Primary solid pseudopapillary neoplasm of the ovary: A Case Report and Literature Review
Primary solid pseudopapillary neoplasm of the ovary
Authors
Abstract
IntroductionSolid pseudopapillary neoplasm (SPN) is an uncommon neoplasm of the pancreas. Extrapancreatic cases of SPN are exceedingly rare. To the best of our knowledge, the primary SPN of the ovary was reported in only 13 cases.
,Case PresentationWe report a case located in the right ovary in a 30-year-old woman, morphologically and immunophenotypically identical to pancreatic SPN.
ConclusionThe tumor is presented because of its rarity, and our case is the second case with the longest follow-up period, treated with cystectomy, and the second case who gave birth after treatment.
Keywords
Introduction
Solid pseudopapillary neoplasm (SPN) is a rare neoplasm of the pancreas that occurs in 1-3% of all pancreatic tumors, with a low malignant potential, occurring predominantly in young women (about 90%). It was first recognized by Frantz in 1959.1 In general, the prognosis is good. Complete resection is curative in over 95% of patients.1 On the other hand, extrapancreatic cases of SPN are exceedingly rare. Extrapancreatic SPN can be seen in the ovary, omentum, mesocolon, peritoneum, gastroduodenal area and liver. In these cases, the tumor
mostly arises from ectopic pancreatic tissue.1 There are only 13 previous cases of primary ovarian SPN in the English literature.2,3,4,5,6,7,8,9,10,11,12 We report here, an additional case of ovarian SPN, which is morphologically and immunophenotypically similar to that of the pancreas, in the right ovary of a 30-year-old woman, with a review of the literature on extrapancreatic SPN.
Case Presentation
A 30-year-old female with abdominal discomfort was found to have a right ovarian cyst. No menstrual abnormalities were reported. Ultrasonographic evaluation showed a recent increase in the size of the cyst. Laboratory tests, CA125, CA19-9, AFP and CEA were within the normal range. Radiologically, our patient demonstrated no pancreatic lesion. MRI examination revealed that the uterus and left ovary were normal size and anatomy. A cyst of 51x41mm, which has a solid component of 4 mm was detected in the right ovary. Laparoscopic unilateral right cystectomy was performed. The left ovary was grossly normal. There was no evidence of intraabdominal disease. During a cesarean section which was performed 15 months after the laparoscopy, both ovaries were normal in size and shape. The cystectomy material measured 4.5x3x1 cm. The external surface was smooth. Cut surface and histologic evaluation were predominantly multilocular cystic with a minor solid component. The solid component was yellowish-white. There were no papillary areas grossly. Solid cellular nests, sheets and pseudopapillary architecture were identified
histologically. The pseudopapillae were composed of central fibrovascular cores. Nests were surrounded by thick fibrous septae. The neoplastic cells were cuboidal with abundant pale eosinophilic cytoplasm with uniform, round to oval nuclei with fine chromatin and single, small eccentrically placed nucleoli. Few intracellular and extracellular PAS-positive eosinophilic globules were seen focally (Figure1A-H). No nuclear grooves were identified. Mitoses, nuclear atypia, vascular and capsular invasion were not seen. No pancreatic tissue was seen within or adjacent to the tumor. Immunohistochemistry (IHC) revealed diffuse nuclear positivity for ß-catenin and diffuse cytoplasmic positivity for CD10, CD56, vimentin and Alpha 1-antitrypsin (Figure 2A-D). Pancytokeratin and progesterone receptor (PR) were focally positive (Figure 2E-F). Inhibin and WT-1 stains were negative (Figure 2H). Pancreatic and abdominal screening by CT scan / after the diagnosis of aSPN revealed no pancreatic and other intraabdominal lesions. With this finding, the case was confirmed to be a primary ovarian SPN. Clinicopathologic and immunohistochemical features of ovarian SPN cases, including ours are summarized in Tables 1-2. The patient gave birth to a healthy child 15 months after her initial diagnosis and had no recurrence in her follow-up of 105 months. Informed consent was obtained from the patient.
Ethics ApprovalNot required.
Reporting GuidelinesThis case is reported in accordance with the CARE guidelines.
Discussion
Solid pseudopapillary neoplasm (SPN) of the pancreas is an uncommon, usually benign neoplasm that constitutes approximately 1-3% of all exocrine pancreatic malignancies. It occurs predominantly in young women. SPN occurring as primary tumors outside the pancreas are exceedingly rare, constituting up to 1.01% to 1.8% of cases.1 Extrapancreatic SPN has been documented in other areas such as retroperitoneum, omentum, mesocolon, gastroduodenal area, colon and liver, which occur in ectopic pancreatic tissue.1 The most common extrapancreatic site is the ovary (totaly 14 cases, including the present case).2,3,4,5,6,7,8,9,10,11,12 Desphande et al first reported 3 cases located in the ovary in 2010.2 All cases of ovarian SPN have been reported to occur in the absence of ectopic pancreatic tissue.2,3,4,5,6,7,8,9,10,11,12 In the present case also, despite the whole sampling of the specimen, we did not find any ectopic pancreatic tissue within or adjacent to the tumor. The age of the patients ranged from 17 to 57, with a mean age of 35.5 years, and the median age of 25 in primary ovarian SPNs. Ovarian SPNs are located in the right ovary in 63.6% of the cases.2,3,4,5,6,7,8,9,10,11,12 The diameter of tumors ranged from 3 to 25.5 cm, in our case it was 4.5 cm. SPNs are often asymptomatic or are associated with uncharacteristic abdominal symptoms. Three patients presented with an abdominal mass2,7,11,12 and dysmenorrhea.12 Totaly nine cases, including ours, had abdominal pain or discomfort.2,3,5,6,8,10,12 One patient presented with weight loss, abdominal pain, bloating, adnexal mass, ascites and metastatic 2 masses in the right hepatic lobe, and this case had a malignant course.4 Three of the 12 cases underwent oophorectomy3,6,8 salpingo-oopherectomy was performed in six cases,2,5,7,11,12 bilateral salpingo-oopherectomy was performed in one of them2 total abdominal hysterectomy was performed in one of them,10 two of them underwent salpingo-oopherectomy, omentectomy, lymph node dissection and debulking.4,9 Our case underwent only cystectomy. Similar to the pancreatic SPN, extrapancreatic SPN can vary from entirely cystic with a small mural nodule to solid but most tumors are solid and cystic. Histologically, the tumor contains a mixture of solid, cystic, and pseudopapillary patterns in varying proportions. Characteristic morphologic features of these neoplasms include solid and pseudopapillary patterns, hyaline globules, clusters of uniform cells, and variable longitudinal nuclear grooves.1 SPN of the pancreas is a mysterious tumor, the cell of origin of which has not been fully elucidated yet. Immunohistochemically, SPN variably expresses epithelial, mesenchymal and endocrine markers. Neoplastic cells express nonspecific markers such as vimentin and CD10 diffusely. Epithelial differentiation of this tumor is incomplete with focal or weak expression of pancytokeratin (PCK). Its neuroendocrine differentiation is also unclear with the frequent expression of CD56 and neuron-specific (‘non-specific’) enolase (NSE), however, with the typical absence of chromogranin, the most specific endocrine marker. Alpha-1-antitrypsin (AAT) stains the PAS-positive globules.1 Including ovarian cases such as ours, extrapancreatic SPNs, demonstrate similar IHC profiles (except PCK) as their pancreatic counterparts. Most of the ovarian SPNs (7 cases) have been reported to be negative for PCK2,3,6,8,11,12 however, our case with its focal positivity for PCK, was similar to the remaining three cases4,5,7,10,11 and pancreatic SPNs.1 Several authors suggest that SPN may be related to hormonally sensitive tissue from the gonads. Firstly, this neoplasm usually occurs in young females and in addition, the neoplastic cells consistently express progesterone receptor (PR), suggesting a role for hormones in the evolution of these neoplasms.1 There is a close proximity of the genital ridges to the pancreas during embryogenesis, raising the possibility that cells from the primitive ovary may be incorporated into the embryonic pancreas. The diagnosis of SPN in the ovary may provide evidence to support this hypothesis in the pathogenesis of this neoplasm.2,3,4,5,6,7,8
Nearly all pancreatic SPNs have been reported to be positive for PR. In contrast, most cases of ovarian SPN are negative for PR,2,3,4,9,10 except three cases reported as diffusely positive.2,7,11 Stole and He et al. reported focal PR positivity similar to our case.5,8 Immunohistochemically, aberrant nuclear localization of ß-catenin is the result of mutations in exon 3 of this ß-catenin gene (CTNNB1), and this finding is observed in nearly all cases (90–100%) of pancreatic SPN and can provide strong support for the diagnosis of SPN. This mutation cancels glycogen synthase kinase 3-mediated degradation of this protein. Some studies showed the role of Wnt signaling, mostly associated with ß-catenin mutations in the tumorogenesis of SPN.1,6,10 Nuclear and cytoplasmic ß-catenin positivity has been reported in nine primary ovarian SPN.2,6,8,9,10,11 Nuclear ß-catenin positivity has been reported in four cases.2,3,4,5,6,7,12 Additionally, Kominami and Singh et al. have identified nuclear immunoreactivity for ß-catenin and mutations in exon 3 of CTNNB1.6,10 These results suggest that activated Wnt signaling, which was primarily due to mutations in exon 3 of CTNNB1, plays an important role in the tumorgenesis of both ovarian and pancreatic SPN.6,10 Although uniform cells and common positivity for CD56 and NSE in SPN may mimic a neuroendocrine tumor (NET) (but without “salt and pepper type” chromatin and insular and trabecular patterns), unlike NET, chromogranin is typically negative in SPN. Furthermore, in contrast to NET, SPN uniformly lack cytoplasmic membrane staining for E-cadherin.1,12 The presence of solid growth patterns and tumor cells exhibiting grooves and nuclear membrane irregularity can mimic the diffuse pattern of adult granulosa cell tumors (GCT). GCT and Sertoli cell tumors (SCT) can rarely exhibit a pseudopapillary pattern. On the other hand,
the predominance of solid growth and cells along with vacuolated pale and eosinophilic cytoplasm are features that SCT of the ovary. However, ovarian SPN lacked the typical architectural patterns, such as microfollicular, insular, and gyriform, that are seen in GCT. Lack of immunoreactivity for calretinin and inhibin also distinguishes these neoplasms from GCT and SCT of the ovary.2,3,5,12 SPNs of the pancreas are usually benign or indolent tumors with less than 5% displaying aggressive behavior.1 Complete surgical excision is curative also in extrapancreatic cases. In extrapancreatic SPNs, metastasis has been reported only in two cases located in the ovary.4,9 One of the presented cases with malignant morphological features and metastasis had a fatal behavior.4 Another case has been reported with metastasis in the omentum, parametria, and pelvic lymph nodes, who lived for 1.5 years of follow-up.9 The histopathology and immunohistochemistry of all primary ovarian SPNs in all the cases including ours, closely resembled their pancreatic counterparts. Radiological studies showed an unremarkable pancreas in all ovarian SPNs, including our case.2,11
He et al. reported that 3 months postoperatively, a cystic shadow in the right ovary was detected by ultrasonography, but no evidence of any recurrence was found during a follow-up of 3 years .8 Three of the reported cases have no prognostic information.2,6 There was no evidence of disease in these seven cases, which were followed from 3 months to 12 years.2,3,5,7,8,9,10,11,12
In our case, there were no morphologic signs of malignant behavior such as mitosis, atypia, or vascular and capsular invasion. After the pathological diagnosis, meticulous abdominopelvic evaluation of the patient (with special regard to the pancreatic region) revealed no evidence of any other tumor, and the tumor in our case was diagnosed as primary ovarian SPN. Our case is the second case with the longest follow-up period, after the 144-month follow-up case reported by Cheuk et al.8 In her follow-up of 105 months, she gave birth (like the patient in the literature 12 (Nguyen MT at al.)) to a healthy child 15 months after her initial diagnosis and did not have any recurrence.
Limitations
This study is limited by its single-case design.
Conclusion
We report the 14th case of primary SPN of the ovary with follow-up. These neoplasms are histologically and immunohistochemically similar to their pancreatic counterparts. This rare ovarian neoplasm with a solid and pseudopapillary appearance should be considered in the differential diagnosis of ovarian masses, and immunohistological staining should be performed for accurate diagnosis. Positive nuclear staining with ß-catenin supports the diagnosis of an SPN. It should be kept in mind that metastases of the pancreatic SPNs to the ovaries can also occur. The presence of a primary pancreatic SPN should be excluded with radiological studies, before the diagnosis of a primary ovarian SPN.
Declarations
Ethics Declarations
The authors declare that all procedures performed in this study were conducted in accordance with institutional, national, and international ethical standards.
Animal and Human Rights Statement
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the Declaration of Helsinki and its later amendments.
Informed Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Conflict of Interest
The authors declare no conflict of interest.
Funding
None.
Author Contributions (CRediT Taxonomy)
Conceptualization: N.B.
Methodology: N.B., İ.T.
Investigation: N.B., İ.T.
Data curation: N.B.
Formal analysis: N.B.
Writing - original draft: N.B.
Writing - review & editing: F.B., G.B.D., S.T.
Supervision: S.T.
Scientific Responsibility Statement
The authors declare that they are responsible for the scientific content of the article, including study design, data collection, analysis and interpretation, manuscript preparation, and approval of the final version of the manuscript.
Abbreviations
AAT: alpha-1-antitrypsin
AFP: alpha-fetoprotein
CA125: cancer antigen 125
CA19-9: carbohydrate antigen 19-9
CEA: carcinoembryonic antigen
CT: computed tomography
GCT: granulosa cell tumor
IHC: immunohistochemistry
MRI: magnetic resonance imaging
NET: neuroendocrine tumor
NSE: neuron-specific enolase
PCK: pancytokeratin
PR: progesterone receptor
SCT: Sertoli cell tumor
SPN: solid pseudopapillary neoplasm
References
-
Bosman FT, Carneiro F, Hruban RH, Theise ND, eds. WHO classification of tumours of the digestive system. 4th ed. Lyon: International Agency for Research on Cancer; 2010:327-330.
-
Deshpande V, Oliva E, Young RH. Solid pseudopapillary neoplasm of the ovary: a report of 3 primary ovarian tumors resembling those of the pancreas. Am J Surg Pathol. 2010;34(10):1514-1520. doi:10.1097/pas.0b013e3181f133e9
-
Cheuk W, Beavon I, Chui DT, Chan JK. Extrapancreatic solid pseudopapillary neoplasm: report of a case of primary ovarian origin and review of the literature. Int J Gynecol Pathol. 2011;30(6):539-543. doi:10.1097/pgp.0b013e31821724fb
-
Syriac S, Kesterson J, Izevbaye I, de Mesy Bentley KL, Lele S, Mhawech-Fauceglia P. Clinically aggressive primary solid pseudopapillary tumor of the ovary in a 45-year-old woman. Ann Diagn Pathol. 2012;16(6):498-503. doi:10.1016/j.anndiagpath.2011.04.007
-
Stoll LM, Parvataneni R, Johnson MW, Gui D, Dorigo O, Sullivan P. Solid pseudopapillary neoplasm, pancreas type, presenting as a primary ovarian neoplasm. Hum Pathol. 2012;43(8):1339-1343. doi:10.1016/j.humpath.2011.12.018
-
Kominami A, Fujino M, Murakami H, Ito M. β-catenin mutation in ovarian solid pseudopapillary neoplasm. Pathol Int. 2014;64(9):460-464. doi:10.1111/pin.12194
-
Chen Q, Lu W, Lv W. Overlap of microcystic stromal tumor and primary solid pseudopapillary neoplasm of the ovary. Int J Clin Exp Pathol. 2015;8(9):11792-11797.
-
He S, Yang X, Zhou P, Cheng Y, Sun Q. Solid pseudopapillary tumor: an invasive case report of primary ovarian origin and review of the literature. Int J Clin Exp Pathol. 2015;8(7):8645-8649.
-
Gahlot GP, Mridha AR, Sable M, Sharma MC, Pramanik R, Kumar L. Solid pseudopapillary neoplasm of the ovary with metastases to the omentum and regional lymph nodes. Indian J Pathol Microbiol. 2016;59(3):348-350. doi:10.4103/0377-4929.188107
-
Singh K, Patel N, Patil P, Paquette C, Mathews CA, Lawrence WD. Primary ovarian solid pseudopapillary neoplasm with CTNNB1 c.98C>G (p.S33C) point mutation. Int J Gynecol Pathol. 2018;37(2):110-116. doi:10.1097/pgp.0000000000000396
-
Komforti MK, Edelman M, Fan C, Liang SX. Solid pseudopapillary neoplasm presenting as a primary ovarian mass in an eighteen-year-old female: report of a case and review of the literature. Virchows Arch. 2018;472(2):285-291. doi:10.1007/s00428-017-2231-y
-
Nguyen MT, Carter M, Zhao Z, Abidi A, Hodeib M. Ovarian solid pseudopapillary tumor resembling benign hemorrhagic cyst on rapid frozen section. Case Rep Obstet Gynecol. 2020:1-4. doi:10.1155/2020/6473630
Figures
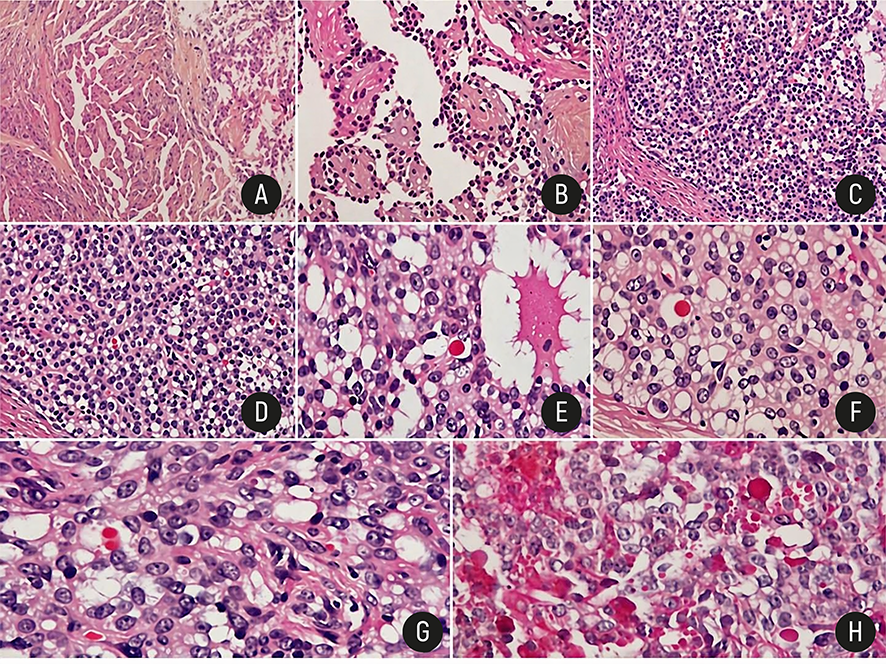
Figure 1. Low-power view shows a solid and pseudopapillary pattern HE x4 (a); pseudopapillary pattern HE x20(b); nests of tumor cells surrounded by thick fibrous septa HE x10 (c); scattered eosinophilic globules in solid area HE x20 (d); microcysts filled with colloid-like material HE x40 (e); uniform tumor cells and scattered eosinophilic globules HE x40 (f,g) and PAS-positive eosinophilic globules x40 (h)
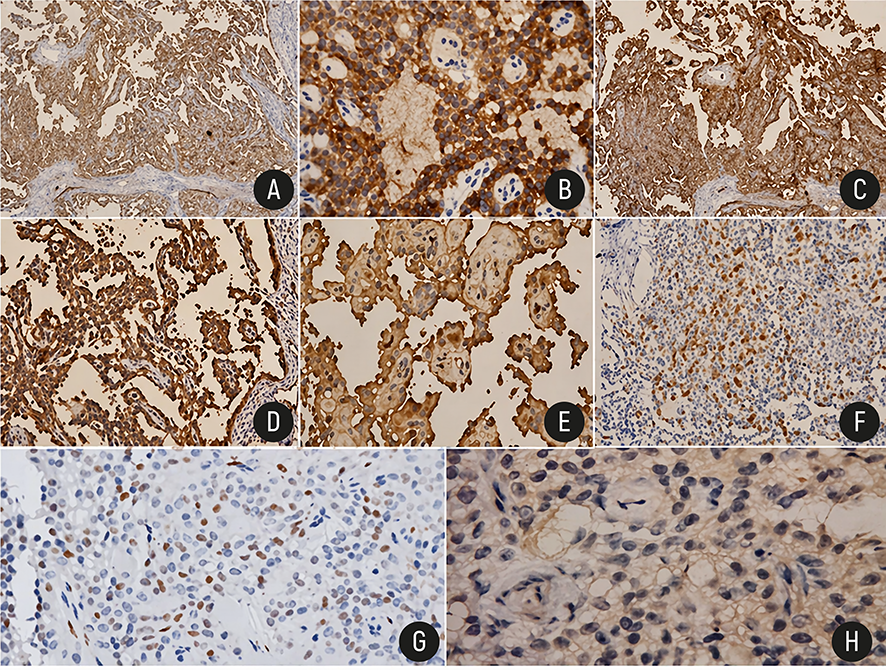
Figure 2. Abnormal nuclear b-catenin immunostaining x20 (a); diffuse cytoplasmic expression of CD10 x20 (b), CD56x4 (c), vimentin x10 (d) and trypsin x20 (e); focal cytoplasmic expression of pancytokeratin x10 (f) and progesterone x40 (g); negativity of inhibin x40 (h).
Tables
Table 1. Clinicopathologic features of reported cases of ovarian solid pseudopapillary neoplasm
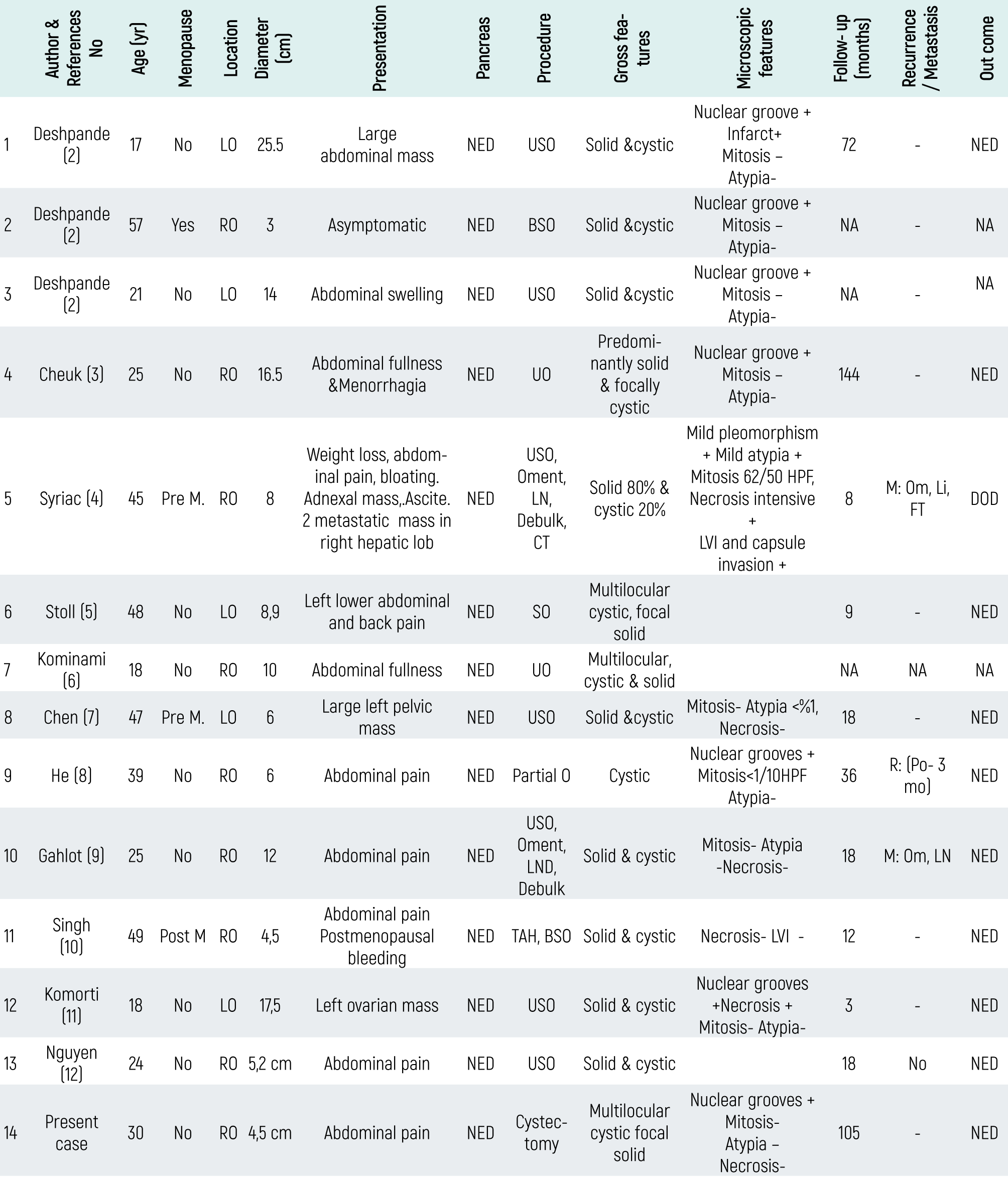
NED: No evidence of disease, NA: Not Available; Pre M: Premenopausal; Post M: Postmenopausal; LVI: lymphovascular invasion; LO: Left Ovary, RO: Right Ovary; O: oopherectomy, USO: Unilateral Salpingo-oopherectomy, BSO: Bilateral Salpingo-oopherectomy, TAH: Total Abdominal Hysterectomy, Oment: Omentectomy, LND: Lymph Node Dissection, Debulk: Debulking, CT: Chemotherapy, DOD: Died of disease; M: Metastasis, Om: Omentum, Li: Liver FT: Fallopian tube, LN: Lymph nodes; R: Recurrence, Po: Postop.
Table 2. Immunohistochemical features of reported cases of ovarian solid pseudopapillary neoplasm
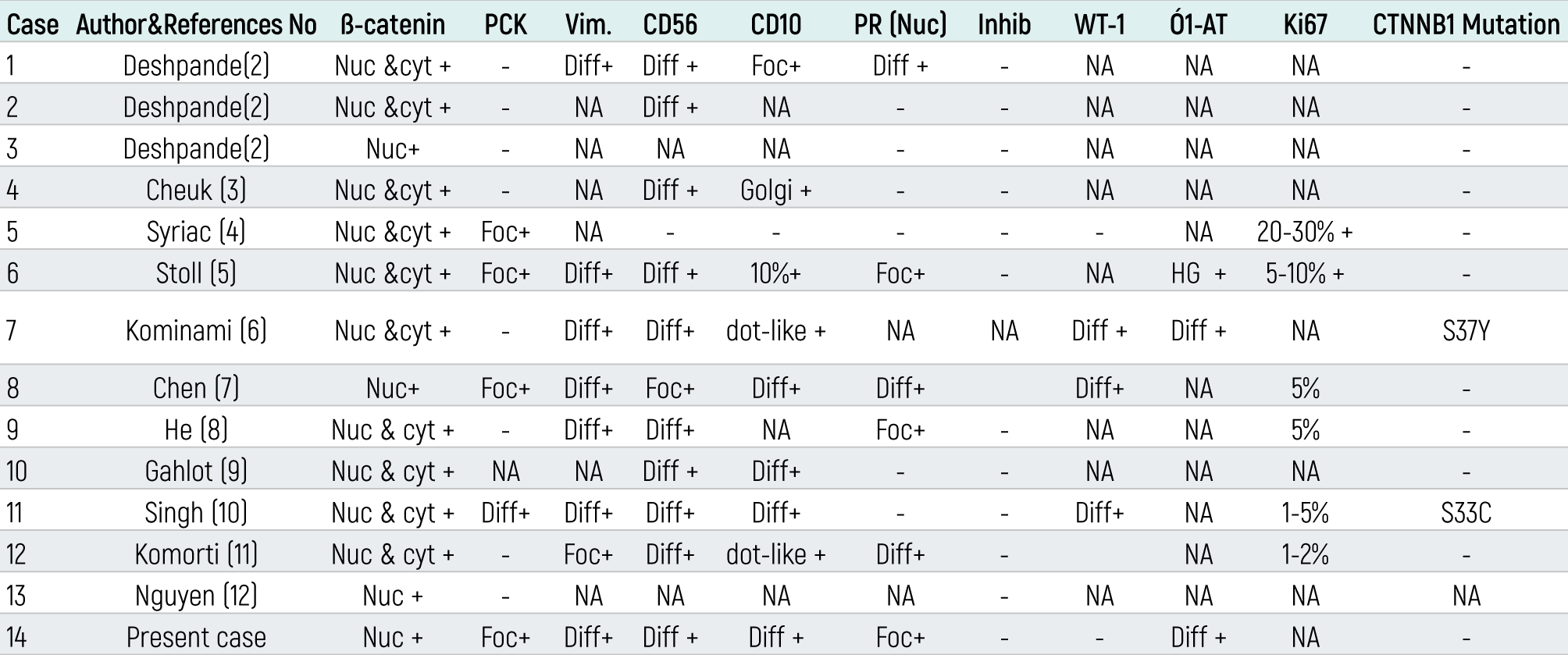
Nuc: Nuclear, Cyt: Cytoplasmic, Diff: Diffuse, Foc: Focal, NA: Not Available, PR: Progesterone Receptor, PCK: Pancytokeratine, Ó1-AT:Alpha 1-antitrypsin, Vim: Vimentine, Inhib: Inhibine, HG: Hyaline globular
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Nuray Bassullu, İlknur Turkmen, Faruk Buyru, Gulen Bulbul Dogusoy, Sitki Tuzlali. Primary solid pseudopapillary neoplasm of the ovary: A Case Report and Literature Review. Eu Clin Anal Med 2023;11(2):26-29. doi:10.4328/ECAM.10047
- Received:
- December 27, 2019
- Accepted:
- April 19, 2023
- Published Online:
- April 30, 2023
- Printed:
- May 1, 2023