Role of intestinal barrier and dysfunction in cancer cachexia
Intestinal barrier and cachexia
Authors
Abstract
AimIn this study, we aimed to determine whether weight loss could be estimated by measuring small intestine function in patients who will start chemotherapy.
MethodsSerum TRAF 6, citrulline and TNF α, hs-CRP, transferrin, ceruloplasmin levels were compared with controls and tumor stages.
ResultsIn patients with weight loss after chemotherapy, a statistically significant correlation was found with basal serum citrulline levels.
ConclusionPatients who had weight loss according to the pre-chemo stage had lower levels of serum citrulline compared to patients who did not lose weight.
Keywords
Introduction
Cancer is the second most common cause of death today, and at least 50% of deaths in end-stage cancer patients are associated with cancer-related cachexia. Cachexia is a multifactorial syndrome characterized by skeletal muscle mass loss, leading to progressive functional impairment, and it should be irreversible with standard nutritional support.1 Cancer-associated cachexia is a metabolic syndrome with a multiorgan involvement with muscle and fat reduction.2,3 In our clinical practice, cancer patients begin to lose weight at an unknown time during chemotherapy, and in many patients, this loss is irrepressible. For this reason, we are strongly in need of markers to predict weight loss at baseline. The small intestine is the most important organ that regulates the nutrition of a human. While the surface area of the small intestine in our body is 0.5 m2 (5mt length x 10cm circumference), the functional area of the epithelium is 250 m².4 The explanation of this 500-fold increase is associated with the villus structure. Villus is coated with enterocytes and is an essential element in the absorption function.5 In order for the small intestines to perform this function, the structural integrity of the enterocytes, the paracellular permeability, the reduced mucosal immunity, and the mucus structure must be complete. Both cancer itself and chemotherapeutic agents have adverse effects on the small intestine. In this context, we aimed to determine whether measuring small intestine function can estimate weight loss in patients who start chemotherapy. As a catabolism indicator, we examined the patients’ serum albumin, protein, and TRAF 6 levels. In addition, we investigated serum ceruloplasmin and transferrin levels to exclude possible serum intestinal malabsorption status and serum citrulline levels as an indicator of small bowel function reserve. Finally, hs-CRP levels were examined to rule out inflammations.
Materials and Methods
This prospective study was conducted between September 2016 and January 2018. The study was carried out with 64 patients clinically and radiologically diagnosed as cancer histological. Patients included in this study had cachexia as a new finding, and their body mass indexes were 18.5 and below (patient group). Twenty-one healthy subjects were included in the control group. The exclusion criteria for the control group were the operation of the gastrointestinal system, depressive mood, smoking and alcohol consumption, regular medication use, and recent changes in eating habits. Body mass index values between 18.5-24.9 were considered normal, values of 18.5 and below were considered weak, and values of 25 and over were considered as overweight. Criteria for inclusion in the study were a diagnosis of cancer and receiving chemotherapy for cancer diagnosis. Criteria for exclusion in the study were history of previous chemotherapy due to another cancer, intensive alcohol use, initial body mass index <16, small bowel resection (> 60%), having a disease that can cause chronic malnutrition, uncontrolled chronic disease that will lead to weight loss (diabetes mellitus, chronic renal failure, chronic pancreatitis, chronic obstructive pulmonary disease, short bowel syndrome), a disease leading to chronic malnutrition. Serum TRAF 6, citrulline, and TNF α levels were measured by commercially available Molgen branded ELISA kits. The levels of hsCRP, transferrin, and ceruloplasmin were measured by commercially available Medisis brand ELISA kits. The study was carried out with the Bio-Tek branded (Vermont, USA) ELx 50 washing device, while the ELISA plates were read on the ELx800 ELISA plate reader.
Statistical AnalysisFor statistical analysis, statistical-package for social sciences for Windows 18.0 (SPSS 18 inc) program was used. Descriptive statistical methods (mean, standard deviation, frequency distribution, %) were used when evaluating study data, and ANOVA and Fischer’s test was used to compare categorical data. Before the quantitative data were analyzed, the Kolmogorov-Smirnov test was used to evaluate the normal distribution. In comparing the two independent groups, data with normal distribution were evaluated by ANOVA test, and the data with abnormal distribution were evaluated with the Mann-Whitney U test. The Kruskal-Wallis test was used to compare more than two groups. The non-parametric Spearman Test was used for correlation analysis. The results were evaluated at a 95% confidence interval and p <0.05 at the significance level.
Ethical ApprovalThis study was approved by the Sakarya University Hospital Board of Ethics on 22/08/2016 and numbered 16214662 / 050.01.04 / 119. This study was supported by the Sakarya University Scientific Research Projects (BAP) with project number: 2017-40-02-004.
Results
Our study involved 64 cancer patients and 21 healthy individuals. There were 48 women (75%) and 16 men (25%) in the cancer group. In the healthy control group, there were 7 males and 14 females. In the study group, 29 patients had lung cancer, 11 patients had breast cancer, 6 patients had gastric cancer, 5 patients had colon cancer, and the remaining 8 patients were diagnosed with kidney, prostate, head–neck, and pancreatic cancer. The other 5 patients had Hodgkin lymphoma, malignant melanoma, bladder cancer, paraganglioma, and testicular cancer. There were 18 patients at the early stage, 16 at the local advanced stage, and 30 at the metastatic stage. Hs-CRP levels were significantly higher in the patient group compared to the control group (21.8mg/l vs 1.8mg/l, p = 0.0001), similarly ceruloplasmin levels were also significantly higher (0.49 g/l vs 0.24 g/l p = 0.001). Serum transferrin levels were similar in both groups (2.48g/l vs 2.40g/l p = 0.53). Serum citrulline levels were significantly higher in the control group (248pg/ml vs 103pg/ml p = 0.0001). SerumTRAF-6 levels were significantly higher in the control group (384pg/ml vs 209pg/ml p = 0.001). Serum TNF-alpha levels were higher in the control group but not statistically significant (277pg/ml vs 215pg/ml p=0.07) (Table 1).
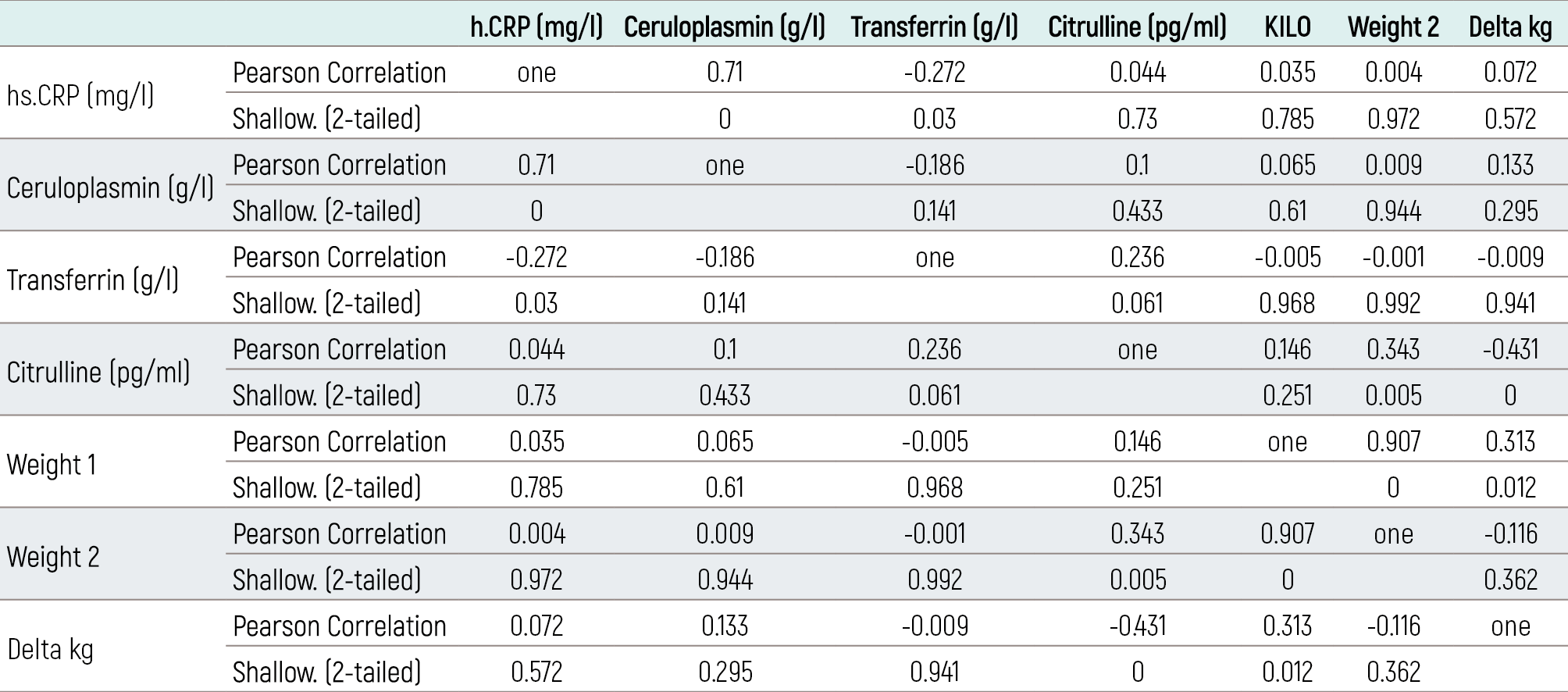
When the patients were classified according to their stages, it was statistically significant in serum hs-CRP, ceruloplasmin, citrulline, and TRAF-6 levels (p=0.002, 0.0001, 0.0001, 0.001, respectively). No significant difference was found in Transferrin and TNF-alpha (p=0.73, 0.32, respectively). Hs-CRP levels were highest in the metastatic phase (30.6 mg / l). Ceruloplasmin levels were highest at the metastatic stage (0.52g /l). The stage with the lowest serum citrulline levels was the metastatic stage (82pg / ml). TRAF-6 levels were also at the lowest metastatic stage (192pg / ml), similar to citrulline (Table 2). A statistically significant correlation was found with basal serum citrulline levels in patients with weight loss after chemotherapy. A negative correlation was found between citrulline level and weight change. Overall survival was 15 months in patients who lost weight during chemotherapy and 29 months who had not (P: 0.001). In the Coxregression model, hs-CRP and serum citrulline levels were significant with overall survival (p-value = 0.02 and 0.008, respectively). Cox-linear regression analysis revealed two parameters related to OS. For the hsCRP and citrulline levels, the p-value was 0.006 and 0.003, respectively. The parameters examined in the correlation analysis were hs-CRP, ceruloplasmin, transferrin, citrulline, pre-and post-treatment weight loss (Table 3).
Discussion
This study investigated the relationship between intestinal function and weight loss during chemotherapy in cancer patients. According to the pre-chemo stage, patients who had weight-loss had lower serum citrulline levels than patients who did not lose weight. Also, multivariate analyses showed that serum citrulline levels were significantly correlated with OS in patients with weight loss. Plasma citrulline (C6H13N3O3) is an amino acid, and the primary source of citrulline in our bodies is enterocytes. Citrulline is synthesized in the mitochondria of mature enterocytes and contains 80% glutamine as a precursor.6 In our country, there are no clear data on the mean serum citrulline levels, but in the literature, it is reported that citrulline levels in western societies are 20-60 micromol/L.7 In the control group of our study, this value was median 157 pg/ml. Serum citrulline is produced in enterocytes, and it turns into arginine and is excreted by the kidney. Reduced serum citrulline is associated with decreased enterocyte function in individuals with normal renal function. Studies have shown that plasma citrulline levels are an accurate indicator of small bowel function. This is a confirmed finding in short bowel syndrome.8,9 Serum citrulline levels have been shown to decrease in many studies in intensive care patients. This decrease was observed in 21 patients who were followed up after cardiac arrest and 16 after septic shock.10,11 In addition, it has been shown that decreased serum citrulline levels below 10 micromol/lt increase mortality in intensive care units.12 In another study, 100 patients with stem cell transplantation were investigated for chemotherapy-induced gastrointestinal mucositis, and serum citrulline levels were observed to decrease below 10 micromol/lt. In this study, it was observed that serum citrulline level predicted mucositis better than albumin.13 In addition, the researchers have emphasized that serum citrulline is not a negative acute phase reactant such as albumin. Our study showed the relationship between serum citrulline levels and weight loss and concluded that gastrointestinal function loss would be better predicted with citrulline than albumin. Serum citrulline levels are known to show small bowel function independent of diet and nutritional status.14 In our study, serum citrulline levels were statistically lower in the patient group than in the control group. It has been suggested that cancer patients begin their treatment with lower enterocyte performance and that it is one of the first causes of rapid weight loss in cancer patients. According to the stage, serum citrulline levels were significantly lower in the metastatic stage than in the early stages. This may be an explanation for the faster weight loss in metastatic patients. The production of pro-inflammatory cytokines in cancer patients triggers systemic inflammation and leads to an acute phase response.15 As a result of increased catabolism, albumin synthesis decreases, and atrophy develops in skeletal muscles. An acute-phase reactant, CRP, is also involved in the regulation of the immune response and is an indicator of poor prognosis in cancer patients.16 For the hsCRP, there is no satisfactory data. However, it has been reported that there is a 7% increase in breast cancer risk with a 2-fold increase in hsCRP level.17 In another study, the relationship between hsCRP increase and increased breast cancer mortality was reported.18 In another study, the relationship between hsCRP increase and increased breast cancer mortality was reported. No relationship was found between HsCRP and weight loss, and in fact, it contributed to the acceptance of serum citrulline levels as evidence of GUT function independent of inflammation.
The TRAF 6 protein is a member of both the TNF family and the Tol/IL-1 family and is associated with the synthesis of pro-inflammatory cytokines. The TRAF family is a cytoplasmic protein that undertakes negative control of apoptosis and survival-related functions.19 The mechanism of cancer cachexia has not yet been elucidated, and the atrophic process in the skeletal muscles is emphasized. In a study, a muscle biopsy was performed in 102 patients with gastric cancer and cachexia due to muscle atrophy, and TRAF-6 expression in muscle tissue was compared with the control group. As a result of the study, it was found that the expression of TRAF-6 was significantly higher in the atrophic muscle tissue than in the control group.20 In an in vivo study, TRAF 6 synthesis was suppressed, and cachexia was inhibited in mice. In the study conducted by Bilir et al., it was found that TRAF 6 levels were significantly higher in cachectic patients than in noncachectic patients.21 In our study, there was no significant difference between the levels of TRAF 6. However, TNF alpha levels were higher than the control group. No relationship was found between the levels of TRAF 6 and TNF alfa according to stage or weight. One of the reasons for this finding is that patients are newly diagnosed, and the process of refractory cachexia has not yet begun. The insufficient number of patients can explain another reason.One of our study’s most important limitations is that we do not follow citrulline levels during the treatment period. The second point is that the patient numbers do not show an equal distribution between the groups according to the cancer types. However, in the literature, we think it is valuable because it is the first study to predict weight loss and citrulline levels in cancer patients.
Conclusion
In conclusion, our study showed a relationship between basal intestinal function measurement and weight loss in cancer patients for the first time in the literature. Despite the missing points in our study, citrulline can be used as a marker to predict the period of cachexia in cancer patients, and perhaps citrulline can be used as a criterion of success in the treatment response.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors have no conflict of interest to disclose.
Funding
This study was supported by Sakarya University BAP (project number: 2017-40-02-004).
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content including study design, data collection, analysis and interpretation, writing, some of the main line, or all of the preparation and scientific review of the contents and approval of the final version of the article.
References
-
Fearon K, Strasser F, Anker SD, Bosaeus I, Bruera E, Fainsinger RL, et al. Definition and classification of cancer cachexia: an international consensus. Lancet Oncol. 2011;12(5):489-495. doi:10.1016/s1470-2045(10)70218-7
-
Uomo G, Gallucci F, Rabitti PG. Anorexia-cachexia syndrome in pancreatic cancer: recent developments in research and management. JOP. 2006;7(2):157-162.
-
Baiti NB, Davis MP. Cytokines and cancer anorexia-cachexia syndrome. Am J Hosp Palliat Med. 2008;25(5):407-411.
-
Crawley SW, Mooseker MS, Tyska MJ. Shaping the intestinal brush border. J Cell Biol. 2014;207:441-451. doi:10.1083/jcb.201407015
-
Thomson AB, Cheeseman CI, Keelan M, Fedorak R, Clandinin MT. Crypt cell production rate, enterocyte turnover time and appearance of transport along the jejunal villus of the rat. Biochim Biophys Acta. 1994;1191(1):197-204. doi:10.1016/0005-2736(94)90249-6
-
van de Poll MC, Ligthart-Melis GC, Boelens PG, Deutz NE, van Leeuwen PA, Dejong CH. Intestinal and hepatic metabolism of glutamine and citrulline in humans. J Physiol. 2007;581(Pt 2):819-827. doi:10.1113/jphysiol.2006.126029
-
Crenn P, Coudray-Lucas C, Thuillier F, Cynober L, Messing B. Postabsorptive plasma citrulline concentration is a marker of absorptive enterocyte mass and intestinal failure in humans. Gastroenterology. 2000;119(6):1496-1505. doi:10.1053/gast.2000.20227
-
Crenn P, Messing B, Cynober L. Citrulline as a biomarker of intestinal failure due to enterocyte mass reduction. Clin Nutr. 2008;27:328-339. doi:10.1016/j.clnu.2008.02.005
-
Crenn P, Vahedi K, Lavergne-Slove A, Cynober L, Matuchansky C, Messing B. Plasma citrulline: a marker of enterocyte mass in villous atrophy-associated small bowel disease. Gastroenterology. 2003;124(5):1210-1219. doi:10.1016/s0016-5085(03)00170-7
-
Grimaldi D, Guivarch E, Neveux N, Fichet J, Pène F, Marx JS, et al. Markers of intestinal injury are associated with endotoxemia in successfully resuscitated patients. Resuscitation. 2013;84(1):60-65. doi:10.1016/j.resuscitation.2012.06.010
-
Crenn P, Neveux N, Chevret S, Jaffray P, Cynober L, Melchior JC, et al. Plasma L-citrulline concentrations and its relationship with inflammation at the onset of septic shock: a pilot study. J Crit Care. 2014;29(2):315.e1-315.e6. doi:10.1016/j.jcrc.2013.11.015
-
Piton G, Manzon C, Monnet E, Cypriani B, Barbot O, Navellou JC, et al. Plasma citrulline kinetics and prognostic value in critically ill patients. Intensive Care Med. 2010;36(4):702-706. doi:10.1007/s00134-010-1751-6
-
van der Velden WJ, Herbers AH, Brüggemann RJ, Feuth T, Donnelly JP, Blijlevens NM. Citrulline and albumin as biomarkers for gastrointestinal mucositis in recipients of hematopoietic stem cell transplantation. Bone Marrow Transplant. 2013;48(7):977-981. doi:10.1038/bmt.2012.278
-
Crenn P, Hanachi M, Neveux N, Cynober L. Circulating citrulline levels: a biomarker for intestinal functionality assessment. Ann Biol Clin. 2011;69:513-521. doi:10.1684/abc.2011.0609
-
Gabay C, Kushner I. Acute-phase proteins and other systemic responses to inflammation. N Engl J Med. 1999;340(6):448-454. doi:10.1056/nejm199902113400607
-
Tan BH, Deans DA, Skipworth RJ, Ross JA, Fearon KC. Biomarkers for cancer cachexia: is there also a genetic component to cachexia? Support Care Cancer. 2008;16(3):229-234. doi:10.1007/s00520-007-0367-z
-
Visser M, Bouter LM, McQuillan GM, Wener MH, Harris TB. Elevated C-reactive protein levels in overweight and obese adults. JAMA. 1999;282(22):2131-2135. doi:10.1001/jama.282.22.2131
-
Frydenberg H, Thune I, Lofterød T, Mortensen ES, Eggen AE, Risberg T, et al. Prediagnostic high-sensitivity C-reactive protein and breast cancer risk, recurrence, and survival. Breast Cancer Res Treat. 2016;155(2):345-354. doi:10.1007/s10549-015-3671-1
-
Plewka A, Madej P, Plewka D, Nowaczyk G, Morek M, Bogunia E, et al. The TRAF2 and TRAF6 expression in myomas and myometrium of women in reproductive and perimenopausal age. Folia Histochem Cytobiol. 2010;48(3):407-416. doi:10.2478/v10042-010-0039-6
-
Sun YS, Ye ZY, Qian ZY, Xu XD, Hu JF. Expression of TRAF6 and ubiquitin mRNA in skeletal muscle of gastric cancer patients. J Exp Clin Cancer Res. 2012;31:81. doi:10.1186/1756-9966-31-81
-
Bilir C, Engin H, Can M, Temi YB, Demirtas D. The prognostic role of inflammation and hormones in patients with metastatic cancer with cachexia. Med Oncol. 2015;32(3):56. doi:10.1007/s12032-015-0497-y
Tables
Table 1. Comparison of laboratory values of groups, FBG (Fasting Blood Glucose)
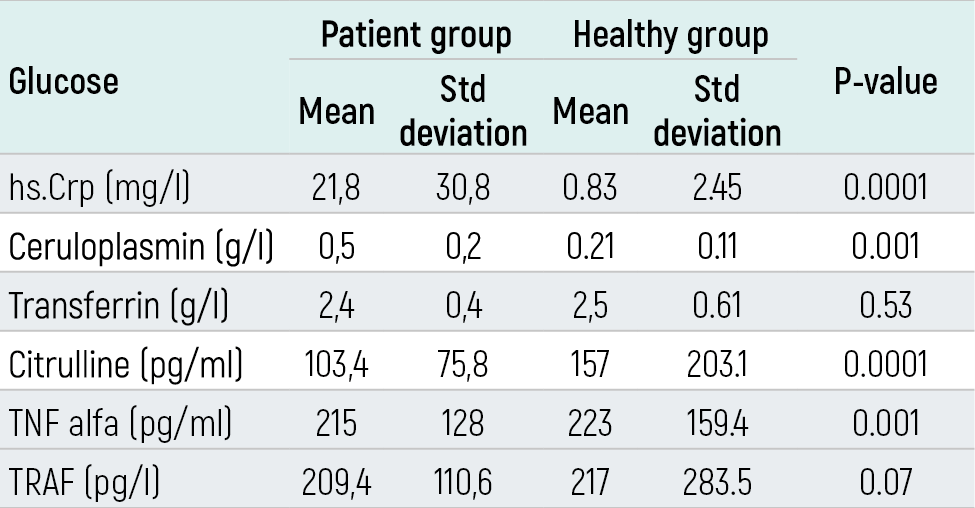
Table 2. Study parameters of patients according to stage
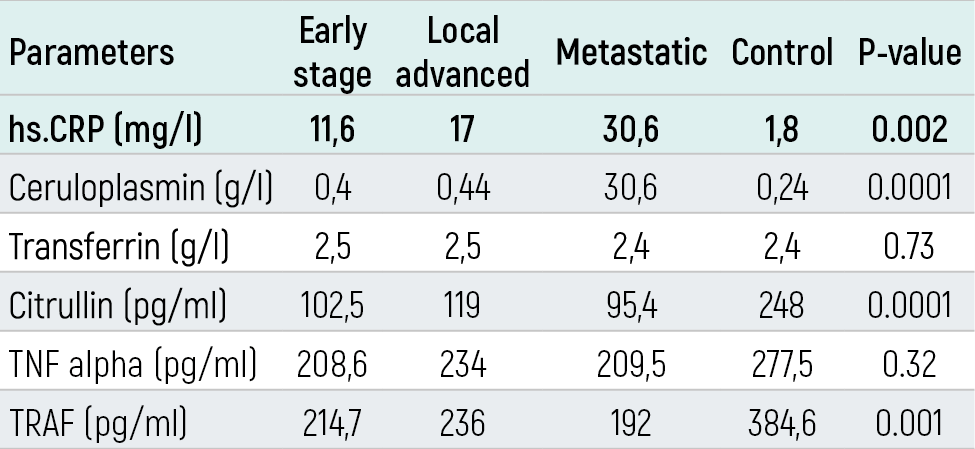
Table 3. Correlation of parameters with each other
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Zeynep Ergenç, Hasan Ergenç, Özlem Özkul, Ayşe Erdoğan Çakar, Fatma Behice Cinemre, Cemil Bilir. Role of intestinal barrier and dysfunction in cancer cachexia. Eu Clin Anal Med 2022;10(3):27-30. doi:10.4328/ECAM.10045
- Received:
- September 27, 2022
- Accepted:
- October 11, 2022
- Published Online:
- October 11, 2022
- Printed:
- September 1, 2022