Squamous cell carcinoma of nasal septum: A Case Report
Primary nasal septum malignancy
Authors
Abstract
IntroductionPrimary nasal septum tumours are extremely rarely seen among nasal cavity tumours and mostly originate from the end section of the caudal septum. Septum tumours are seen with complaints such as recurrent epistaxis, nasal obstruction, discharge, facial oedema or pain.Case PresentationIn the examination of a patient who presented with complaints of breathing difficulties, there was seen to be a bleeding lesion of approximately 20 x 15 mm which was crusted over and raised from the mucosa, over the medial crus in the anterior and extending to the alar cartilage. Squamous cell carcinoma was reported as a result of the biopsy. The lesion was excised en bloc and the defect was reconstructed with a sublabial pedicled flap. Although local recurrence rates are high in nasal septum carcinomas, these are tumours which respond well to treatment if determined in the early stages.ConclusionTreatment of nasal septum malignancies includes surgical treatment, radiotherapy or combined treatment.
Keywords
Introduction
While 0.2%-0.8% of all malignant tumours are seen in the nasal cavity and paranasal sinuses, 3% of head and neck tumours are in the nasal cavity and paranasal sinuses. Primary nasal septum malignancies constitute 9% of sinonasal malignancies.1,2
Occupational exposure of leather workers, wood workers, those engaged in nickel processing, textile workers and those producing petrol products or isopropyl alcohol manufacturers or the use of tobacco are epidemiological risk factors for nasal cavity and paranasal sinus malignant tumours. The association of these factors with nasal septal squamous cell cancers is not yet fully known.3,4,5 The clinical table of septal malignancies is formed of non-specific symptoms such as recurrent epistaxis, nasal obstruction, discharge, facial oedema or pain. As the complaints are non-specific, diagnosis may be delayed. The most common examination findings are mucosal ulceration, mass lesion, polyp, nasal deformity and perforations. To determine local spread of the disease, MR imaging is necessary and for lymph node spread and distant metastasis, USG and computed tomography imaging. Diagnosis of septum tumours is made from tissue biopsy.1,2 More than two-thirds of septum cancers originate from the anterior septum and mucocutaneous junction.6 Benign tumours of the nasal septum are rarely seen and these can be listed as chondroma, osteoma and hemangioma. The most common nasal septum malignant tumour is squamous cell carcinoma, followed by melanoma. There are reports in literature of nasal septum malignancies such as adenosarcoma, chondrosarcoma, osteosarcoma, adenoid cystic carcinoma, Merkel cell carcinoma, mucosal melanoma, neuroendocrine carcinoma and malignant lymphoma.1,2 In this paper we present the treatment approach and patient prognosis of an uncommon case diagnosed with squamous cell carcinoma in the nasal septum.
Case Presentation
A 76-year old female presented with the complaints of breathing difficulties. In the examination there was seen to be a bleeding lesion of approximately 20 x 15 mm which was crusted over and raised from the mucosa, over the medial crus in the anterior and extending to the alar cartilage. It was seen to originate from the nasal septum caudal end and was showing protrusion towards the left nasal cavity. In the detailed ear, nose and throat examination, no other pathology was determined. The histological diagnosis of the biopsy which was taken was squamous cell carcinoma. No lymphadenopathy pathology was determined on the ultrasonography and magnetic resonance imaging of the neck. Leaving an intact surgical border of 1cm, the lesion was excised en bloc, including 2/3 of the upper lip left side skin together with caudal septal cartilage and the medial crus of the left alar cartilage. Frozen samples taken from the surgical border were reported as tumour negative. For tip support, the remaining septal cartilage was taken forward by excision in a manner not to impair the upper support (Figure 1). Reconstruction was made with a sublabial pedicled flap. As there was no lymphadenopathy, neck dissection was not applied (Figure 2). In the pathology examination of the specimen, all the surgical borders were clean, no invasion of nasal septum cartilage was observed, there was no lymphovascular invasion and perineural invasion was observed. No postoperative radiotherapy was applied to the patient. After 3 months, interpolation flaps were applied by the plastic surgeon for reconstruction. At the 2, 4,6 and 12-month postoperative follow-up examinations, no pathology was determined.
Discussion
Squamous cell carcinoma is the most frequently seen type of malignant tumour of the nose. They can originate from the nasal vestibule, the lateral wall of the nose, the meatus and the septum. The lateral wall of the nose is the most common area and approximately 50% originate from the concha. Cancers rarely originate from the nasal septum, the choanal arch or the base of the nose.7
Nasal septum malignancies constitute 9% of all sinonasal malignancies. As it is a rarely seen disease, there is limited information on this subject in literature and up to 2010, fewer than 400 cases of nasal septum malignancy had been reported.1 There is no standardised classification system because of the limited numbers of this rarely seen disease.3 All sinonasal malignancies are staged according to the American Joint Committee on Cancer (AJCC-2001) classification.4
Nasal septum tumours are generally seen in males and in the 4th and 5th decades of life. In the etiology of nasal cavity and paranasal sinus malignant tumours, tobacco consumption and occupational exposure have been reported to be responsible. Leather workers, wood workers, those engaged in nickel processing, textile workers and those producing petrol products or isopropyl alcohol manufacturers are at risk.3,4,5
The patient presented in this case report was a 76-year old female. There were no risk factors associated with occupational exposure such as employment in the leather, wood or textile industries, which are held responsible for the formation of paranasal sinus and nasal cavity cancers. The patient had no history of cigarette smoking. This demonstrates that septal squamous cell carcinoma may emerge at an advanced age without any of the above-mentioned risk factors.
Symptoms are non-specific in the majority of these patients and diagnosis may be delayed as differentiation from other nasal symptoms cannot be made in the early period. The current case presented with the common non-specific complaint of nasal obstruction. Therefore, it is important that a biopsy is taken from suspicious lesions. Palpable cervical lymphadenopathy is seen at a frequency vary ing from 10% to 44%. Nasal septum carcinoma are seen together with other malignant tumours in 20%-30% of cases.6
Although local recurrence rates are high in nasal septum carcinomas, these are tumours which respond well to treatment if determined in the early stages. The most important prognostic factor is diagnosis in the early stage. Just as in the treatment of other head and neck tumours, surgical treatment, radiotherapy or combined treatment can be applied. With developments in endoscopic applications, excellent results have been obtained cosmetically and in terms of tumour control in the early stage of the disease. Large anterior nasal septum malignancies extending to the anterior nasal bone are an indication for rhinectomy. Postoperative radiotherapy is applied to reduce the recurrence rate in large lesions. After ensuring that the tumour has been completely cleared, nose reconstruction with surgery or prosthesis should be applied.1,8
As a limited, early stage tumour was detected in the current patient, surgical excision was applied and reconstruction was made with a sublabial flap. As there was no lymphadenopathy in the neck, dissection of the neck was not applied and there was no requirement for postoperative radiotherapy.
Conclusion
In cases of septal lesions which emerge with non-specific complaints and do not improve despite treatment, squamous cell carcinoma should be kept in mind. It is important that an incisional biopsy is taken from suspicious lesions in these types of patients. When diagnosis is made in the early stage, these are tumours which respond well to treatment. Close monitoring after treatment is of vital importance in the determination of early recurrence.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments.
Informed Consent
Informed consent was obtained from all participants.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the scientific content of the article, including the study design, data collection, analysis and interpretation, manuscript preparation, and approval of the final version of the manuscript.
References
-
Ho YM, Coman WB. Nasal septum malignancy. ANZ J Surg. 2011;81:533-536. doi:10.1111/j.1445-2197.2011.05669.x
-
Çukurova İ, Gümüşsoy M, Mercan GC, Yaz A, Bayol Ü. Tumors originating from the nasal septum. Bidder Tıp Bilim Derg. 2010;2(3):22-25.
-
Fornelli RA, Fedok FG, Wilson EP, Rodman SM. Squamous cell carcinoma of the anterior nasal cavity: a dual institution review. Otolaryngol Head Neck Surg. 2000;123:207-210. doi:10.1067/mhn.2000.107450
-
Allen MW, Schwartz DL, Rana V, et al. Long-term radiotherapy outcomes for nasal cavity and septal cancers. Int J Radiat Oncol Biol Phys. 2008;71(2):401-406. doi:10.1016/j.ijrobp.2007.10.031
-
Çukurova İ, Gümüşsoy M, Kaptaner S, et al. Squamous cell carcinoma originating from nasal septal perforation: a rare nasal tumor. Kulak Burun Bogaz Ihtis Derg. 2014;24(3):177-180. doi:10.5606/kbbihtisas.2014.77200
-
Özkırış M, Akbulut S, Aydın E, Ünver Ş. Squamous cell carcinoma originating from the nasal septum: a case report. Kulak Burun Bogaz Ihtis Derg. 2006;16(2):91-93.
-
Bhattacharyya N. Cancer of the nasal cavity: survival and factors influencing prognosis. Arch Otolaryngol Head Neck Surg. 2002;128:1079-1083. doi:10.1001/archotol.128.9.1079
-
NaBadalung DP. Prosthetic rehabilitation of a total rhinectomy patient resulting from squamous cell carcinoma of the nasal septum: a clinical report. J Prosthet Dent. 2003;89:234-238. doi:10.1067/mpr.2003.45
Figures
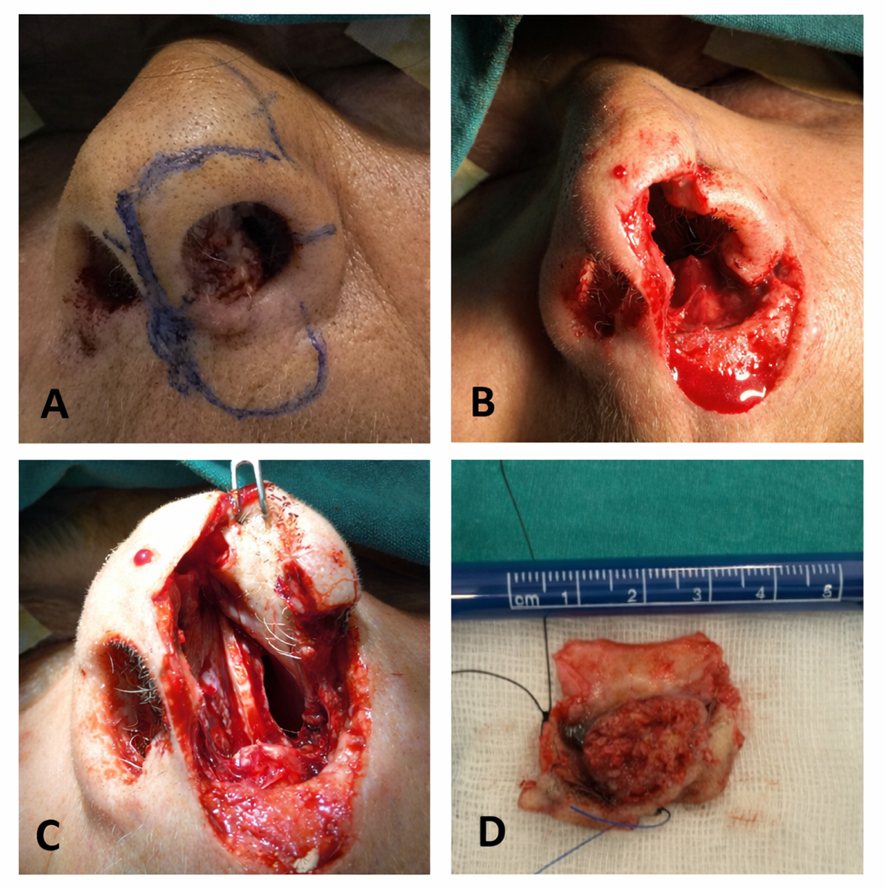
Figure 1. Squamous cell carcinoma of nasal septum (A), Surgical excision of the tumour (B,C), Specimen (D).

Figure 2. Reconstruction defect with a sublabial pedicled flap.
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Özer Erdem Gür, Nuray Ensari, Dilek Şenel, Dudu Gül Ceylan, Halit Çetin Önol. Squamous cell carcinoma of nasal septum: A Case Report. Eu Clin Anal Med 2017;5(1):11-13. doi:10.4328/ECAM.101
- Received:
- November 5, 2016
- Accepted:
- December 7, 2016
- Published Online:
- January 1, 2017
- Printed:
- January 1, 2017