Opinions and knowledge level of pediatricians on circumcision
Pediatricians’ views on circumcision
Authors
Abstract
AimThis study aimed to assess the knowledge level and opinions of pediatricians about circumcision and the preputium and discuss them in light of the existing literature.
MethodsThis descriptive field study, employing a mixed design, was conducted among pediatricians (n = 292). The questionnaire form was prepared by the researchers based on the existing literature. The questionnaire forms were distributed via WhatsApp, Messenger, and SMS. Analysis of variance was used to examine knowledge levels in groups of three stages and above. A chi-square test was used to compare proportionate data, and a p-value of <0.05 was considered statistically significant.
ResultsAmong the study participants, 92.2% stated that they recommended circumcision in cases of phimosis, while 88.9% did so for recurrent urinary tract infections. Additionally, 98.3% acknowledged hypospadias awareness, 64.4% stated that they considered circumcision a part of their cultural/religious identity, and 28.1% expressed the belief that circumcision should be avoided in patients with bleeding disorders unless medically warranted. It was observed that 33.2% of the participants endorsed circumcision between the ages of 6–10 years, 74.4% recommended it be performed by pediatric surgeons, and 96.6% suggested its execution in a hospital setting. The average knowledge level of the participants was found to be 47.95 ± 19.84 points out of 100.
ConclusionResults revealed that pediatricians who participated in our study believed that there should be no legislation limiting circumcision and that circumcision should preferably be performed by pediatric surgeons in a hospital setting, in the presence of an anesthesiologist, and with the option of sedation or local anesthesia. Furthermore, the participants’ knowledge level indicates a potential need for training on circumcision and the preputium.
Keywords
Introduction
Circumcision involves the surgical removal of the penile skin (preputium), which covers the glans penis, thereby revealing some or all of the glans penis. The worldwide prevalence of circumcision, which is a universal practice for religious reasons in Muslim and Jewish societies as well as in certain regions of Asia and Africa, is approximately 37.7%.1 In Türkiye, where the majority of the population is Muslim and ritual circumcision is customary among nearly all men, parents often seek guidance and information from pediatricians regarding circumcision during their children’s health check-ups. Therefore, the knowledge level and opinions of pediatricians are crucial in providing parents with counseling and guidance. The present study aimed to assess the knowledge level and opinions of pediatricians on circumcision and the preputium and discuss them within the framework of the existing literature.
Materials and Methods
The study was approved by the Local Ethics Committee dated April 24, 2023 (number B.10.1.TKH.4.34.H.GP.0.01/145). The study was planned under the Helsinki Principles.
DesignThis descriptive field study, designed with a mixed-method approach, was conducted between May 1 and May 30, 2023.
Participants and ProcedureWithin the scope of the study, 1,500 pediatricians and pediatric subspecialists were identified in the Istanbul region based on the data provided by the Ministry of Health for the year 2023. A minimum of 288 physicians were calculated to achieve population representativeness, maintaining an acceptable margin of error of 5% and a confidence level of 90%. The study was conducted on 292 valid data points. A total of 652 pediatricians received the form via WhatsApp, Messenger, and SMS. The introductory page of the questionnaire, which can be accessed through the provided link, explicitly communicated that proceeding with the questionnaire’s completion would imply the participant’s consent. Out of the distributed questionnaires, 292 were completed.
InstrumentationThe questionnaire included 30 questions created using the Google Forms web tool to collect data on the sociodemographic characteristics of pediatricians as well as evaluate their knowledge level and opinions about circumcision and the preputium. Items 22–30, which were designed based on the existing literature, were developed to measure the knowledge level of the participants about circumcision and the preputium. In the knowledge-based test comprising nine questions, participants received 1 point for correct responses and 0 points for incorrect responses. Statements 29 and 30 of the scale have two correct options. Participants received 2 points for selecting both correct responses and 1 point for selecting a single correct response. The KR-1 reliability level of the scale, which was evaluated over 11 statements in total, was found to be 0.79, and this test was found to be a consistent measurement tool for measuring the knowledge level. Furthermore, to facilitate analysis, the knowledge levels were transformed into a 100-point scale.
Data AnalysisDescriptive statistics included the mean ± standard deviation for continuous variables, while percentage and frequency were used to present discrete variables. The normality of the data distribution was examined through the Kolmogorov–Smirnov test. The independent sample t-test was used for comparisons between paired groups. Fisher’s Exact chi-square test was used to compare qualitative data, and a p-value of <0.05 was considered statistically significant. Analysis of variance in groups of three stages and above in the examination of knowledge levels was conducted. A chi-square test was used to compare proportionate data. The KR-21 test was conducted to determine the reliability levels of the knowledge-based statements. The relationship between the measurements was evaluated using Pearson’s correlation coefficient. In the study, a p-value of <0.05 was considered the critical decision-making threshold. The data were analyzed on a computer using the SPSS 25.0 program.
Ethical ApprovalThis study was approved by the Local Ethics Committee of Health Sciences University Umraniye Training and Research Hospital (Date: 2023-04-24, No: B.10.1.TKH.4.34.H.GP.0.01/145)
Results
A total of 292 pediatricians (173 general pediatricians and 119 pediatric subspecialists) participated in the study by completing the questionnaire in May 2023. Of the participants, 220 were female, 72 were male, 113 were aged 25–35 years, 122 were aged 35–45 years, and 57 were aged >45 years. Of the participants, 243 were working in organizations affiliated to the Ministry of Health and 49 in private organizations; 39 had less than 5 years of professional experience, 76 had 5–10 years of professional experience, 83 had 10–15 years of professional experience, and 94 had >15 years of professional experience. Among the 152 participants who did not have a male child, 89.5% indicated their intention to choose circumcision for their potential or existing male child. Similarly, among the 140 participants who were parents of a male child, 94.3% stated that they had opted for or would choose circumcision for their sons. According to the results of the difference analysis, no statistically significant difference was observed between the groups with and without male children regarding the opinion about the circumcision of their own children (Fischer’s Exact Test, p = 0.099). Table 1 shows the participants’ opinions on age, setting, practitioner, and anesthesia method recommended for circumcision (Table 2). The proportions of respondents recommending circumcision for certain penile and urinary system diseases are as follows: physiological phimosis (n: 42) 14.5%, pathological phimosis (n: 269) 92.2%, paraphimosis (n: 158) 54.1%, recurrent balanitis (n: 220) 75.5%, hypospadias/epispadias (n: 173) 59.3%, balanitis xerotica obliterans (n: 155) 53.1%, at the time of initial diagnosis of urinary tract infection (n: 30) 10.3%, recurrent urinary tract infection (n: 260) 88.9%, congenital hydronephrosis (n: 135) 46.2%, vesicoureteral reflux (n: 158) 54.1%, nonorganic enuresis (n: 45) 15.5%, and in all congenital urinary tract anomalies (n: 140) 47.9%. Of the participants, 90.3%, 98.3%, 93.8%, 40%, and 34.1% stated that they could visually recognize the buried penis, hypospadias, epispadias, chordia, and penoscrotal web, respectively.
Regarding these deformities, 15.4% of the participants stated that they would recommend conventional circumcision, 45.9% stated that they would not recommend it, and 38.7% stated that they had no opinion on this issue and would instead consult to the relevant branch for guidance
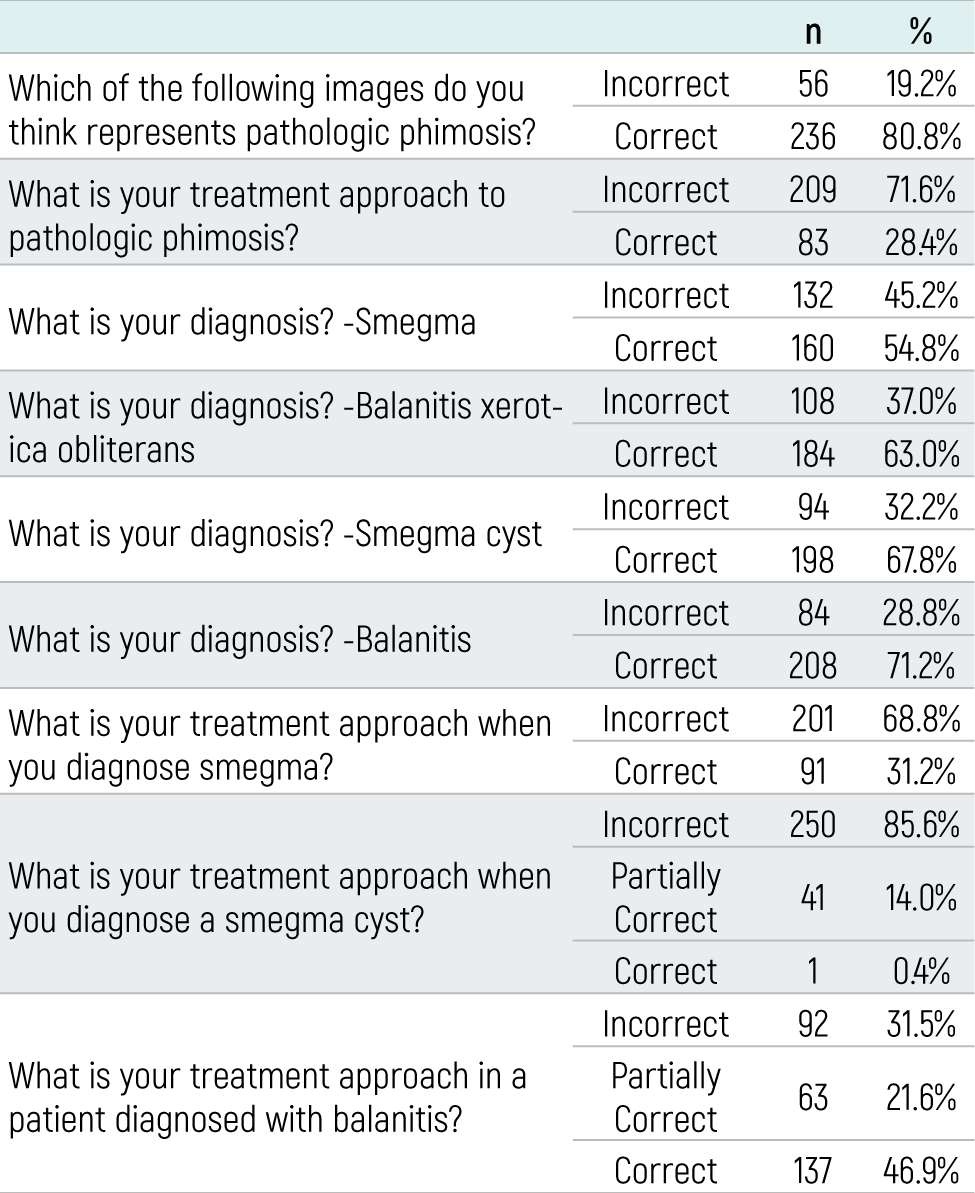
Table 3 shows the distribution of the results of the participants’ answers to the information questions. According to these answers, the participants received an average score of 5.27 ± 2.18. When the test is evaluated over 11 points, the average knowledge level is 47.95 ± 19.84 points out of 100. This level indicates intermediate knowledge. The study found that knowledge scores about circumcision vary significantly by to gender, age, and professional seniority. In the study, it was observed that male participants had higher knowledge levels than female participants (p = 0.04) (t-test analysis), participants over 46 years of age had higher knowledge levels than other age groups (p = 0.01) (Variance test analysis), and participants with more than 10 years of professional seniority had higher knowledge levels than other professional seniority groups (p = 0.02) (Variance test analysis).
Discussion
Based on the developmental stage and cultural attributes of each country, circumcision can vary in terms of performers, settings, timing, and underlying motivations. For instance, in the United States, circumcision is typically performed by pediatricians, family physicians, or obstetricians within a hospital environment.2 However, ceremonial circumcisions may involve traditional circumcizers representing various religious or ethnic groups.3 Similarly, in cross-sectional studies conducted in the United States, a lower circumcision rate was noted, which is often attributed to religious factors.4 A study conducted in Türkiye highlighted that the primary motive for families considering circumcision was religion and tradition (84.8%); this rate tended to increase as the level of education decreased.5 Furthermore, Rediger et al. reported that parents’ decisions to circumcise their children were influenced by their own religious beliefs as well as the physicians’ opinions.6 From a ceremonial perspective, circumcision is performed in the neonatal period (day 8) in the Jewish community, while no specific age range is recommended in Muslim communities.7 From a medical perspective, the American Academy of Pediatrics recommends circumcision in the neonatal period to prevent urinary tract infections (UTIs), whereas no specific circumcision age range is recommended to prevent other diseases.4 In addition, during the “phallic stage” of child development (3–6 years), penile surgery is not recommended for children, and it is recommended to use general anesthesia and local anesthetic techniques to minimize pain and suffering during circumcision.4,5 Upon analyzing the viewpoints of the participating pediatricians, it was observed that the percentage of those who regarded circumcision as a component of their cultural or religious identity was lower than that of the general population. Nevertheless, a significant majority of the participants indicated that they had either already circumcised their own children or were contemplating doing so. In addition, there was no statistically significant difference between the opinions of the participating pediatricians regarding the circumcision of their own children, regardless of whether they had a male child or not. These findings suggest that respondents who hold similar views to the community are more likely to recommend elective circumcision. However, it was observed that the pediatricians who participated in our study recommended circumcision mostly within the age bracket of 6–10 years and during the neonatal period, while circumcision during the phallic stage was less frequently endorsed. In addition, most pediatricians who participated in our study stated that circumcision should be performed by surgeons, preferably pediatric surgeons, and pediatric urology and urology specialists in a hospital setting under sedation or local anesthesia in the presence of an anesthesiologist. We believe that the pediatricians who participated in our study also made suggestions in this direction while counseling their parents. There are differing views as to whether prophylactic and ritual circumcision can be performed with parental consent. Opponents of circumcision raise concerns related to the child’s right to bodily integrity, the potential for nonprofessionals to perform the procedure in unsuitable settings, and the financial burden of ritual circumcision on health insurance. On the contrary, advocates of circumcision underscore the parents’ constitutional freedom of religion and their right to raise the child in accordance with the religious beliefs of the child’s affiliation.3,8 Although circumcision is offered free of charge under health insurance in Türkiye, a study reported that 13.3% of circumcisions were performed by traditional circumcizers in inappropriate settings.4 This rate might further rise if circumcision is legally restricted or excluded from health insurance coverage. A significant portion of the participating pediatricians in our study also conveyed the viewpoint that legislation against circumcision should not be enacted and that the decision should remain with the parents. We believe that the continued provision of circumcision free of charge within the scope of social security in hospital settings in Türkiye is important to mitigate the risk of complications and prevent circumcisions performed by inexperienced individuals.
Currently, research and practical endeavors concerning the impact of circumcision on the management of specific urological issues and infections are ongoing. In this context, studies show that circumcision reduces the risk of human papillomavirus infection, cervical cancer, trichomonas vaginalis, bacterial vaginosis, and genital ulcers in women, and adult circumcision reduces the risk of human immunodeficiency virus infection by approximately 60% .9,10 In addition, it has been reported that local steroids can be used for the treatment of inflammatory diseases such as balanitis xerotica obliterans, and in some cases, circumcision may have a curative impact on these patients.11 Emergency circumcision may be required in the treatment of paraphimosis.7 In their study, Mishra et al. demonstrated a reduction in periurethral contamination with organisms responsible for UTIs in children following circumcision.12 However, it has been reported that circumcision decreases the incidence of UTI in boys who have had a previous UTI and are likely to have recurrent infections.13 In a meta-analysis by Wahyudi et al., it was reported that circumcision decreased the incidence of UTI in all urinary tract anomalies such as congenital hydronephrosis, vesicoureteral reflux, posterior urethral valve, megaureter, and ureteropelvic junction stenosis.14 In fact, circumcision can be described as a simple and effective treatment method in the management and prevention of certain mentioned urological problems and infections. However, it is observed that the pediatricians participating in our study recommended circumcision at a lower rate than expected for these patient groups, and we believe that organizing necessary trainings may be required to increase these rates. Furthermore, the literature encompasses studies investigating the impact of circumcision on male sexuality, offering varying perspectives ranging from positive to negative and even inconclusive outcomes.15,16 However, there are no scientific data showing a clear benefit of circumcision during the treatment of nonorganic enuresis.17 In line with existing literature, our study also revealed that participants held differing opinions regarding the influence of circumcision on male sexuality and did not recommend circumcision as a treatment for enuresis.
While a significant majority of the participating pediatricians demonstrated the ability to visually recognize pathological phimosis, their effectiveness in treating the condition varied. In addition, it was found that the majority of pediatricians who participated in the study tended to recommend circumcision for recurrent balanitis and pathological phimosis, even if their approach to balanitis was correct. However, studies have shown that pathological phimosis can be treated with topical steroids, balanitis can be treated with local care (warm water cleansing, topical antifungal, and topical antibiotic), and pathologic phimosis and recurrent balanitis are not absolute indications for circumcision.7,18,19 The majority of the pediatricians who participated in our study could make the decision to circumcise patients with pathological phimosis and balanitis more easily in our country, where ritual circumcision is common.
The pediatricians who participated in our study were found to be well aware of penile deformities such as hypospadias, epispadias, and buried penis but less aware of conditions such as smegma cysts and smegma. In previous studies, circumcision has been considered contraindicated in congenital anomalies of the penis, such as chordia, hypospadias, epispadias, and penoscrotal web.20,21 In addition, it has been reported that genital hygiene is important in cases where smegma (the natural secretion of the preputium) and smegma cysts (formed by the accumulation of smegma in some areas of the preputium) occur. When the preputium becomes more retractile, these lesions will disappear spontaneously and do not need to be treated with circumcision.7,22,23 Most pediatricians who participated in our study referred patients to a surgical specialist instead of recommending circumcision in cases of penile deformities, smegma, and smegma cysts. Therefore, pediatricians are thought to safeguard numerous children from potential complications and unwarranted interventions through proper guidance, even if they may have a lower likelihood of diagnosing certain illnesses.
The data from the knowledge-based questions revealed that the participating pediatricians’ knowledge level concerning circumcision and the preputium falls within an intermediate range. This suggests that some participants have incomplete or incorrect information about circumcision and the preputium. Hence, it can be concluded that there is a need for educational efforts regarding circumcision and the preputium among the participants. According to the data, it was determined that the level of knowledge of male participants about circumcision was significantly higher than that of female participants. This difference could be attributed to the fact that men have more social and cultural awareness concerning circumcision. In the evaluation made according to age groups, it was found that participants aged ≥46 years had significantly higher levels of knowledge about circumcision compared to other age groups. Likewise, in the evaluation made according to professional seniority levels, it was determined that the knowledge levels of the participants with 10 years and above seniority were higher than the other seniority groups. This could be attributed to the accumulation of experience and knowledge throughout one’s professional career with age. These findings indicate a requirement for education regarding circumcision and the preputium among the participants. Targeting specific groups and fostering continuous learning through lifelong education can further enhance knowledge levels during training planning.
Declarations
Animal and Human Rights Statement
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the Declaration of Helsinki and its later amendments.
Informed Consent
Informed consent was obtained electronically from all participants before participation in the study.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Conflict of Interest
The authors declare no conflict of interest.
Funding
None.
Author Contributions (CRediT Taxonomy)
Conceptualization: C.Ş.; N.G.
Methodology: C.Ş.; N.G.
Data Curation: C.Ş.
Formal Analysis: C.Ş.; N.G.
Investigation: C.Ş.; N.G.
Writing – Original Draft Preparation: C.Ş.
Writing – Review & Editing: N.G.
Supervision: N.G.
Scientific Responsibility Statement
The authors declare that they are responsible for the scientific content of the manuscript, including study design, data collection, analysis and interpretation, manuscript preparation, and approval of the final version.
Abbreviations
ANOVA: Analysis of Variance
CI: Confidence Interval
KR-21: Kuder–Richardson Formula 21
SD: Standard Deviation
SPSS: Statistical Package for the Social Sciences
UTI: Urinary Tract Infection
References
-
Morris BJ, Wamai RG, Henebeng EB, et al. Estimation of country-specific and global prevalence of male circumcision. Popul Health Metr. 2016;14(1):1-13.
-
Stang HJ, Snellman LW. Circumcision practice patterns in the United States. Pediatrics. 1998;101(6):e5. doi:10.1542/peds.101.6.e5
-
Ventura F, Caputo F, Licata M, et al. Male circumcision: ritual, science and responsibility. Ann Ist Super Sanita. 2020;56(3):351-358.
-
Blank S, Brady M, Buerk E, et al. Male circumcision. Pediatrics. 2012;130(3):e756-e785. doi:10.1542/peds.2012-1990
-
Şahin F, Beyazova U, Aktürk A. Attitudes and practices regarding circumcision in Turkey. Child Care Health Dev. 2003;29(4):275-280. doi:10.1046/j.1365-2214.2003.00342.x
-
Rediger C, Muller AJ. Parents’ rationale for male circumcision. Can Fam Physician. 2013;59(2):e110-e115.
-
Prabhakaran S, Ljuhar D, Coleman R, Nataraja RM. Circumcision in the paediatric patient: a review of indications, technique and complications. J Paediatr Child Health. 2018;54(12):1299-1307. doi:10.1111/jpc.14206
-
Morris BJ, Moreton S, Krieger JN. Critical evaluation of arguments opposing male circumcision: a systematic review. J Evid Based Med. 2019;12(4):263-290. doi:10.1111/jebm.12361
-
Morris BJ, Hankins CA, Banerjee J, et al. Does male circumcision reduce women’s risk of sexually transmitted infections, cervical cancer, and associated conditions? Front Public Health. 2019;7:4. doi:10.3389/fpubh.2019.00004
-
Prodger JL, Galiwango RM, Tobian AAR, et al. How does voluntary medical male circumcision reduce HIV risk? Curr HIV/AIDS Rep. 2022;19(6):484-490. doi:10.1007/s11904-022-00634-w
-
Ghidini F, Virgone C, Pulvirenti R, Trovalusci E, Gamba P. Could a careful clinical examination distinguish physiologic phimosis from balanitis xerotica obliterans in children? Eur J Pediatr. 2021;180(2):591-595. doi:10.1007/s00431-020-03881-4
-
Mishra K, Isali I, Sindhani M, et al. Characterization of changes in penile microbiome following pediatric circumcision. Eur Urol Focus. 2023;9(4):669-680. doi:10.1016/j.euf.2022.12.007
-
Renko M, Salo J, Ekstrand M, et al. Meta-analysis of the risk factors for urinary tract infection in children. Pediatr Infect Dis J. 2022;41(10):787-792. doi:10.1097/inf.0000000000003628
-
Wahyudi I, Raharja AR, Situmorang GR, Rodjani A. Circumcision reduces urinary tract infection in children with antenatal hydronephrosis: systematic review and meta-analysis. J Pediatr Urol. 2023;19(1):66-74. doi:10.1016/j.jpurol.2022.10.029
-
Banuelos MB, Garcia JL. Circumcision in childhood and male sexual function: a blessing or a curse? Int J Impot Res. 2021;33(2):139-148.
-
Morris BJ, Krieger JN. The contrasting evidence concerning the effect of male circumcision on sexual function, sensation, and pleasure: a systematic review. Sex Med. 2020;8(4):577-598. doi:10.1016/j.esxm.2020.08.011
-
Coşkun A, Erdem K. The relationship between monosymptomatic enuresis and circumcision: is it beneficial or traumatic? A randomized study. South Clin Ist Euras. 2023;34(1):49-53.
-
Falcao BP, Stegani MM, Matias EF. Phimosis and circumcision: concepts, history, and evolution. Int J Med Rev. 2018;5(1):6-18.
-
Javaid AA, Powell K, Awad K. Guideline review NICE Clinical Knowledge Summary: balanitis in children. Arch Dis Child Educ Pract Ed. 2022;107(2):131-132. doi:10.1136/archdischild-2020-321303
-
Osinibi E, Smith T, Henderson A. A primary care update to circumcision. InnovAiT. 2020;13(3):173-178. doi:10.1177/1755738019891189
-
Zeitler M, Rayala B. Neonatal circumcision. Prim Care. 2021;48(4):597-611. doi:10.1016/j.pop.2021.08.002
-
Fahmy MA. Smegma. In: Fahmy MA, ed. Normal and abnormal prepuce. 1st ed. Springer; 2020:153-161. doi:10.1007/978-3-030-37621-5_17
-
Drake T. Foreskin problems in boys. Trends Urol Mens Health. 2014;5(2):28-30. doi:10.1002/tre.387
Tables
Table 1. Participants’ opinions about the recommended age, setting, operator, and anesthesia method for circumcision.
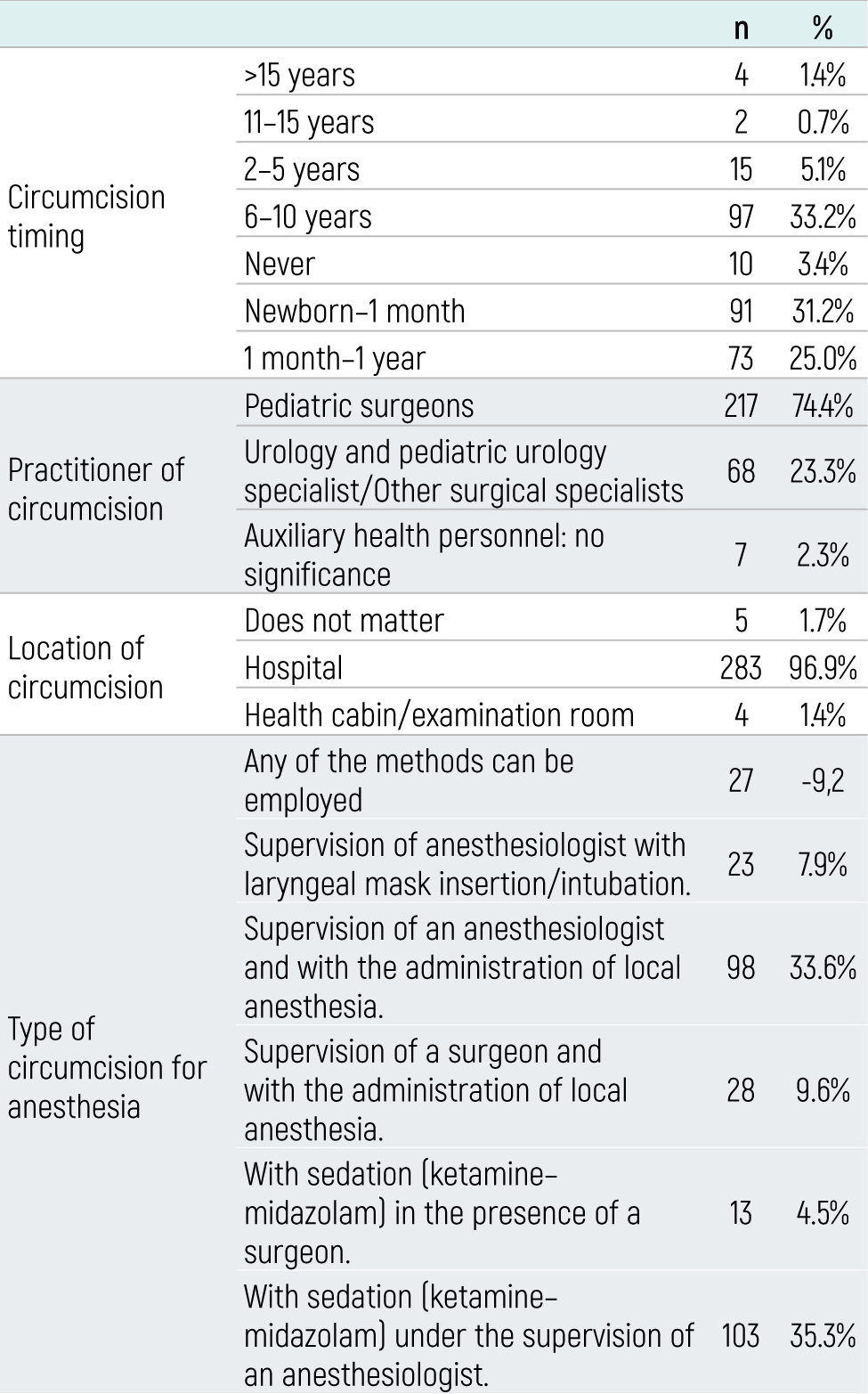
Table 2. Several viewpoints of participants regarding circumcision.
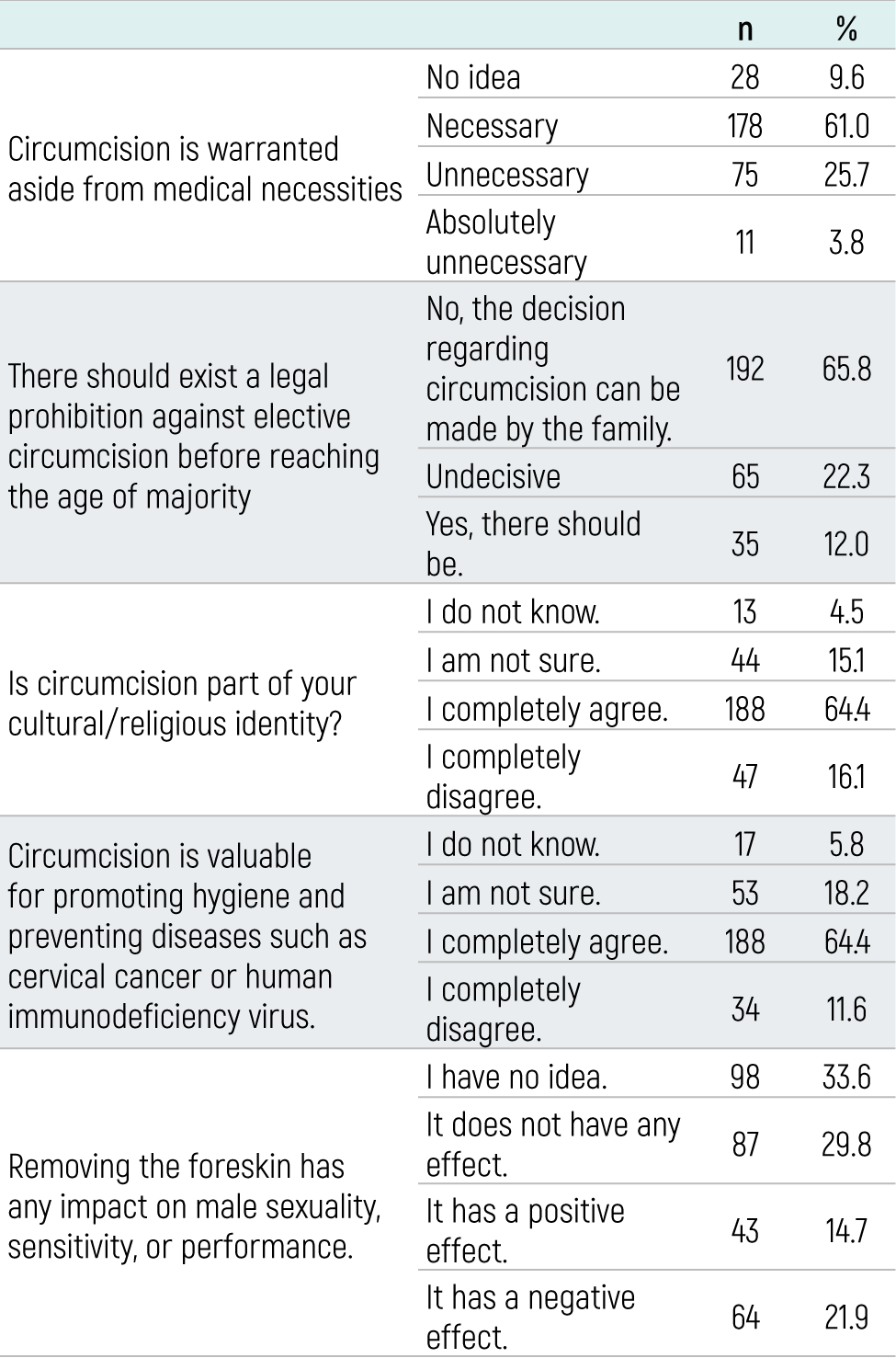
Table 3. Distribution of participants’ responses to knowledge-based questions
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Ceyhan Şahin, Neslihan Gülçin. Opinions and knowledge level of pediatricians on circumcision. Eu Clin Anal Med 2023;11(3):55-59. doi:10.4328/ECAM.10056
- Received:
- August 14, 2023
- Accepted:
- August 30, 2023
- Published Online:
- August 30, 2023
- Printed:
- September 1, 2023