Complementary and alternative medicine practices used by families inasthmatic children
Complementary and alternative medicine
Authors
Abstract
AimIn this study, we aimed to examine the use of complementary and alternative medicine (CAM) in children with asthma.
MethodsThis is a descriptive type of study. The study included all patients aged 2-17 years who visited to the Pediatric Allergy and Immunology Department of a tertiary hospital in Istanbul between May and July 2022 with asthma diagnosis. Age, duration of asthma diagnosis, use of complementary and alternative therapies of the patients were asked.
ResultsPediatric patients (n=115) with asthma were evaluated. All families used at least one CAM. Of the children, 72.2% (n=83) used multiple CAM product. While the percentage of those who used one of the CAM products was 27.8% (n=32), 6.1% (n=7) of the families used five different CAMs. The most frequently used CAM was honey with a percentage of 67.0% (n=77). Honey was followed by carob molasses (n=29, 25.2%), ginger (n=29, 25.2%), black seed oil (n=20, 17.4%) and lemon (n=20, 17.4%). Only three (2.6%) parents stated that they had heard about CAM from their doctor. The duration of asthma diagnosis was statistically significantly longer in children using multiple products (p=0.017).
ConclusionIn our study, the percentage of multiple CAM products usage among children with asthma was high. However, very few parents have used CAM on doctor’s advice. Further studies on the reasons for CAM use, CAM side effects and benefits should be planned.
Keywords
Introduction
Asthma is a major public health problem worldwide.1 It is a respiratory disease characterized by chronic inflammation of the airways.2 Chronic airway inflammation and hyperresponsiveness lead to episodes of wheezing, shortness of breath, chest tightness and/or coughing, especially in the middle of the night or early morning. Symptoms and airflow limitation often resolve with treatment or spontaneously.3 Asthma is one of the most common chronic diseases in children.4 It constitutes a significant burden of disease for the patient and the community.5 It can cause a decrease in quality of life, mental disorders such as anxiety and depression, and school loss in children.6,7,8 Despite all this, asthma can be controlled with appropriate treatment.3
Pharmacotherapies used in the treatment of asthma are generally effective and well- tolerated in the management of the disease and control of attacks.9 Despite this, some asthma patients use complementary and alternative therapies.10 Complementary treatments aim to support medical treatments. Patients mostly prefer to use them to improve well-being, to reduce disease symptoms and use of medications.11,12 Patients who did not want to use complementary and alternative medicine reported focusing on the treatment recommended by the doctor as the most common reason for not using it.13
A study reported that 76,4% of the children with asthma had ever used complementary and alternative medicine (CAM).11 The use of CAM methods in asthma patients has been reported to be high.14,15 It is essential that healthcare professionals have sufficient knowledge about such a widely used method.10,16 In this study, we aimed to examine the CAM use in children with asthma admitted to our clinic and to evaluate variables such as age and duration of asthma diagnosis that may be associated with CAM use.
Materials and Methods
This is a prospectively designed, descriptive type of study. The study included all patients aged 2-17 years who presented to the Pediatric Allergy and Immunology Department of a tertiary hospital in Istanbul between May 2022 and July 2022 with asthma diagnosis and used CAM. Asthma was diagnosed by clinical and laboratory methods in patients with recurrent wheezing and cough with improvement between attacks. Parents were asked questions about age, duration of asthma diagnosis, hometown, use of complementary and alternative therapies of the patients. Children who did not use CAM were excluded. Statistical AnalysisSPSS (Statistical Package for Social Sciences) for Windows 25.0 program was used for statistical analysis and data recording. Median, minimum and maximum values, number (n) and percentages (%) were used for descriptive data. The conformity of continuous variables to normal distribution was examined with histograms and probability plots and with the Kolmogorov-Smirnov/Shapiro-Wilk tests. The Mann Whitney U test was used to compare continuous variables that did not conform to normal distribution. P<0.05 was accepted as the level of statistical significance.
EthicsEthical approval was obtained from the Ethics Committee of the relevant hospital on 10.02.2022 with decision number 41.
Statistical AnalysisSPSS (Statistical Package for Social Sciences) for Windows 25.0 program was used for statistical analysis and data recording. Median, minimum and maximum values, number (n) and percentages (%) were used for descriptive data. The conformity of continuous variables to normal distribution was examined with histograms and probability plots and with the Kolmogorov-Smirnov/Shapiro-Wilk tests. The MannWhitney U test was used to compare continuous variables that did not conform to normal distribution. P<0.05 was accepted as the level of statistical significance.
Results
In our study, 115 pediatric patients with asthma were evaluated. Of the children, 52.2% (n=60) were male, 47.8% (n=55) were female. The median age of the children was 6.0 years (2.0-17.0). The median duration of asthma diagnosis was 4.0 years (1.0-16.0). The most common hometown of the children was Blacksea (n=40, 34.8%) (Table 1).In our study, parents were asked about their children’s use of CAM via a questionnaire. All families used at least one CAM. The percentage of those who used one of the CAM products was 27.8% (n=32), 25.2% (n=29) used two different types of CAM, and 27.8% (n=32) used three types. While 13.0% (n=15) of the families used four types of CAM, 6.1% (n=7) of the families used five different CAMs (Figure 1).
The most frequently used CAM was honey with a percentage of 67.0% (n=77). Honey was followed by carob molasses (n=29, 25.2%), ginger (n=29, 25.2%), black seed oil (n=20, 17.4%) and lemon (n=20, 17.4%). The percentages of CAM use are shown in Table 2.
Parents were asked where they obtained information about CAM products and their use. Parents mostly heard about these products from social media (n=59, 51.3%) or from their ancestors (n=46, 40.0%). While 6.1% (n=7) of the parents heard about CAM from their social environment, three (2.6%) parents stated that they heard about CAM from their doctor.
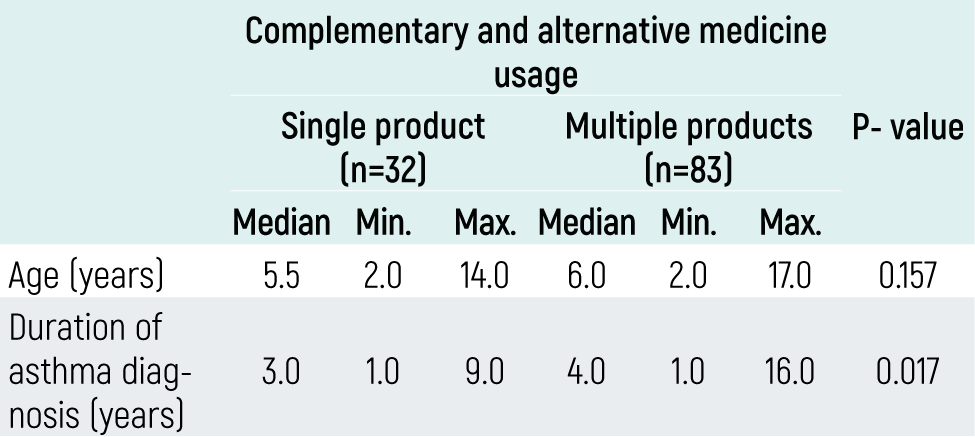
The study evaluated children’s age and duration of asthma diagnosis, which may be associated with single and multiple CAM product use. Of the children, 72.2% (n=83) used multiple CAM products. The median age of children using multiple products was 6.0 years (2.0-17.0), while the median age of children using a single product was 5.5 years (2.0-14.0) (p=0.157). The median duration of asthma diagnosis in children who used multiple products was 4.0 years (1.0-16.0), while the duration of asthma diagnosis in single product users was 3.0 years (1.0-9.0). The duration of asthma diagnosis was statistically significantly longer in children using multiple products (p=0.017) (Table 3).
Discussion
Today, the prevalence of asthma in children is increasing.17,18 Since asthma is a significant disease burden for both children and parents, it is important to treat and clinically control the disease. For this reason, parents may turn to complementary and alternative therapies instead of or in addition to pharmacologic treatments.10
In our study, parents were questioned about CAM use in their children. All families used at least one CAM. The percentage of those who used only one of the CAM products was 27.8% (n=32), whereas 72.2% (n=83) of the children used multiple CAM products. In a large sample study in the literature, 57.0% of asthma patients used CAM.19 In different studies conducted in our country, this percentage was reported as 77.0% and 66.0%, respectively.9,10 According to the literature, CAM use in asthma patients is high and according to our study, almost 3 out of 4 asthmatic children use multiple CAMs. It is necessary to know what products are in such widespread use in order to manage the disease and to be careful for possible side effects.
The most frequently used CAM was honey with a percentage of 67.0%. Honey was followed by carob molasses, ginger, black seed oil and lemon. Similar to our study, honey was the most common CAM product used in children with asthma in one of the studies in Türkiye.10 Molasses types and black seed oil were the other products used respectively. Similarly, honey and molasses were the most commonly used CAM products in different studies conducted in our country.9,20 The results of our study are consistent with the literature on CAM use in asthma. Although some CAM therapies have been used in asthma for many years, studies on the safety, concurrent use with pharmacologic treatments, benefits and harms of these products are needed.In our study, nearly half of the parents heard about CAM from social media. A big proportion of them (40.0%) received information about CAM from their ancestors. While 6.1% of the parents heard about CAM from their social environment, 2.6% of the parents stated that they heard about CAM from their doctor. In a study the parents of asthmatic children learned about CAM mostly through friends and relatives.21 Similar to our results, only 6% learned about it from physicians. Since the study was conducted in 2003, the concept of social media was not developed at that time. According to the results of our study, in the context of the modern development of social media networks, the sources of information for parents about CAM are largely shaped by social media. Studies can be planned to control the informative posts on social media and to prevent misinformation if exists.
In our study, the age of the child and the duration of asthma diagnosis, which we thought might be associated with multiple CAM use, were evaluated. The duration of asthma diagnosis was statistically significantly longer in children using multiple products. This result can be interpreted as a search by families for different therapeutic methods in the later stages of the disease. Further qualitative and quantitative studies are needed to investigate other reasons that lead families to use CAM. In literature, there are studies reporting the high use of CAM methods in childhood diseases in low-income families and countries.16,22 Economic status, education level, severity of the disease have also been reported to have an impact on CAM use.23 In our study, data on income and educational status could not be presented. Future studies need to evaluate parameters such as income status and disease severity.
Limitations
Limitations and Strengths: Although the fact that our study was conducted in a single center creates a limitation in terms of the generalizability of the results, since it was conducted with patients admitted to a tertiary care hospital, participants could be recruited from different regions of the country. Another limitation of our study is that other factors such as socioeconomic level, education level and occupation that may affect parents’ CAM use were not questioned. Nevertheless, since few studies have been conducted in this field, our study has made an important contribution to the literature in this field with single and multiple CAM use and the factors affecting it.
Conclusion
In our study, the percentage of multiple CAM products usage among children with asthma was high. Parents mostly heard about these products from social media and from their ancestors. However, very few parents have used it on doctor’s advice. The most frequently used CAM was honey. Honey was followed by carob molasses, ginger, black seed oil and lemon. Further studies asking the reasons for CAM use, CAM side effects and benefits should be planned.
Declarations
Animal and Human Rights Statement
All procedures performed in this study involving human participants were conducted in accordance with the ethical standards of the institutional and/or national research committee and with the Declaration of Helsinki and its later amendments or comparable ethical standards.
Informed Consent
Written informed consent was obtained from the parents of the participants.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Conflict of Interest
The authors declare that they have no conflict of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the scientific content of the article, including study design, data collection, analysis and interpretation, manuscript preparation, and approval of the final version of the manuscript.
Abbreviations
CAM: Complementary and Alternative Medicine
SPSS: Statistical Package for the Social Sciences
References
-
Trikamjee T, Comberiati P, Peter J. Pediatric asthma in developing countries: challenges and future directions. Curr Opin Allergy Clin Immunol. 2022;22(2):80-85. doi:10.1097/aci.0000000000000806
-
Mims JW. Asthma: definitions and pathophysiology. Int Forum Allergy Rhinol. 2015;5(Suppl 1):S2-S6. doi:10.1002/alr.21609
-
Asher MI, Rutter CE, Bissell K, et al. Worldwide trends in the burden of asthma symptoms in school-aged children: Global Asthma Network Phase I cross-sectional study. Lancet. 2021;398(10311):1569-1580. doi:10.1016/s0140-6736(21)01450-1
-
Jones H, Lawton A, Gupta A. Asthma attacks in children: challenges and opportunities. Indian J Pediatr. 2022;89(4):373-377. doi:10.1007/s12098-021-04069-w
-
Croisant S. Epidemiology of asthma: prevalence and burden of disease. Adv Exp Med Biol. 2014;795:17-29. doi:10.1007/978-1-4614-8603-9_2
-
Gaffin JM, Castro M, Bacharier LB, Fuhlbrigge AL. The role of comorbidities in difficult-to-control asthma in adults and children. J Allergy Clin Immunol Pract. 2022;10(2):397-408. doi:10.1016/j.jaip.2021.11.016
-
Sullivan P, Ghushchyan V, Navaratnam P, et al. The national burden of poorly controlled asthma, school absence and parental work loss among school-aged children in the United States. J Asthma. 2018;55(6):659-667. doi:10.1080/02770903.2017.1350972
-
Khdour M, Abu Ghayyadeh M, Al-Hamed D, et al. Assessment of quality of life in asthmatic children and adolescents: a cross-sectional study in West Bank, Palestine. PLoS One. 2022;17(6):e0270680. doi:10.1371/journal.pone.0270680
-
Babayiğit AH. High usage of complementary and alternative medicine among Turkish asthmatic children. Iran J Allergy Asthma Immunol. 2015;14(4):410-415.
-
Özkars MY, Kırık S. Use of complementary and alternative therapy in children with asthma: alternative therapy in asthma. Ortadogu Tip Derg. 2018;10(4):403-406. doi:10.21601/ortadogutipdergisi.378723
-
Kalaci O, Giangioppo S, Leung G, et al. Complementary and alternative medicine use in children with asthma. Complement Ther Clin Pract. 2019;35:272-277. doi:10.1016/j.ctcp.2019.02.017
-
Barnes LAJ, Rolfe MI, Barclay L, et al. Women’s reasons for taking complementary medicine products in pregnancy and lactation: results from a national Australian survey. Complement Ther Clin Pract. 2022;49:101673. doi:10.1016/j.ctcp.2022.101673
-
Yeom J, Lee JM. Use of complementary and alternative medicine (CAM) in patients with colorectal cancer. Clin Nutr Res. 2022;11(4):255-263. doi:10.7762/cnr.2022.11.4.255
-
Tuncel T, Çetemen A, Karabel M, et al. Complementary and alternative medicine in children with asthma and/or allergic rhinitis. Asthma Allergy Immunol. 2014;12(3):146-151.
-
George M, Topaz M. A systematic review of complementary and alternative medicine for asthma self-management. Nurs Clin North Am. 2013;48(1):53-149. doi:10.1016/j.cnur.2012.11.002
-
Diorio C, Lam CG, Ladas EJ, et al. Global use of traditional and complementary medicine in childhood cancer: a systematic review. J Glob Oncol. 2017;3(6):791-800. doi:10.1200/jgo.2016.005587
-
Triasih R, Setyowireni D, Nurani N, Setyati A. Prevalence, management, and risk factors of asthma among school-age children in Yogyakarta, Indonesia. J Asthma Allergy. 2023;16:23-32. doi:10.2147/jaa.s392733
-
Ren J, Xu J, Zhang P, Bao Y. Prevalence and risk factors of asthma in preschool children in Shanghai, China: a cross-sectional study. Front Pediatr. 2022;9:793452. doi:10.3389/fped.2021.793452
-
Huang TP, Liu PH, Lien AS, et al. Characteristics of traditional Chinese medicine use in children with asthma: a nationwide population-based study. Allergy. 2013;68(12):1610-1613. doi:10.1111/all.12273
-
Işık S, Gül İ, Çetin M. Van ilinde astım ve/veya allerjik rinitli çocuklarda tamamlayıcı ve alternatif tıp uygulamaları [Complementary and alternative medicine practices in children with asthma and/or allergic rhinitis in Van]. Turk J Pediatr Dis. 2018;12(2):131-135. doi:10.12956/tjpd.2017.311
-
Orhan F, Sekerel BE, Kocabas CN, et al. Complementary and alternative medicine in children with asthma. Ann Allergy Asthma Immunol. 2003;90(6):611-615. doi:10.1016/s1081-1206(10)61864-9
-
Richmond E, Adams D, Dagenais S, et al. Complementary and alternative medicine: a survey of its use in children with chronic respiratory illness. Can J Respir Ther. 2014;50(1):27-32.
-
Yildiz Y, Yavuz AY. Complementary and alternative medicine use in children with asthma. Complement Ther Clin Pract. 2021;43:101353. doi:10.1016/j.ctcp.2021.101353
Figures
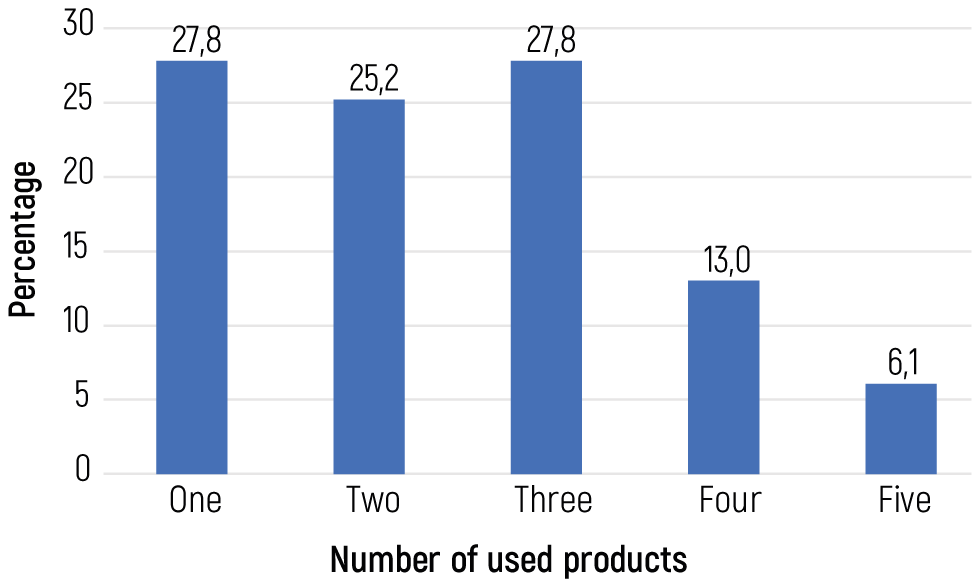
Figure 1. Numbers of different complementary and alternative medicine usage
Tables
Table 1. Characteristics of the patients
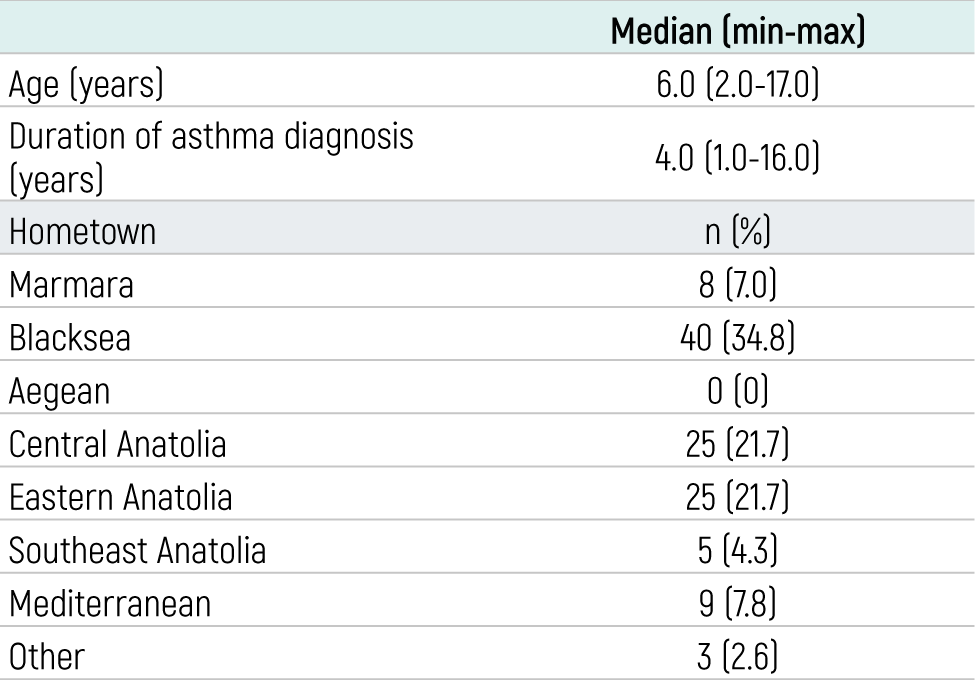
Table 2. Use of different types of complementary and alternative medicine products
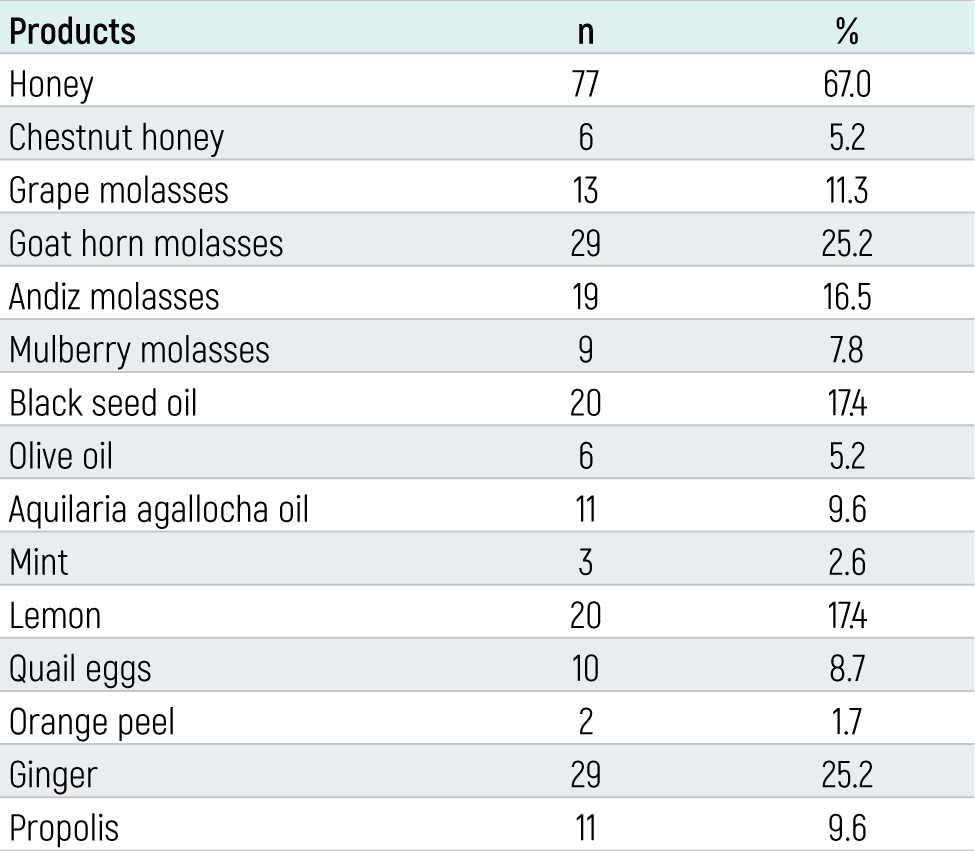
Table 3. Age, duration of asthma diagnosis and complementary and alternative medicine usage
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Uğur Altaş, Muhammed Esad Sıddık Özkars, Zeynep Meva Altaş, Neslihan Sağlam, Mehmet Yaşar Özkars. Complementary and alternative medicine practices used by families inasthmatic children. Eu Clin Anal Med 2023;11(3):51-54. doi:10.4328/ECAM.10055
- Received:
- August 14, 2023
- Accepted:
- August 30, 2023
- Published Online:
- August 30, 2023
- Printed:
- September 1, 2023