Comparison of clinical outcomes of conservatively treated type 5 and type 6 fractures in distal radius according to frykman classification
Results of treated frykman type 5 and type 6 fractures in radius
Authors
Abstract
AimDistal radius fractures are among the most common upper extremity fractures and are often associated with ulnar styloid fractures. Ulnar styloid fractures can potentially lead to instability and pain in the distal radioulnar joint. This retrospective study aims to investigate the clinical and radiological effects of ulnar styloid fractures in conjunction with distal radius fractures.
MethodsIn this retrospective study, 64 (group 1: 33 patients, group 2: 31 patients) patients with distal radius fractures were enrolled. Specifically, patients with type 5 and type 6 fractures, according to the Frykman classification, were included in the study from January 2016 to December 2022. All patients in this study received conservative treatment at Selcuk University Orthopaedics Clinic.
ResultsFurthermore, there were no significant differences observed between the groups in terms of fracture type, range of motion, pain and instability in the distal radioulnar joint (DRUJ), grip strength, Visual Analog Scale (VAS) scores, Disabilities of the Arm, Shoulder, and Hand (DASH) scores, as well as Gartland-Werley and Green & O’Brien tests.
Comparison of clinical and radiological parameters between the groups revealed no statistically significant differences.
ConclusionThe impact of ulnar styloid fractures on distal radius fractures is not fully illuminated in the literature. While it is claimed that styloid fractures may affect the TFCC and that ulnar-sided pain could be persistent, opposing views suggest that the outcome remains unchanged. In our study, our radiological and functional comparisons also indicated that the result did not change statistically.
In summary, regardless of whether an ulnar styloid fracture accompanies distal radius fractures, it does not appear to significantly impact the outcomes.
Keywords
Introduction
In the case of a patient with a distal radius fracture, treatment and rehabilitation protocols are tailored according to the fracture’s type and specific patient circumstances.1
Distal radius fractures are the most common fractures in the upper extremity and are associated with ulnar styloid fractures in approximately 55% of cases.1 The ulnar styloid serves as an attachment point for the triangular fibrocartilage complex (TFCC), where it is anchored. The TFCC facilitates the coordinated movement and function of the distal radius, ulnar head, and proximal row of carpal bones. Consequently, a fractured ulnar styloid is believed to potentially lead to instability and the development of pain in the distal radioulnar joint.2,3,4
The impact of ulnar styloid fractures on functional outcomes remains uncertain. Numerous clinical studies have yielded conflicting results, with some indicating that ulnar styloid fractures do not affect functional, anatomical, or radiographic aspects. However, several other studies have shown an association between ulnar styloid fractures and distal radioulnar joint instability.4,5
In this study, patients with and without ulnar styloid fractures, both conservatively treated, will be retrospectively classified. Frykman’s6 type 5 and type 6 fractures will be compared, aiming to determine whether there is a correlation between styloid fractures and distal radioulnar joint instability and pain. Additionally, the study will seek to establish whether there are any functional differences between those with ulnar styloid fractures and those without.
Materials and Methods
Between January 2016 and September 2022, a retrospective evaluation was conducted on 64 patients with distal radius fractures who were treated at the Orthopedics and Traumatology Clinic of Selcuk University Faculty of Medicine Hospital.
Demographic information, examination results, and radiographs of the patients were reviewed. Functional and clinical outcomes of the patients at the end of the first year were assessed based on objective and subjective criteria. Radiological evaluation was conducted using hospital archives.
Patients who regularly attended follow-up appointments and adhered to recommendations during a one-year period were considered for inclusion.
Exclusion CriteriaPatients under 18 or over 65 years old, those with malnutrition, chronic kidney insufficiency, a history of previous wrist surgery, prior fractures in the same wrist, or those who had experienced multiple traumas were not included in the study. Patients who developed reflex sympathetic dystrophy during follow-ups and those who did not attend regular follow-up appointments were also excluded from the study.
Fifteen patients under the age of 18 who did not have one-year follow-ups were excluded from the study. Additionally, 19 patients who did not attend follow-up appointments and 3 patients who developed reflex sympathetic dystrophy were also excluded from the study.
Patients classified as Frykman type 5 and type 6 fractures, who had undergone conservative treatment. The patients were categorized into two groups. Group 1 consisted of patients with only distal radius fractures, totaling 33 patients, while group 2 included patients with both distal radius fractures and ulnar styloid fractures, totaling 31 patients.
The presence of distal radioulnar joint (DRUJ) instability was examined in conjunction with the opposite side and recorded. When assessing DRUJ instability, the radius was held steady, while the ulna distal end was moved forward and backward, it was categorized into four grades and compared with the opposite side.
In subjective assessment, VAS (Visual Analog Scale) scores and DASH (Disabilities of the Arm, Shoulder, and Hand) scores were utilized. In clinical and functional evaluations, the Gartland-Werley Scoring and Green & O’Brien clinical scoring results were employed.
Radiological evaluation involved classification of distal radius fractures according to the Frykman classification based on initial radiographs. Patients wrist pre-treatment radiographs and post-treatment radiographs in final follow-up, were assessed. In the evaluation, arthritic changes from radiological findings were scored using the Knirk and Jupiter arthritic scoring system.7 Angular measurements were performed according to Stewart et al.’s radiological evaluation system.8 Dorsal angulation, radial length loss, and radial angulation loss were measured and assessed. Ulnar styloid was evaluated in the final follow-up films, recording cases of union and non-union.
Patients who met the criteria for closed reduction and had their fractures reduced were followed up with weekly radiographic assessments until around 6 weeks. During follow-up visits, radiographic assessments were performed to check for any displacement. Fracture union was evaluated, considering the formation of callus tissue and the absence of pain upon palpation. Casts were removed after 6 weeks. Functional outcomes of patients who completed the 12-month follow-up were compared.
Ethical ApprovalThis study was approved by the Ethics Committee of Selcuk University Faculty of Medicine (Date: 15.09.2023, Decision No: 2023/67).
Statistical AnalysisFor the statistical analysis of the data, the SPSS 16.0 software package was utilized. Categorical measurements were summarized as numbers and percentages, while continuous measurements were presented as mean ± standard deviation or median. To compare categorical measurements between groups, the Chi-squared test, the Mann-Whitney U test and the Student t-test were utilized. In all tests, a significance level of p<0.05 was considered statistically significant.
Reporting GuidelinesThe study was reported in accordance with STROBE guidelines.
Results
A total of 64 patients who met the inclusion criteria and were followed for distal radius fractures were included in the study. The distribution of patients by gender in each group is presented in Table 1.
In Group 1, it was noted that the affected side was the dominant side in 78% of cases, while in Group 2, it was observed that the affected side was the dominant side in 75% of cases. There was no statistically significant difference between the groups in terms of age and dominant side rate (p=0.08) .
Furthermore, in Group 2, it was determined that in 5 patients, there were styloid base fractures or displacements exceeding 2 mm. The other styloid fractures were under 2 mm.
At the conclusion of the study, the assessment revealed that, in Group 2, all ulnar styloid fractures had healed except for two cases, and there were no unresolved styloid fractures.
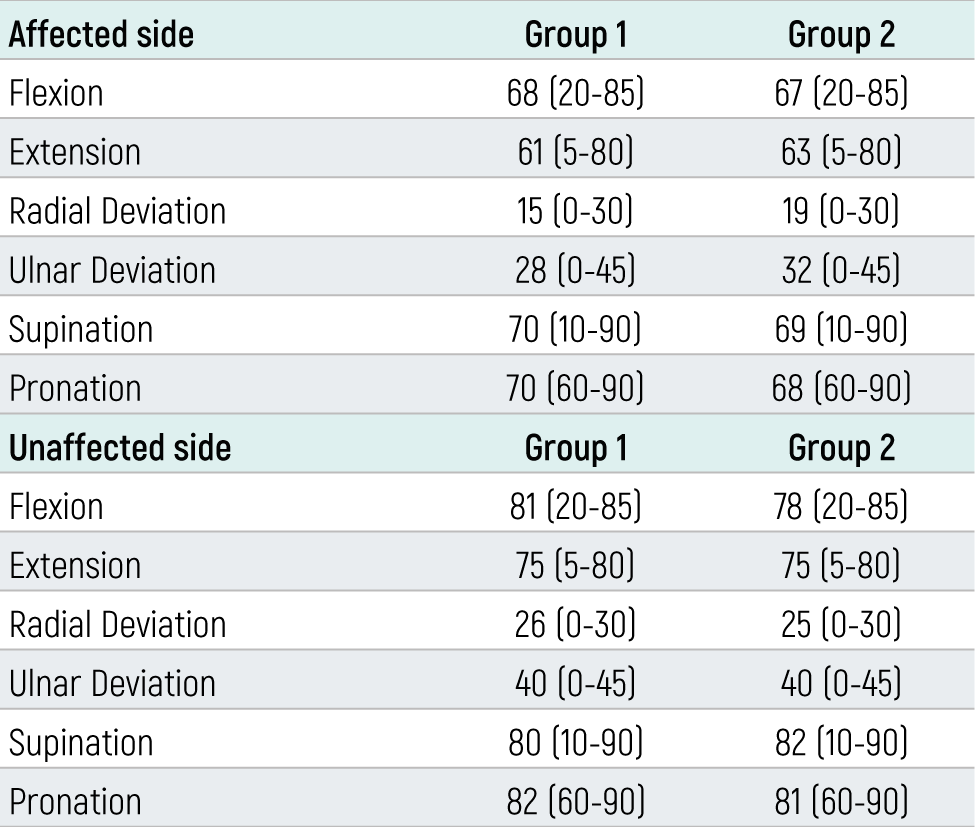
Objective FindingsDuring the final follow-up evaluations, the average range of motion for patients in Group 1 and Group 2 were shown in Table 2. There were no statistically significant differences (p=0.17, which is greater than 0.05).
Range of motion on the unaffected side was also evaluated and compared (Table 2).
The average handgrip strength was measured as 33 kg for Group 1 and 29 kg for Group 2.
When patients in Group 1 and Group 2 were compared in terms of handgrip strength, no statistically significant difference was found (p=0.18).
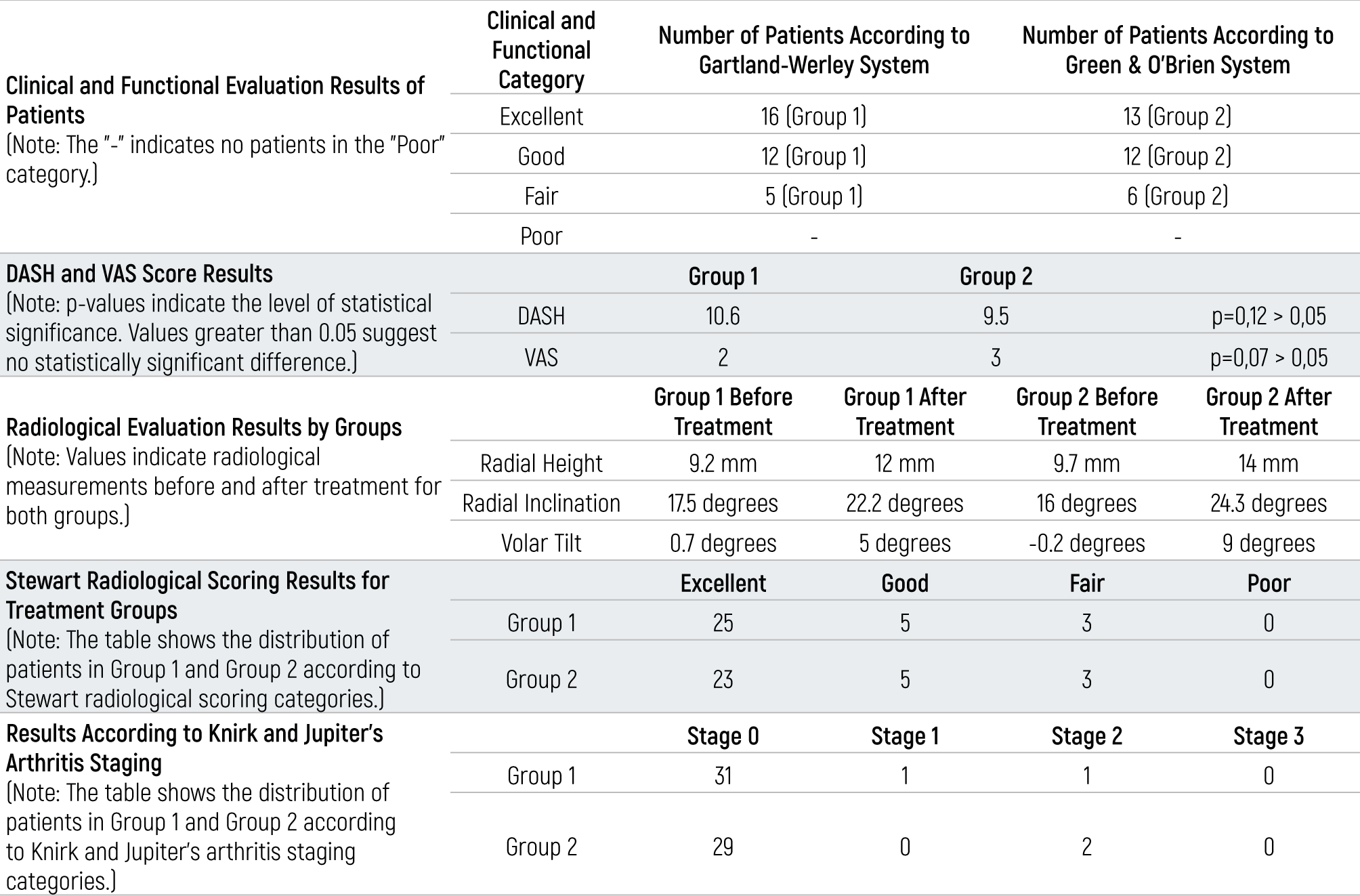
Clinical FindingsClinical evaluation was conducted using the Green and O’Brien clinical scoring system, the Gartland and Werley clinical scoring system, the DASH score, the VAS score, ulnar pain and DRUJ instability (Table 3).
In Group 1, there were no patients with ulnar wrist pain. However, in Group 2, 2 patients had ulnar wrist pain.
When evaluating distal radioulnar joint (DRUJ) instability, it was found that there was no DRUJ instability in Group 1 patients. On the other hand, 1 patient in Group 2 exhibited instability. There was no statistically significant difference between the groups in terms of Gartland-Werley and Green & O’Brien systems, the DASH score, Vas score, ulnar wrist pain and DRUJ instability. (p=0.08, p=0.12, p=0.05, p=0.09, p=0.09 properly).
Radiological FindingsIn the comparison made between the two treatment groups based on average values of fractures, Stewart radiological score system and Knirk and Jupiter’s arthritis staging, no statistically significant relationship was found (Table 3).
Discussion
Distal radius fractures are often accompanied by ulnar styloid fractures, and ulnar styloid fractures have been considered a potential cause of poor outcomes following distal radius fracture treatment. However, some authors disagree with this view. In our study, we aimed to determine whether there are functional and radiological differences between patients with ulnar styloid fractures and those without, as well as to investigate the presence of distal radioulnar joint instability and wrist pain.
These fractures are more commonly observed in males than in females. In our study, the rate of occurrence in males was found to be 54.9%.9
The dominant extremity involvement may provide insights into the mechanism of injury, but in our study, it did not show a significant association with the presence of ulnar styloid fractures or the outcomes of treatment.
Our study found no significant differences in functional and radiological outcomes, wrist pain, or distal radioulnar joint instability between patients with and without ulnar styloid fractures in the context of distal radius fractures. This suggests that the presence of ulnar styloid fractures may not be a critical factor affecting the overall treatment outcomes of distal radius fractures. However, further research with larger sample sizes and longer follow-up periods may provide additional insights into this topic.
Distal radius fractures occurring in conjunction with ulnar styloid fractures have been the subject of ongoing debate regarding whether ulnar styloid should be fixed or not. These fractures are frequently associated with ulnar styloid base fractures. Large ulnar styloid fractures may involve at least a portion of the triangular fibrocartilage complex (TFCC), potentially contributing to TFCC tears. However, the extent of ulnar styloid base fractures’ contribution to limitations in forearm rotation, wrist pain, and the development of distal radioulnar joint instability is not well-established, and there is a lack of extensive research in this area.10,11
Many authors have suggested that one of the reasons for achieving suboptimal outcomes in distal radius fractures is the presence of ulnar styloid fractures.3 This assertion is based on the fact that the triangular fibrocartilage complex (TFCC) originates from the ulnar styloid base, and repairing ulnar styloid base fractures may potentially restore distal radioulnar joint stability.12 In a study conducted by May and colleagues, out of 166 patients with distal radius fractures, 14 had distal radioulnar joint instability, and 11 of these patients had ulnar styloid base fractures. The study concluded that ulnar styloid base fractures and ulnar styloid fractures of 2 mm or more were risk factors for distal radioulnar joint instability in patients.13
In a study conducted by Stoffelen and colleagues on 272 patients with distal radius fractures, they observed distal radioulnar joint instability in 13 patients, all of whom were reported to have ulnar styloid base fractures.14 They also noted that patients with ulnar styloid base fractures had worse outcomes compared to those without such fractures.
Similarly, in a study by Ruch and colleagues, they compared patients with ulnar styloid base fractures who underwent cast immobilization in supination to those treated using the tension band technique. They reported that patients treated with cast immobilization in supination had better outcomes.15
In a study by Velmurugasam and colleagues, they compared patients with significant ulnar styloid fractures who were treated with surgery for distal radius fractures without specific treatment for the ulnar styloid fracture. The study did not find a significant difference in outcomes between the two groups.16
While some studies suggest the importance of detecting ulnar styloid fractures, other studies have found that even when these fractures are not specifically identified and treated, the outcomes may still be similar.17
At the end of our study, it was determined that clinical and radiological scores in the evaluated patients, according to the Gartland and Werley clinical assessment criteria, DASH and VAS scoring results, and the Steward radiological scoring for radiological assessment, showed parallelism in patients. There was no statistically significant difference found within each parameter among the groups.
When compared in terms of grip strength, a decrease in strength on the affected side was observed, but the rate of loss was the same across all groups.
Limitations
Limitations were the small sample size and retrospective nature of the study, as well as the assessment of DRUJ instability through physical examination.
Conclusion
There was no statistically significant difference in wrist range of motion (ROM), distal radioulnar joint instability, ulnar-sided wrist pain, wrist grip strength, VAS scores and DASH scores, Gartland-Werley Scoring and Green & O’Brien clinical scoring systems between patients with and without ulnar styloid fractures.
The results indicate that ulnar styloid fractures do not have an impact on functional and radiological outcomes in conservatively managed distal radius fractures without ulnar styloid fractures.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was waived by the Ethics Committee due to the retrospective design of the study.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare no conflict of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content including study design, data collection, analysis and interpretation, writing, some of the main line, or all of the preparation and scientific review of the contents and approval of the final version of the article.
Abbreviations
DASH: Disabilities of the arm, shoulder, and hand
DRUJ: Distal radioulnar joint
ROM: Range of motion
TFCC: Triangular fibrocartilage complex
VAS: Visual analog scale
References
-
Shapiro LM, Kamal RN. Distal radius fracture clinical practice guidelines-updates and clinical implications. J Hand Surg Am. 2021;46(9):807-811. doi:10.1016/j.jhsa.2021.07.014
-
Jawed A, Ansari MT, Gupta V. TFCC injuries: how we treat? J Clin Orthop Trauma. 2020;11(4):570-579. doi:10.1016/j.jcot.2020.06.001
-
Ding BTK, Pillay K, Sechachalam S. Radial shaft fracture obliquity as a predictor of distal radioulnar joint instability. J Hand Surg Eur Vol. 2018;43(7):732-738. doi:10.1177/1753193418756591
-
Kim KW, Lee CH, Choi JH, Ahn JM, Gong HS. Distal radius fracture with concomitant ulnar styloid fracture: does distal radioulnar joint stability depend on the location of the ulnar styloid fracture? Arch Orthop Trauma Surg. 2023;143(2):839-845.
-
Ajit Singh V, Jia TY, Santharalinggam RD, Gunasagaran J. Relationship of ulna styloid fracture to the distal radio-ulnar joint stability: a clinical, functional, and radiographic outcome study. PLoS One. 2023;18(1). doi:10.1371/journal.pone.0279210
-
de Alencar Neto JB, Jales CS, Coelho JVV, Souza CJD, Cavalcante MLC. Epidemiology, classification, and treatment of bilateral fractures of the distal radius. Acta Ortop Bras. 2022;30(3). doi:10.1590/1413-785220223003e245185
-
Esworthy GP, Johnson NA, Divall P, Dias JJ. Origins of the threshold for surgical intervention in intra-articular distal radius fractures. Bone Joint J. 2021;103-B(9):1457-1461. doi:10.1302/0301-620x.103b9.bjj-2021-0313.r1
-
Paul AW, Athens CM, Patel R, Rizzo M, Rhee PC. Effect of trapeziectomy on carpal stability. Hand (N Y). 2022;17(3):432-439. doi:10.1177/1558944720939198
-
Cuenca J, Martinez AA, Herrera A, Domingo J. The incidence of distal forearm fractures in Zaragoza, Spain. Chir Main. 2003;22(4):211-215. doi:10.1016/s1297-3203(03)00057-x
-
Skalski MR, White EA, Patel DB, Schein AJ, Melo HR, Matcuk GR. The traumatized TFCC: an illustrated review of the anatomy and injury patterns of the triangular fibrocartilage complex. Curr Probl Diagn Radiol. 2016;45(1):39-50. doi:10.1067/j.cpradiol.2015.05.004
-
Simic PM, Weiland AJ. Fractures of the distal aspect of the radius: changes in treatment over the past two decades. Instr Course Lect. 2003;52:185-195. doi:10.2106/00004623-200303000-00026
-
Srinivasan RC, Shrouder-Henry JJ, Richard MJ, Ruchet DS. Open and arthroscopic triangular fibrocartilage complex (TFCC) repair. J Am Acad Orthop Surg. 2021;29(12):518-525. doi:10.5435/jaaos-d-20-00998
-
May MM, Lawton JN, Blazar PE. Ulnar styloid fractures associated with distal radius fractures: incidence and implications for distal radioulnar joint instability. J Hand Surg Am. 2002;27(6):965-971. doi:10.1053/jhsu.2002.36525
-
Stoffelen D, De Smet L, Broos P. The importance of the distal radioulnar joint in distal radial fractures. J Hand Surg Br. 1998;23(4):507-511. doi:10.1016/s0266-7681(98)80134-4
-
Ruch DS, Lumsden BC, Papadonikolakis A. Distal radius fractures: a comparison of tension band wiring versus ulnar outrigger external fixation for the management of distal radioulnar instability. J Hand Surg Am. 2005;30(5):969-977. doi:10.1016/j.jhsa.2005.05.005
-
Velmurugesan PS, Nagashree V, Davendra A, Dheenadhyalan J, Rajasekaran S. Should ulnar styloid be fixed following fixation of a distal radius fracture? Injury. 2023;54(7):110768. doi:10.1016/j.injury.2023.04.055
-
Wijffels MM, Keizer J, Buijze GA, et al. Ulnar styloid process nonunion and outcome in patients with a distal radius fracture: a meta-analysis of comparative clinical trials. Injury. 2014;45(12):1889-1895. doi:10.1016/j.injury.2014.08.007
Tables
Table 1. Distribution of patients by gender in groups
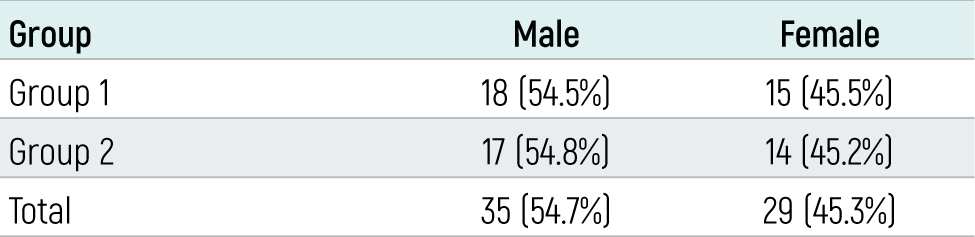
Table 2. Mean range of motion values for the affected and unaffected side
Note: Values are presented as mean (range)
Table 3. Comparison of clinical (objective and subjective), radiological, and functional results between two groups
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Selim Safalı, Fatih Durgut. Comparison of clinical outcomes of conservatively treated type 5 and type 6 fractures in distal radius according to frykman classification. Eu Clin Anal Med 2023;11(Suppl 1):S38-42. doi:10.4328/ECAM.10074
- Received:
- October 6, 2023
- Accepted:
- October 14, 2023
- Published Online:
- October 14, 2023
- Printed:
- October 15, 2023