Kavalci C, Kirnap M, Moray G, Haberal M. Platelet-to-lymphocyte ratio as a potential indicator of infection-associated emergency visits of renal transplant recipients. Exp Clin Transplant. 2019
Figures
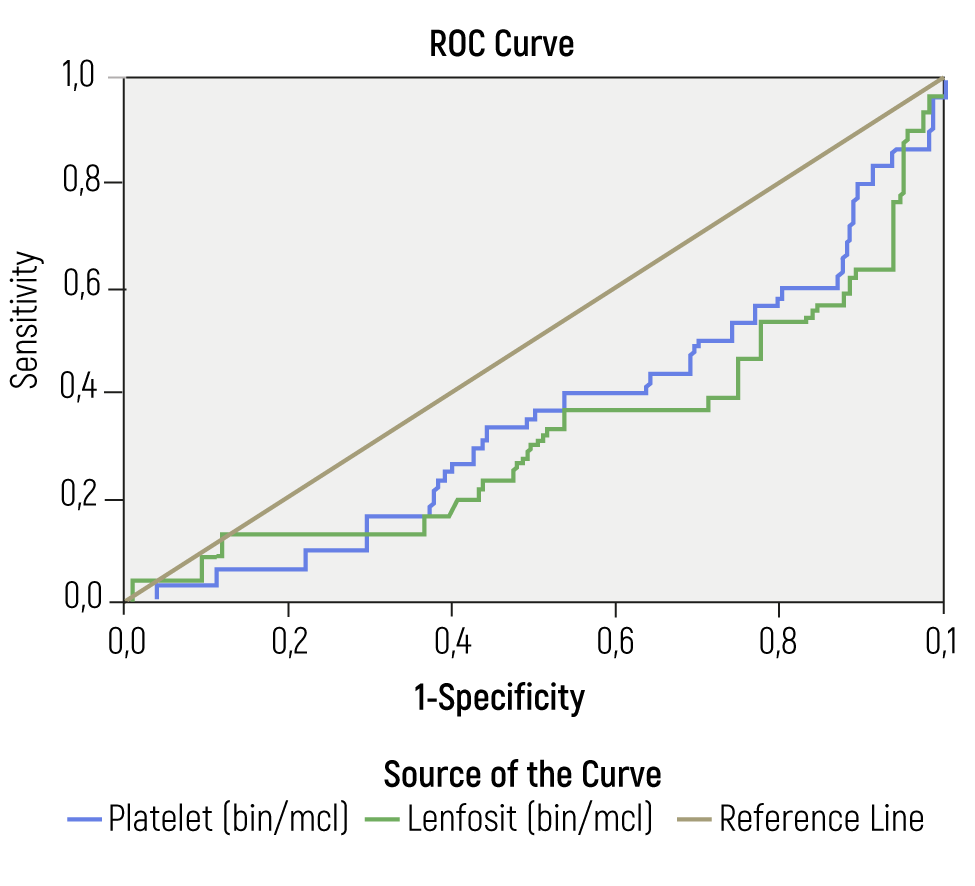
Figure 1. The “receiver operating characteristic” (ROC) curve was plotted to determine the sensitivity and specificity of the PLR and CRP
Tables
Table 1. Characteristics of the patients, laboratory parameters, and no lesion on CT (Group 1), patients with lesion on CT (Group 2)
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Murat Muratoglu, Hayrettin Meftun Kaptan, Ishaaq Sakwa Eshikumo, Ebru Biyikli. Platelet-lymphocyte ratio as a potential marker in minor head traumas in emergency department admissions. Eu Clin Anal Med 2022;10(1):1-4. doi:10.4328/ECAM.10032
- Received:
- September 13, 2021
- Accepted:
- October 9, 2021
- Published Online:
- December 31, 2021
- Printed:
- January 1, 2022