Biomechanical comparison of rotational stability of long and short plates in fixation of high tibial osteotomies in the surgical treatment of osteoarthritis
Plates in osteoarthritis
Authors
Abstract
Aim High tibial osteotomy (HTO) is a widely performed surgical procedure for the treatment of medial-sided knee osteoarthritis, especially in active young, middle-aged patients. In this study, we aimed to compare the rotational stabilities of long and short plate fixation of biplanar medial opening wedge osteotomy in artificial tibia.
Material and Methods Six identical artificial left tibias were assigned to the two separate groups. The first group consisted of the subjects who had undergone medial opening wedge osteotomy fixed with short plates, and the second group with long plates. Twelve artificial seaborne left tibias were used in this study.
Results The subjects had proper biomechanical properties with ISO-9001 and ISO-14001_en quality standards in Turkey. Maximum torque, yield torque, stiffness torque, and angle values were calculated and compared for both the short and long plate groups. The values for the short plate were as follows: Max Torque:16.16±1.58, Yield Torque: 10.46±1.95, Stiffness: 0.40±.04, Torque: 3.33±76.44, Angle: 63.63±109.33, and Time 28.83±6.96. The values for the long plate were as follows: Max Torque: 19.71±4.17, Yield Torque: 11.95±3.13, Stiffness. 0.45±.08, Torque: 19.66±31.93, Angle: -20.77±54.26, and Time: 29.33±7. There was no statistically significant difference between the groups regarding the rotational stability, which was evaluated by MaxTorque, YieldTorque, stiffness, and angle time parameters.
Conclusion The use of a long plate for the fixation resulted in skin irritation in the distal part of the plate and a bigger incision with a longer time of surgery. We suggest short plates in HTO with biplanar osteotomy as short plates yielded similar biomechanical properties in terms of torsional forces.
Keywords
Introduction
High Tibial Osteotomy (HTO), which is a realignment osteotomy, is used for decreasing the load on the medial compartment of the knee, delaying the osteoarthritis (OA) progress lateral transfer of the medially deviated mechanical axis. HTO is a widely preferred surgical technique for the treatment of patients with medial gonarthrosis, especially in active young, middle-aged patients. The main aim of HTO is to relieve or release the pain by decreasing the pathologic increase of load to the medial side of the knee 1,2,3.
Lateral closing wedge osteotomy had been the most preferred technique, whereas medial opening wedge osteotomy has been more popular recently 4,5. The main aim of medial opening wedge high tibial osteotomy is to transfer the load to the lateral side by making anteromedial cuts with the use of wedges distally or proximally to the tibial tubercle. In the lateral closing wedge technique, a bone wedge is removed from the lateral tibial metaphysis. Medial opening wedge HTO has certain advantages: practical technique, more predictable correction of the deformity, and lack of the risk of peroneal nerve injury. Dome osteotomy is a proximal tibial osteotomy that is performed on the proximal part of the tibial tubercle in a dome-shaped 6,7.
We have used the medial opening wedge biplanar technique in this study as biplanar osteotomy has a V shape that has intrinsic stability which promotes bone healing 8,9,10. This increased biomechanical stability provides the use of short plate designs. There was no previous study that compared the rotational stabilities of the short and long plate fixation for medial opening wedge high tibial osteotomy in the current literature.
Materials and Methods
ParticipantsThis is an experimental biomechanical study. Six identical artificial left tibias were assigned to the two separate groups. The first group consisted of the subjects who had undergone medial opening wedge osteotomy fixed with short plates, and the second group with long plates.
12 artificial selbone left tibias were used in this study. The subjects had proper biomechanical properties with ISO-9001 and ISO-14001_en quality standards in Turkey.
ProcedureArtificial tibias (Selbone, Turkey) were rigidly fixed with the use of clamps. 2 parallel K wires are advanced from 3-5 cm distal part of the joint line, anterolaterally and posteromedially, aiming at the fibular head. Using the K wires as guides, osteotomy is performed with the use of an oscillating saw. The osteotomy is a biplanar osteotomy that is placed in the proximal part of the tibial tubercle, and 1 to 1.5 cm lateral cortex is preserved. After completing the osteotomy, two osteotomes are used for distraction to obtain an 8,5 mm gap. Keeping the gap, both short and long plates are placed in the proper position on the bone. Short placed are fixed with the use of 3 proximal and two distal screws, and long plates are fixed with the use of 3 proximal and three distal screws (Figure 1a-f).
Load-bearing tests are performed in the TOBB ETU experimental lab with the use of the Instron 5944 device in Ankara/Turkey. The artificial tibia had undergone proximal and distal compression for evaluation of the resistance against torsional forces after the fixation of the osteotomy. Fracture resistance against internal and external torsional forces was investigated in correlation with daily life (Figure 2a-c).
The breaking curve of short and long plate against maximum torque is shown respectively (Figure 3).
Maximum torque, yield torque, stiffness torque, and angle values were calculated and compared for both the short and long plate groups.
Statistical analysesIBM SPSS 25.0 was used for statistical analysis of the data. The results were evaluated with a 95% confidence interval and with a significance of p<0,05. Normal distribution of the data means standard deviation, minimal, and maximal analyses were performed. The normal distribution of the variables was assessed with Skewness. Kurtosis values and Kolmogorov-Smirnov tests. Mann Whitney U test was used for the comparison of the groups.
Ethical ApprovalThis study was approved by the decision of the Ethics Committee of Health Sciences University. The Declaration of Helsinki protocol was followed in the research protocol (Date: 2019-11-22, No: 2019/2173).
Results
Maximum torque, yield torque, stiffness torque, and angle values for the short plate are presented in Table 1. The values for the short plate were as follows: Max Torque 16.16±1.58, Yield Torque 10.46±1.95, Stiffness 0.40±.04, Torque 3.33±76.44, Angle63.63±109.33, and Time 28.83±6.96. Maximum torque, yield torque, stiffness torque, and angle values for the long plate are presented in Table 2. The values for the long plate were as follows: Max Torque 19.71±4.17, Yield Torque 11.95±3.13, Stiffness. .45±.08, Torque 19.66±31.93, Angle -20.77±54.26, and Time 29.33±7. A comparison of the groups is presented in Table 3. There was no statistically significant difference between the groups regarding the rotational stability, which was evaluated by Max Torque, Yield Torque, stiffness, and angle time parameters. The use of a long plate for the fixation resulted in skin irritation in the distal part of the plate and a bigger incision with a longer time of surgery.
Discussion
The biplanar medial opening wedge osteotomy is the preferred technique in this study as it has less rate of complications, providing more gap without involvement of the lateral cortex 11,12,13. Additionally, since the tibial tubercle is spared, the decrease in the tibial slope and patella alta, as well as patellofemoral arthrosis, are prevented in the biplanar medial opening wedge technique 14,15. The resistance of the fixation of osteotomies with long (HTO plate -Trumed-Turkey) and the short (OWO HTO plate-TST-Turkey) HTO plates against torsional forces are evaluated and compared in this study. Tommofix and Puddu plates have been widely used in the fixation of osteotomies, and there are many comparative clinical and biomechanical studies in the literature on those plates 16. In a biomechanical study, it is reported that fixed locking long plates were more durable and provided more primary stability 17. However, rotational stability was not assessed. Our study is unique as it is the only study that evaluated the resistance against torsional forces in biplanar osteotomy fixation.
Radiologic comparison of single and dual plane osteotomy for the treatment of medial compartment osteoarthritis revealed that single plane osteotomy resulted in a decrease of the patellar index rate and an increase in posterior tibial slope, whereas biplanar osteotomy lacked those changes 11. A comparative study on biplanar and mono- planar osteotomy revealed that biplanar osteotomy could provide a bigger gap and more angular correction than uniplanar osteotomy 11. Sphanah et al. reported that the bi-planar technique decreased the rate of lateral cortical hinge fractures. Still, in cases with gaps greater than 12,5 mm, the risk of fractures of the lateral tibial plate is increased and, in such cases, if the preoperative planning suggests more gap distance is required, both long and short plates should be ready, and the proper implant should be preferred for fixation 18,19. Lateral hinge fracture is reported to decrease the stability, causing delayed union of the fracture, and long plates are reported to have provided better stability in the case of lateral hinge fractures. We did not have any subjects with lateral wedge fractures in this study. Even though long plates are required in lateral wedge fractures, short plates have had more satisfactory outcomes for the patients as the long plates could be palpated under the skin, especially in slim patients 18. Long plates had better outcomes in terms of rigidity and stability in our study.
Studies comparing Puddu and Tomofix plates revealed more rigidity and stability for the Tomofix plates. Fu et al. reported that additional lateral fixation is required in patients with signs of instability of the lateral cortical edge with Puddu plates. This study reported insufficient stability against torsional forces with Puddu plates, but it may be caused by the non-locking cancellous screws used in that study. We have used locking 6,5 mm cancellous locking screws, and we have advanced the screw up to the edge of the lateral cortex, which may have contributed to the stability 20.
Na et al. reported that screws that are as long as 90% of the width of the proximal tibial plate could achieve stable fixation as strong as the bi-cortical screws. Whereas if the screw is smaller than 55% of the plate, it could impair the mechanical and axial stability in medial opening wedge osteotomy fixation with plate and locking screw 21. In our study length of the parallel screws is more than 90% of the plate. In a study that evaluated the outcomes of 20 patients who had undergone HTO with Puddu plates, the mean age was 49,4 at the time of surgery, and in the 2nd-year postoperative Kysholm and HSS scores were excellent, and in the following mean, 8,3 years period, 70% went on with their native knees, and 25% had total knee replacement 22,23,24,25. We have used small plates that had comparable biomechanical properties to the Puddu plate. The small plates which are used in our study had 3 6,7 mm screw holes and a locking option up to 15 degrees in different directions which may have provided extra stability for fixation.
Limitations
One of the most important limitations of our study is that we have used only an artificial tibia, which lacked the fibula and tibiofibular ligaments, the absence of which could affect the mechanical properties of the experiment mechanism. Another limitation is that the gap created for correction of the deformity is exactly 8,5 mm, and when bigger gaps are required, it may result in different outcomes. Also, we use tests only on the torsional stability in this study without evaluating the axial and mechanical stability.
Conclusion
In conclusion, there was no statistically significant difference regarding torsional forces between the groups. Longer plating resulted in skin irritation in the distal part of the plate and a bigger incision with a longer time of surgery. We suggest the use of short plates in HTO with biplanar osteotomy as short plate yielded similar biomechanical properties in terms of torsional forces.
Declarations
Ethics Declarations
This study was approved by the Ethics Committee of Health Sciences University (Date: 2019- 11-22, No: 2019/2173)
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or compareable ethical standards.
Data Availability
The data supporting the findings of this article are available from the corresponding author upon reasonable request, due to privacy and ethical restrictions. The corresponding author has committed to share the de-identified data with qualified researchers after confirmation of the necessary ethical or institutional approvals. Requests for data access should be directed to bmp.eqco@gmail.com
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content including study design, data collection, analysis and interpretation, writing, some of the main line, or all of the preparation and scientific review of the contents and approval of the final version of the article.
References
-
Kull C, Martin R, Rossel JB, Nguyen A, Albrecht E. Femoral vs sciatic nerve block to provide analgesia after medial open wedge high tibial osteotomy in the setting of multimodal analgesia: A randomized, controlled, single-blinded trial. J Clin Anesth. 2023;93(12):1-9.
-
Tanifuji O, Mochizuki T, Koga Y, Tanabe Y, Kawashima H. Biomechanical effect of fibular osteotomy on the knee joint in high tibial osteotomy: a cadaveric study. Biomed Mater Eng. 2023;34(2):123-31.
-
Kurz E, Brehme K, Bartels T, Pyschik M, Jenz M, Kadler W, et al. Standing steadiness and asymmetry after high tibial osteotomy surgery: A 2-year follow-up study. J Pers Med. 2022;12(10):1-9.
-
Pilone C, Rosso F, Cottino U, Rossi R, Bonasia DE. Lateral opening wedge distal femoral osteotomy for lateral compartment arthrosis/overload. Clin Sports Med. 2019;38(3):351-9.
-
Matsubara S, Onodera T, Iwasaki K, Hishimura R, Matsuoka M, Kondo E, et al. Discrepancy in the distribution patterns of subchondral bone density across the ankle joint after medial opening-wedge and lateral closing-wedge high tibial osteotomy. Am J Sports Med. 2022;50(2):478-85.
-
Abraham E, Toby D, Welborn MC, Helder CW, Murphy A. New single-stage double osteotomy for late-presenting infantile tibia vara: a comprehensive approach. J Pediatr Orthop. 2019;39(5):247-56.
-
Beslikas T, Christodoulou A, Chytas A, Gigis I, Christoforidis J. Genu recurvatum deformity in a child due to Salter Harris Type V fracture of the proximal tibial physis treated with high tibial dome osteotomy. Case Rep Orthop. 2012;2012:1-7.
-
Lauwers R, van Beek N, Goossens D, Claes S, Bartholomeeusen S, Claes T. Clinical and radiological outcomes of medial opening-wedge monoplanar and biplanar high tibial osteotomy using a triangular allograft impaction technique: a retrospective single centre study. Knee. 2023;44(7):21-30.
-
Jiao S, Qin S, Wang Z, Guo Y, Xu H, Liu Z, et al. [Correction of tibial multiplanar deformities using single Taylor external fixator combined with biplanar osteotomy]. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2023;37(7):839-45.
-
Wu Z, Yuan D, Hua D, Yang L, Zou Q, Tian X, et al. Precise patellar tendon insertion protection and osteotomy surface advantage of transtibial tuberosity-high tibial osteotomy. Orthop Surg. 2023;15(2):639-47.
-
Turkmen F, Kacira BK, Ozkaya M, Erkocak OF, Acar MA, Ozer M, et al. Comparison of monoplanar versus biplanar medial opening-wedge high tibial osteotomy techniques for preventing lateral cortex fracture. Knee Surg Sports Traumatol Arthrosc. 2017;25(9):2914-20.
-
Jo IH, Lee OS, Lee SH, Kim KW, Lee YS. Retro-tubercular gap widening can be caused by inappropriate anterior osteotomy and large opening gap in the medial biplanar open-wedge HTO. Knee Surg Sports Traumatol Arthrosc. 2019;27(9):2910-6.
-
Yildirim C, Demirel M, Ekinci M, Ozturk S, Bozdag E. Biomechanical comparison of uniplanar versus biplanar lateral opening-wedge distal femoral osteotomy techniques in terms of risk for medial hinge fracture. J Knee Surg. 2023;37(9):623-30.
-
Qiao Y, Ye Z, Zhang X, Xu X, Xu C, Li Y, et al. Effect of lower extremity torsion on clinical outcomes after medial patellofemoral ligament reconstruction and tibial tubercle transfer for recurrent patellofemoral instability. Am J Sports Med. 2023;51(9):2374-82.
-
Parikh SN, Rajdev N. Patients with bilateral patellar instability have multiple and symmetric risk factors in each knee. Knee Surg Sports Traumatol Arthrosc. 2023;31(12):5299- 305.
-
Ahmed AM, Addosooki A, Saleh Sleem A, Said E. Superior survivorship and plate-related results of TomoFix compared to Puddu plate fixation for opening-wedge high tibial osteotomy: A systematic review of the literature. Knee. 2023;42(3):1-18.
-
Gordon K, Winkler M, Hofstadter T, Dorn U, Augat P. Managing Vancouver B1 fractures by cerclage system compared to locking plate fixation - a biomechanical study. Injury. 2016;47(2):51-7.
-
Kang KT, Koh YG, Lee JA, Lee JJ, Kwon SK. Biomechanical effect of a lateral hinge fracture for a medial opening wedge high tibial osteotomy: Finite element study. J Orthop Surg Res. 2020;15(1):63.
-
Spahn G. Complications in high tibial (medial opening wedge) osteotomy. Arch Orthop Trauma Surg. 2004;124(10):649-53.
-
Fu D, Li G, Chen K, Zhao Y, Hua Y, Cai Z. Comparison of high tibial osteotomy and unicompartmental knee arthroplasty in the treatment of unicompartmental osteoarthritis: a meta-analysis. J Arthroplasty. 2013;28(5):759-65.
-
Ebraheim NA, Sabry FF, Haman SP. Open reduction and internal fixation of 117 tibial plateau fractures. Orthopedics. 2004;27(12):1281-7.
-
Erquicia J, Gelber PE, Perelli S, Ibanez F, Ibanez M, Pelfort X, et al. Biplane opening wedge high tibial osteotomy with a distal tuberosity osteotomy, radiological and clinical analysis with minimum follow-up of 2 years. J Exp Orthop. 2019;6(1):10.
-
Tuncay I, Bilsel K, Elmadag M, Erkocak OF, Asci M, Sen C. Evaluation of mobile bearing unicompartmental knee arthroplasty, opening wedge, and dome-type high tibial osteotomies for knee arthritis. Acta Orthop Traumatol Turc. 2015;49(3):280-7.
-
Jing L, Liu K, Wang X, Wang X, Li Z, Zhang X, et al. Second-look arthroscopic findings after medial open-wedge high tibial osteotomy combined with all-inside repair of medial meniscus posterior root tears. J Orthop Surg (Hong Kong). 2020;28(1):1-10.
-
Diffo Kaze A, Maas S, Waldmann D, Zilian A, Dueck K, Pape D. Biomechanical properties of five different currently used implants for open-wedge high tibial osteotomy. J Exp Orthop. 2015;2(1):14-23.
Figures
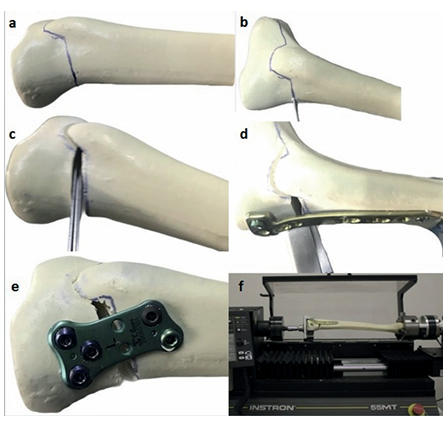
Figure 1. a. Before starting the osteotomy procedure, determination of the osteotomy line. b. After determining the osteotomy line, advancement of 2 K wires and osteotomy of the tibia with osteotomes. c. Completion and distraction of the osteotomy line after the cut with the help of osteotomes. d. Fixation with a long plate after the osteotomy. e. Fixation with a short plate after the osteotomy. f. Placement of the artificial tibia for evaluation of the torsional forces
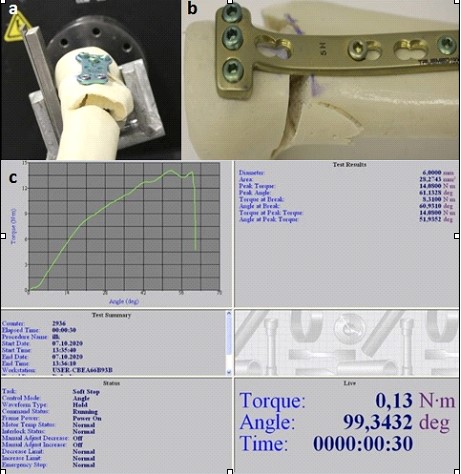
Figure 2. a. Fracture curve of short plate versus maximum torque. b. View of short plate breaking moment against maximum rotational torque. c. View of short plate breaking against maximum rotational torque
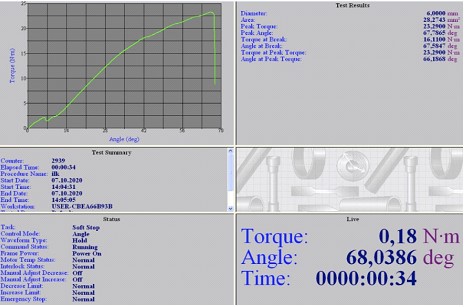
Figure 3. Breaking the curve of the short and long plate against the maximum torque
Tables
Table 1. Distribution of Max Torque, Yield Torque, Stiffness, Time, Torque, Angle Scores of the Short Plate
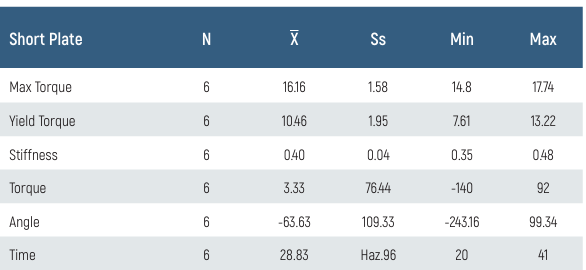
Table 2. Distribution of Max Torque, Yield Torque, Stiffness, Time, Torque, Angle Scores of Long Plate
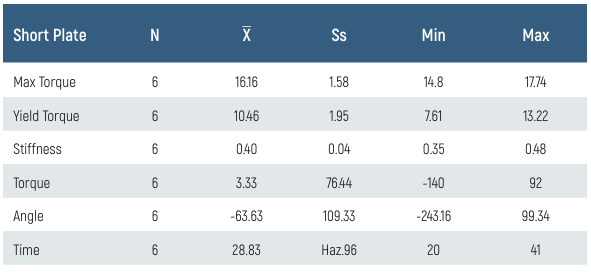
Table 3. Comparison of Max Torque, Yield Torque, Stiffness, Time, Torque, and Angle Scores According to the characteristics of the plaques (n: 12)
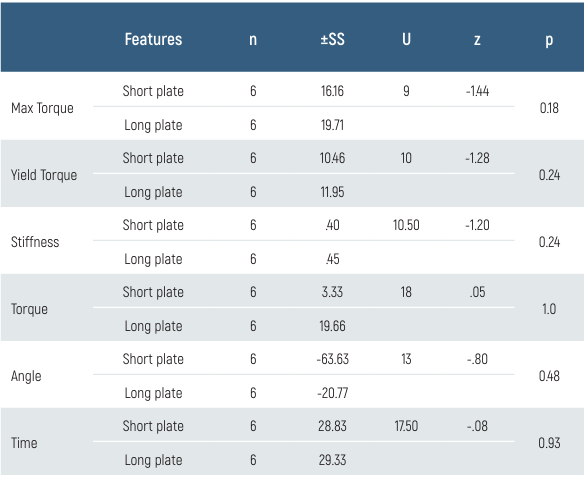
p>0.05, U/Z: Mann Whitney U test
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Ahmet Saray, Faik Türkmen, Fatma Kübra Erbay Elibol, Murat Topal, Turgut Emre Erdem, Teyfik Demir. Biomechanical comparison of rotational stability of long and short plates in fixation of high tibial osteotomies in the surgical treatment of osteoarthritis. Eu Clin Anal Med 2024;12(Suppl 1):S19-22
- Received:
- September 12, 2024
- Accepted:
- October 15, 2024
- Published Online:
- October 15, 2024
- Printed:
- October 20, 2024