Left lower quadrant pain in a patient with situs inversus totalis: acute appendicitis
Appendicitis in left lower quadrant pain
Authors
Abstract
Introduction One of the most common reasons for emergency service admissions is abdominal pain. One of these is acute appendicitis. Situs inversus totalis (SIT) is a rare genetic anomaly characterized by the transposition of the organs in the abdomen and thorax in a mirror image.
Case PresentationIn situs inversus totalis and intestinal malrotation, it is seen that the appendix is located on the left, as in other organs. We aimed to discuss a case diagnosed with situs inversus totalis and acute appendicitis and underwent a laparoscopic appendectomy in light of the literature. A 42-year-old male patient was admitted to the emergency department with left lower quadrant pain. Laparoscopic appendectomy was performed on the detection of situs inversus totalis and acute appendicitis as a result of physical examination and imaging.
Conclusion Rare clinical conditions such as appendicitis should be considered in cases with left lower quadrant pain and situs inversus totalis and should be included in the differential diagnosis. Early diagnosis is important as life-threatening complications may develop.
Keywords
Introduction
One of the most common reasons for admissions to the emergency department is abdominal pain (4-8%). The most common reason for surgical intervention in patients presenting with abdominal pain is acute appendicitis. While the diagnosis cannot be made in 24-41% of the patients, the rate of misdiagnosis has been reported in 30%.1,2 Situs inversus totalis (SIT) is a rare genetic anomaly characterized by the transposition of the organs in the abdomen and thorax in a mirror image. In situs inversus totalis and intestinal malrotation, it is seen that the appendix is located on the left, as in other organs. Also, situs inversus totalis is present in 50% of patients with Kartagener’s Syndrome.3 In this presentation, we aimed to present our case of acute appendicitis with situs inversus totalis is presented that we treated in our clinic in the light of the literature.
Case Presentation
A 42-year-old male patient was admitted to the emergency department with a complaint of abdominal pain that started in the periumbilical area before and localized in the left lower quadrant 6 hours after it started. Nausea and loss of appetite accompanied his anamnesis. The patient had no additional disease. There was tenderness and rebound in the left lower quadrant of the abdomen. In the laboratory, the leukocyte was 9210 / mm3, C-reactive protein was 93 mg / L. His Alvarado score was 6. On abdominal tomography (CT), the liver was located on the left, and the spleen was on the right. Situs inversus totalis was observed in the patient. The appendix diameter was 7 mm in the left lower quadrant, and inflammation was observed in the surrounding mesentery. Findings were consistent with acute appendicitis. With these findings, the case was diagnosed with SIT and acute appendicitis. The patient and his family were informed about the diagnosis of SIT, along with acute appendicitis. They stated that the patient and the family were not aware of SIT. After the necessary medical information was given to the patient and his relatives and their written consents were obtained, he was taken to surgery. The abdomen was entered with a 10 mm trocar from the navel, 10 mm from the right lower quadrant, and 5 mm from the suprapubic area. Laparoscopic appendectomy was performed with the help of 3 ports. The patient was discharged on the first postoperative day without any problem. Histological evaluation was reported following acute appendicitis.
Ethical ApprovalThis study was approved by the Ethics Committee of Necmettin Erbakan University for Non-Drug and Non-Medical Device Research (Date: 2024- 10-18, No: 2024/5279).
Reporting GuidelinesThis case is reported in accordance with the CARE guidelines.
Discussion
Situs inversus is a pathology with an unclear etiology seen at a rate of 0.001% -0.01% and does not include organ dysfunction. It is called partial if it concerns only the thoracic or abdominal organs and total if it includes both cavities. Situs inversus totalis (SIT) occurs when the embryonic middle intestine rotates 270 degrees clockwise while it should turn counterclockwise.1] Thus, all visceral organs in the thorax and abdomen are located symmetrically to the midline of the position they should be, that is, all thoracic and abdominal visceral structures are located in a mirror image of the normal position concerning the midline. In this case, the appendix is also located in the left lower quadrant.4 The association rate of left lower quadrant appendicitis and situs inversus totalis in all cases of appendicitis is 0.016%.5 In our case, the cause of left lower quadrant pain was acute appendicitis in a patient with situs inversus totalis.
Other causes of acute abdomen characterized by left lower quadrant pain should be considered in the differential diagnosis. Diseases causing left lower quadrant pain include bowel obstruction, sigmoid diverticulitis, incarcerated or strangulated hernia, amyand hernia, colitis, psoas abscess, gynecological causes (such as ovarian tumors and cysts, adnexal torsion, ruptured ectopic pregnancy, pelvic inflammatory disease) and acute situs inversus appendicitis.1,6 The fact that the patient’s pain is outside the left lower quadrant is related to the central nervous system not participating in general transposition.4 In our case, the patient’s pain was localized in the left lower quadrant.
The appendectomy approach in patients with situs inversus is performed with the same technique as the appendicitis approach in the normal position. Laparoscopic or open methods can be applied, as in our case. Laparoscopic appendectomy was performed for the first time by Contini in 1998 in the case of totalis with situs inversus. It is also available in the literature that trocars can be placed differently.7 In our clinic, we routinely perform laparoscopic appendectomy with three ports. Since our patient had situs inversus totalis, we entered the port, which we normally enter from the left lower quadrant and the right lower quadrant. Other ports were entered at their normal places (Figure 1).
Limitations
The main limitation of this study is that it represents a single case report. Therefore, the findings cannot be generalized. However, it highlights the importance of considering situs inversus totalis in the differential diagnosis of left lower quadrant abdominal pain.
Conclusion
In cases with situs inversus totalis, if the person does not know this situation, as in our case, it will be difficult to diagnose appendicitis because the appendix is located in an abnormal location. The most important way to prevent complications that may occur is to make use of anamnesis, physical examination, and imaging tests. On physical examination, the heart crest is on the right, heart sounds are more pronounced on the right than on the left, and the liver is palpable on the left, suggesting SIT. The presence of dextrocardia and gastric fundus gas on the right side on direct radiographs is in favor of SIT (Figure 2).
Electrocardiographic findings are helpful in the diagnosis of dextrocardia. Computed tomography of the abdomen is useful in the differential diagnosis of intestinal malrotation and situs inversus totalis and has an accuracy rate of 90-98% in the diagnosis of acute appendicitis.[8] In our case, it was thought that there might be diverticulitis at first, but when it was found out by tomography that it was situs inversus totalis, a diagnosis of acute appendicitis was made. The most common reason for surgical intervention in patients presenting with abdominal pain is acute appendicitis. It should be kept in mind that rare clinical conditions such as appendicitis may be present in patients with situs inversus totalis presenting with left lower quadrant pain. Early diagnosis is important as life-threatening complications may develop.
Declarations
Ethics Declarations
Ethical approval for this study was obtained from the Ethics Committee of Necmettin Erbakan University for Non-Drug and Non-Medical Device Research (Date: 2024-10-18, No: 2024/5279).
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or compareable ethical standards.
Informed Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content including study design, data collection, analysis and interpretation, writing, some of the main line, or all of the preparation and scientific review of the contents and approval of the final version of the article.
Abbreviations
CT: Computed Tomography
SIT: Situs Inversus Totalis
References
-
Liu Y, Wu L, Chen Y, Li D, Jiang J, Zhong W et al. Delayed diagnosis of abdominal pain in patient with situs inversus totalis in emergency department: a case report. Medicine (Baltimore). 2017;96(49):e9028.
-
Buluş H, Akyürek Ö, Akbal E, Doğan M, Koyuncu A. The clinical significance of calcium and serum phosphate in patients with acute appendicitis. Selcuk Med J. 2015;31(4):355-357.
-
Boendermaker AE, Coolsma CW, Emous M, Avest E. Efficacy of scheduled return visits for emergency department patients with non-specific abdominal pain Emerg Med J. 2018;35:499-506.
-
Oh JS, Kim KW, Cho HJ. Left-sided appendicitis in a patient with situs inversus totalis. J Korean Surg Soc. 2012;83:175-178.
-
Al-Jumaily M, Achab M, Hoche F. Laparoscopic cholecystectomy in situs inversus totalis: Is it safe? J Laparoendosc Adv Surg Tech A. 2001;11:229-231.
-
Sabuncuoğlu MZ, Çakır T, Benzin MF, Çelik G, Sabuncuoğlu A. A rare association in the inguinal region: incarcerated hernia and acute appendicitis. Selcuk Med J. 2016;32(1):23-24.
-
Gupta N, Goyal P, Bansal I, Li S, Kumar Y, Baijal SS. Modified palliative biliary stenting in situs inversus totalis patient with carcinoma gallbladder: Feasibility and technical details. Transl Gastroenterol Hepatol. 2017;2:27.
-
Akbulut S, Caliskan A, Ekin A, Yagmur Y. Left-sided acute appendicitis with situs inversus totalis: review of 63 published cases and report of two cases. J Gastrointest Surg. 2010;14:1422-1428.
Figures
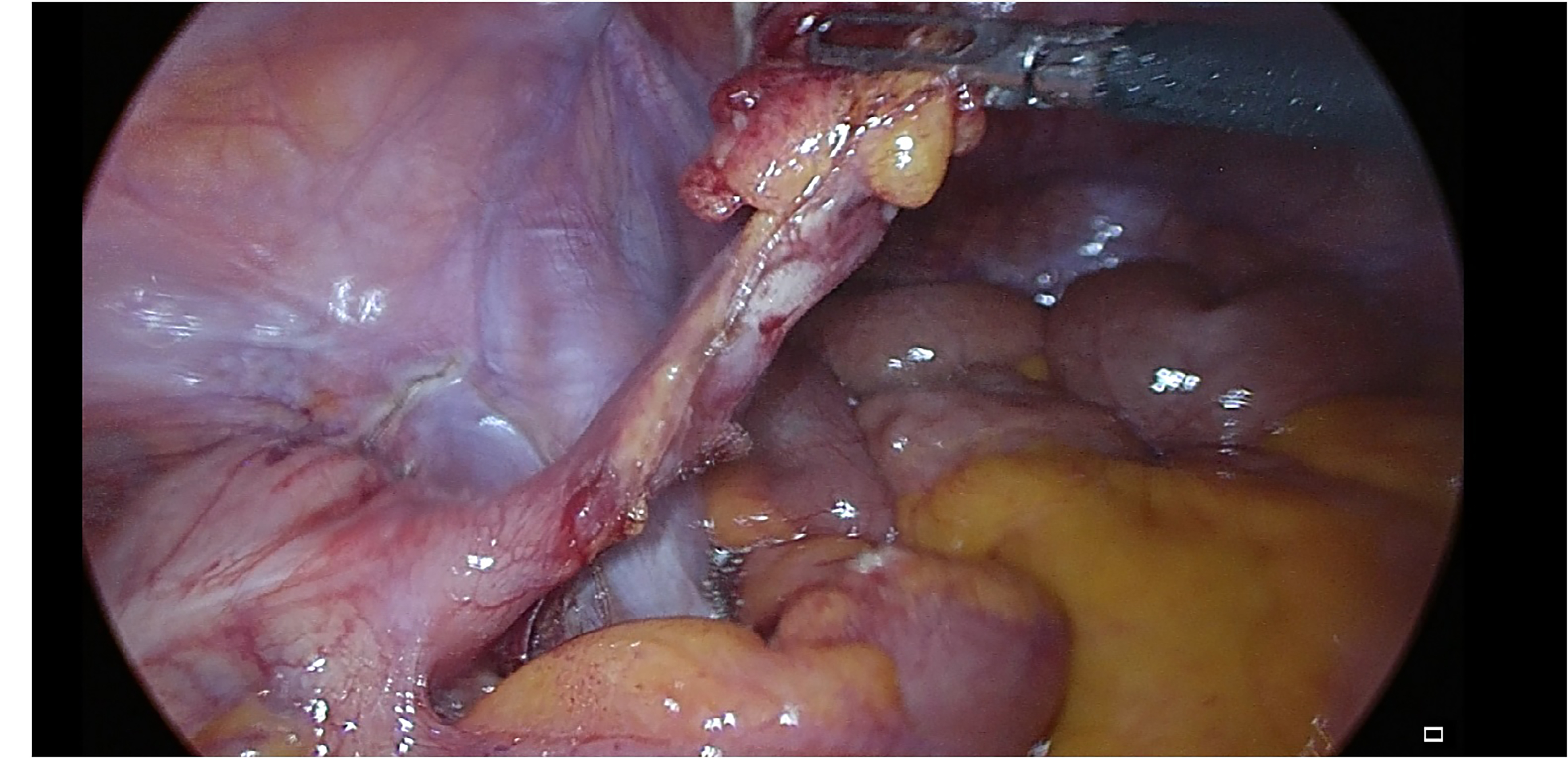
Figure 1. Intraoperative view of the appendix
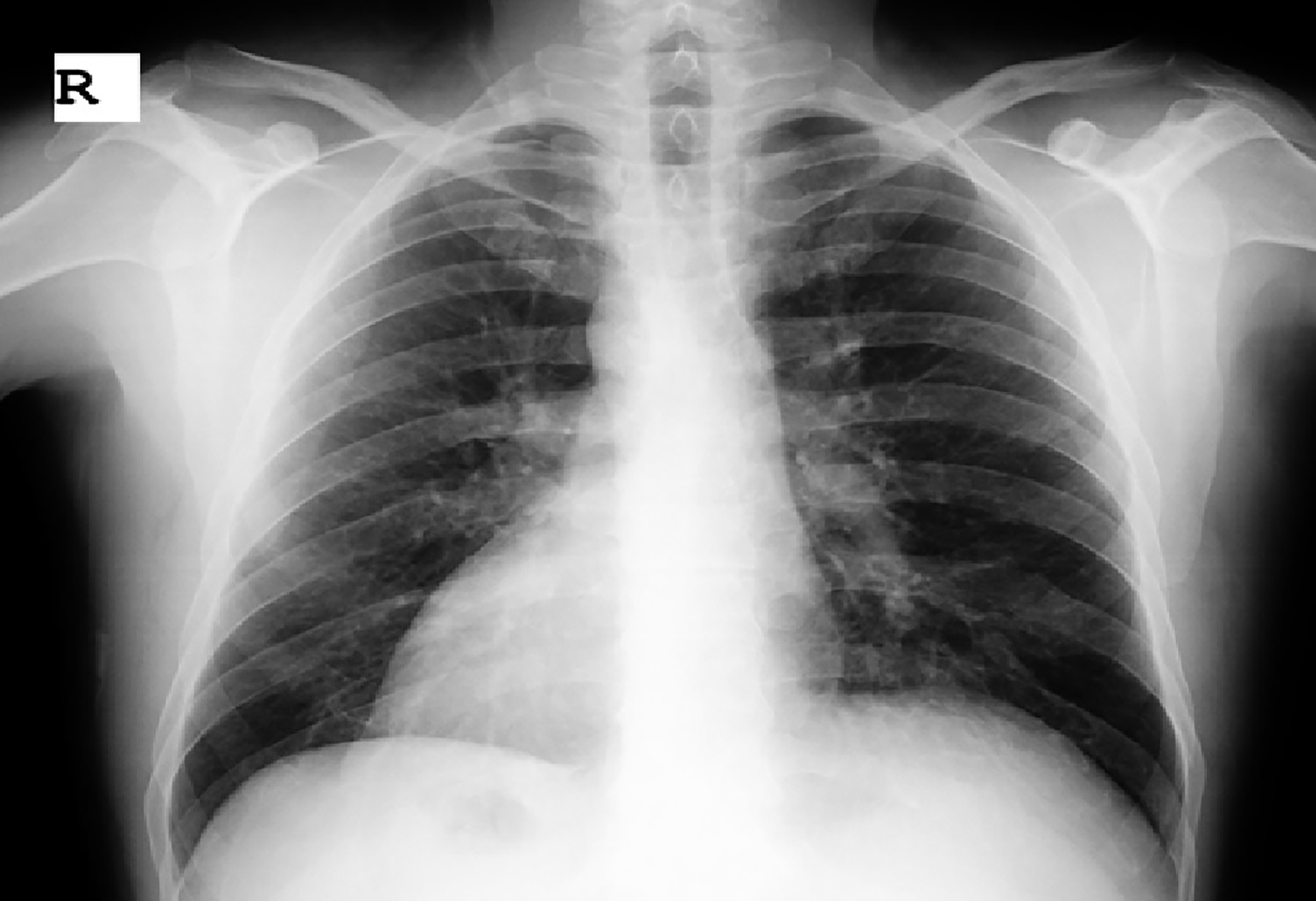
Figure 2. X-ray view of the heart and fundus gas
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Arslan Hasan Kocamaz, Ömer Kişi, Abdulkadir Çelik, Abdullah Gürhan Duyan. Left lower quadrant pain in the patient with situs inversus totalis; Acute appendicitis. Eu Clin Anal Med 2025;13(1):20-22
- Received:
- September 27, 2024
- Accepted:
- November 10, 2024
- Published Online:
- November 20, 2024
- Printed:
- January 1, 2025